
Abstract
Pseudohypoparathyroidism is a terminology used to describe a group of metabolic disorders characterized by parathyroid hormone resistance. Patients with pseudohypoparathyroidism have hypocalcemia, hyperphosphatemia, and elevated serum parathyroid hormone. This methylation defect leads to signaling abnormalities in the parathyroid hormone and parathyroid hormone-related peptide receptor. We present a 40-year-old African American male who was referred to our endocrinology clinic for hypocalcemia. On physical examination, his body mass index was 34.3 kg/m2 and he was found to have a round face, and several subcutaneous nodules on his scalp, hands, and legs. Laboratory findings revealed hypocalcemia, hyperphosphatemia, and elevated levels of intact parathyroid hormone and thyroid stimulating hormone (TSH). His hand X-ray showed brachydactyly of all metacarpal bones, and soft tissue calcifications. Brain CT indicated dense calcifications in the subcortical region, bilateral basal ganglia, bilateral thalami, bilateral cerebellum and vermis, and soft tissue calcifications in the scalp. The “inactivating parathyroid hormone/parathyroid hormone-related peptide signaling disorder” diagnostic approach suggested by the Euro pseudohypoparathyroidism network was applied to the patient, who was diagnosed with parathyroid hormone signaling disorder. Compared to the old pseudohypoparathyroidism classification and the 2018 Pseudohypoparathyroidism International Consensus Statement Report, the inactivating parathyroid hormone/parathyroid hormone-related peptide signaling disorder cluster classification appears to be more flexible, and easier to use. It also accommodates future inclusion of genetic mutations associated with hormonal signaling disorders. Adoption of the inactivating parathyroid hormone/parathyroid hormone-related peptide signaling disorder classification remains limited, and further larger studies are needed to compare the three approaches.
Keywords
Introduction
Pseudohypoparathyroidism (PHP) describes a group of metabolic disorders characterized by parathyroid hormone (PTH) resistance.1,2 PHP is associated with other hormonal disorders, such as those involving thyroid hormone, growth hormone, and gonadotropin. 3 PHP was first described in 1942 by an American endocrinologist, Fuller Albright, who reported a case of hypocalcemia and hyperphosphatemia associated with PTH resistance and unusual combination of developmental and skeletal defects that are collectively termed as Albright hereditary osteodystrophy (AHO).3,4 While the actual disease prevalence is unknown, one study has reported 3.4 cases per 1 million people.4,5
The 2018 PHP International Consensus Statement categorized PHP into PHP type 1a, type 1b, type 1c, type 2, pseudopseudohypoparathyroidism (PPHP), progressive osseous heteroplasia (POH), and acrodysostosis 6 ; this categorization is based on a constellation of clinical features, hormonal resistance, and confirmatory genetic testing. 6 GNAS gene mutation or methylation is responsible for the majority of the PHP disorders. 6 The EuroPHP network has recently proposed a new classification for this group of signaling disorders in 2016 that reflects the actual methylation defects in these diseases. 1
In this report, a case of hypocalcemia with PTH resistance is presented. Additionally, a comparison between the traditional PHP classification, 2018 PHP International Consensus Statement classification, and EuroPHP network classification was performed.2,3,6 This is a detailed case report for a previously published abstract. 7
Case report
A 40-year-old African American man was referred by an orthopedic surgeon to our endocrinology clinic for hypocalcemia treatment before right hip replacement for severe osteoarthritis. He had previously been told that he had hypocalcemia after a car accident, but he did not follow-up. He had chronic pain in both hips, which limited his daily activities; he could not flex his back, because of back and hip stiffness; he also had lumps in his head, arms, and legs, which he indicated were increasing in size and number. The patient had no other significant past medical history or other congenital problems, and his family history is negative for hypocalcemia; he had one elder sister, who was healthy. On physical examination, his body mass index was 34.3 kg/m2 and he was found to have a round face, and several subcutaneous nodules on his scalp, hands, and legs (Figure 1). His thyroid gland was not enlarged. He used a cane to walk; he could not sit on a chair because he was unable to flex his back; and he had a substantially limited range of motion in both hips.

Subcutaneous ossifications on the scalp and finger.
Laboratory findings indicated low calcium <5 mg/dL (reference range (RR): 8–10.6 mg/dL), low ionized calcium of 0.7 mmol/L (RR: 1.13–1.32 mmol/L), high phosphorus of 6.2 mg/dL (RR: 2.3–5 mg/dL), elevated alkaline phosphatase of 161 u/L (50–136 u/L), albumin of 3.7 g/dL (RR: 3.4–5.4 g/dL), GFR > 120 mL/min/1.73 m2 (RR: >60 mL/min/1.73 m2), elevated intact PTH of 327 pg/mL (RR: 15–69 pg/mL), elevated TSH of 11.7 mIU/L (RR: 0.5–4.5 mIU/L), FT4 of 1 ng/dL (RR: 0.82−1.77 ng/dL), and serum 25-hydroxy vitamin D 34 ng/mL (RR: >30 ng/mL). He had normal levels of follicular-stimulating hormone (FSH), lutenizing hormone (LH), testosterone, insulin-like growth factor 1 (IGF-1), and cortisol. His 24-hour urine calcium was low, at 86 mg/d (RR: 100–300 mg/d). GNAS gene analysis was not covered by the patient’s medical insurance. Hand X-ray revealed brachydactyly of all metacarpal bones and soft tissue calcifications (Figure 2).

X-ray of the left (a) and right (b) hands, showing brachydactyly and soft tissue calcifications.
A brain CT showed dense calcifications in the subcortical region, bilateral basal ganglia, bilateral thalami, bilateral cerebellum, and vermis, as well as soft tissue calcifications in the scalp with diffuse osteoporosis of the calvarium and skull base (Figure 3). A dual energy X-ray absorptiometry was requested but not approved by the patient’s medical insurance.

Brain CT showing: (a) and (b) soft tissue calcifications in the scalp; (c) bilateral subcortical calcifications (green arrows), bilateral basal ganglia calcifications (blue arrows) and bilateral thalami calcifications (orange arrows); (d) bilateral cerebellar calcifications (green arrows), and vermis calcifications (orange arrow).
The new signaling disorder approach suggested by The EuroPHP network was applied to the patient. 2 The patient was found to have three major criteria (PTH resistance, ectopic ossifications, brachydactyly) and three minor criteria (TSH resistance, obesity/overweight, flat nasal bridge and/or round face; Table 2).
Based on that, he was diagnosed with inactivating PTH/PTHrP signaling disorder (iPPSD); and treatment with calcitriol (0.25 µg every 12 h), calcium carbonate (1.2 g every 8 h), and levothyroxine (50 µg daily) was initiated.
When the patient was then followed up after 2 months; his level of activities and body aches had significantly improved; the calcitriol dose was gradually increased to 1.5 µg per day; and calcium carbonate was decreased to 1.2 g every 12 h. Six months following treatment, his calcium level increased to 7.6 mg/dL (RR: 8–10.6 mg/dL), albumin-adjusted calcium 7.8 mg/dL (RR: 8–10.6 mg/dL), intact PTH decreased to 90 pg/mL (RR: 15–69 pg/mL), phosphorus increased to 6.5 mg/dL (RR: 2.3–5 mg/dL), TSH decreased to 4.3 (RR: 0.5–4.5 mIU/L), and FT4 increased to 1.4 ng/dL (RR: 0.82−1.77 ng/dL). A written informed consent was obtained from the patient for publication purpose.
Discussion
The old PHP classification depends on the presence of AHO to differentiate PHP1A/PHP1C and PPHP from PHP1B3,8; features of AHO include brachydactyly, short stature, round face, subcutaneous ossifications, and stocky build.3,8 The second step involves differentiating between PHP1 and PPHP according to the hormonal resistance evidence.3,8 PHP2 can then be identified by testing for urinary cAMP levels in response to exogenous PTH injection.3,8 Gsα activity is subsequently measured to differentiate between PHP1A and PHP1C.3,8 Genetic testing can then be performed to determine mutation type. However, there is substantial overlap between categories in this classification 2 ; and the cost and availability of those tests also complicate a definitive diagnosis and classification. Moreover, the traditional PHP classification does not include other diseases with phenotypic or molecular similarities, such as chondrodysplasia and acrodysostosis.2,9
The EuroPHP network suggested a new name and classification for PHP in December of 2016, to overcome the drawbacks of the traditional pseudohypoparathyroidism approach. 2 This new approach suggests using the term “inactivating PTH/PTHrP signaling disorder” (iPPSD) to describe all diseases associated with this pathway 2 ; this terminology replaces “PHP,” which does not reflect the actual mechanism and biochemical changes in this group of disorders. The iPPSD approach considers the presence of physical features and biochemical tests and eliminates the need for measuring urinary cAMP (Table 1).
PHP classifications comparison.

AHO: Albright hereditary osteodystrophy, PHP: pseudohypoparathyroidism, iPPDS: inactivating PTH/PTHrP signaling disorder.
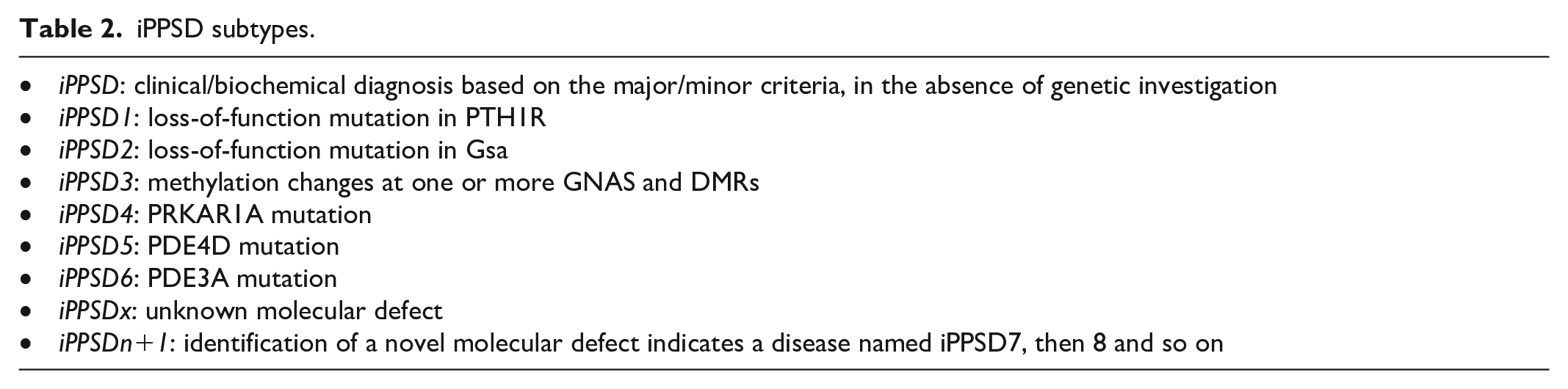
It includes other disease categories, such as POH, acrodystosis, and disorders associated with PTH receptor mutation (e.g., Blomstrand chondrodysplasia). 2 With the iPPDS approach, the diagnosis of a signaling disorder can be made through the application of major and minor criteria (Table 1). 2 The major criteria are more specific, and are comprised of PTH resistance, ectopic ossifications, and brachydactyly.2,10 The minor criteria are less specific, and are comprised of TSH resistance, other hormonal resistance, motor and cognitive retardation or impairment, intrauterine and postnatal growth retardation, obesity/overweight, and a flat nasal bridge and/or maxillary hypoplasia and/or a round face.2,11 The presence of a major criterion of either PTH resistance or ectopic ossifications, or the presence of the major criterion of brachydactyly with at least two minor criteria establishes a diagnosis of iPPSD.2,11 After diagnosis, a molecular analysis can be performed to further categorize the iPPSD subtype on the basis of common published genetic defects (Table 2). Even though the iPPSD classification eliminates the need for an exogenous PTH injection and provids a rapid, less expensive screening tool for high-risk families, this classification does not include the parental origin of the defect. 2
iPPSD subtypes.
The first International Consensus Statement Report (ICSR) about the diagnosis and management of PHP and related disorders was released in 2018. 6 The ICSR was developed by 37 participants from 13 countries and supported by nine European and international scientific societies 6 ; it includes an updated recommendation for the diagnosis and management of PHP. The ICSR committee proposed a primary clinical diagnosis for PHP-related disorders through major clinical and biochemical criteria (Table 1). Acrodysostosis was added to PHP disorders and the need for exogenous PTH administration was eliminated in the ICSR. The committee also suggest using additional clinical features to support the diagnosis, including endocrine, neurological, and mineralization manifestations. However, there is no details on how to apply these features to support the diagnosis. Notably, genetic testing is mandated following clinical diagnosis to confirm diagnosis and subtype determination of the disorder. 6
Compared to the ICSR, the iPPSD approach was found to be more organized and easier to use. Although the ICSR has modified the traditional PHP classification and provided criteria to diagnose PHP clinically, there is a lack of guidance on how to clinically combine and implement these criteria.
In the present case, the iPPSD diagnostic approach was applied to the patient, who was diagnosed with PTH signaling disorder. Genetic testing was not performed due to financial difficulties. He was treated with calcitriol and calcium supplementation. 7
Conclusion
Compared to the traditional PHP classification and ICSR, the iPPSD cluster classification appears to be more flexible, and easier to use. It also accommodates future inclusion of genetic mutations associated with hormonal signaling disorders. Adoption of the iPPSD classification remains limited, and further larger studies are needed to compare the three approaches.
Footnotes
Acknowledgements
Wael Taha, M.D, Assistant Professor, School of Medicine, Internal Medicine Department, Division of Endocrinology, Wayne State University, Detroit, USA.
Imam A, Taha W. SUN-502 from Pseudohypoparathyroidism to Signaling Disorder. J Endocr Soc. 2019 Apr 15;3(Supplement_1):SUN-502.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.