
Abstract
Breast carcinosarcoma, also known as metaplastic breast cancer, is one of the rarest types of breast cancer. It is an aggressive and poor prognostic breast cancer compared to triple-negative breast cancer. Due to the lack of specific and prescribed treatment, it could threaten patients’ lives, especially women worldwide. There are various diagnostic methods, such as multiple imaging and pathology methods, to diagnose breast cancers. Still, considering the common appearance characteristic of this type of breast cancer with other types, histopathology is the most definitive way. There is no standard neoadjuvant or adjuvant chemotherapy for this rare type of breast cancer. In this article, we reported the case of a 62-year-old female with a final diagnosis of metaplastic breast carcinoma and her surgical and medical treatment method.
Introduction
Breast cancer is the most common cancer among the female population that can threaten their lives and is increasing worldwide.1,2 Metaplastic Breast Cancer (MBC) is a rare and aggressive type of breast cancer that includes 0.2–5 % of all breast cancers. 3 This type of tumor heterogeneity, rarity, and lack of standard therapeutic approach makes MBC aggressive and a poorer prognostic than other types of breast cancer. 4 The histological feature of this malignancy is the differentiation of neoplastic epithelium to at least two different cell types, especially squamous epithelium and/or mesenchymal components such as spindle, chondroid, osseous, or rhabdoid cells.4,5 Most of this type of malignancy (MBC) is typically a triple-negative breast cancer, meaning estrogen, progesterone, and human epidermal growth factor 2 receptors’ expression is lacking in the tumor. Unfortunately, this type has shorter survival, twice the risk of recurrence, and a poor prognosis compared to metaplastic TNBC.3,6,7 On the other hand, as MBC has many resembling features with invasive ductal carcinoma and benign lesions on mammography, its diagnosis is complicated. 8
So, it can be concluded that it is crucial to do more clinical trials and research to improve the accuracy of diagnostic and treatment methods. In this article, we report a rare case of metaplastic carcinoma in a 62-year-old female, which was diagnosed by core needle biopsy.
Case presentation
A 62-year-old-woman was admitted to the surgical clinic for a palpable mass of the right breast, which was found during a self-physical examination 6 months ago in February 2023. Her past medical history was unremarkable. During the physical examination, an irregularly shaped, deep, dense, immobile mass measuring approximately 6 × 4 cm was palpable in the upper outer quadrant of the right breast near the axilla area, which was fixed to the pectoralis major. The skin of the breast was normal in appearance without erythema and redness, but the axillary lymph nodes were not palpable, and the nipple was inverted (Figure 1). The patient was admitted to the surgical ward and was asked to do a mammography for more investigation in the first step. Mammography demonstrated a high-density mass with irregularity of margin. On the other hand, the skin of the right breast was thick and edematous without calcification. Ultrasonography was conducted for more investigation, and the result showed an irregular mass with adhesion to the pectoralis major muscle and was highly suspicious of malignancy. Core needle biopsy was performed, and the histopathological examination revealed sarcoma of the breast. Diagnosing microscopic tissue showed that the tumor contained carcinomatous and sarcomatous elements. The epithelial component was dominant, while the mesenchymal cellular structure was evaluated at less than 10%, and the carcinomatous part of the tumor possessed ductal (Figures 2 and 3). The histologic grade of the mass was III. Ki67 proliferation index was 48% which means positive. P53 of the tumor cells was positive, and c-erbB-B2 was positive too.

Inverted nipple in metaplastic breast cancer.
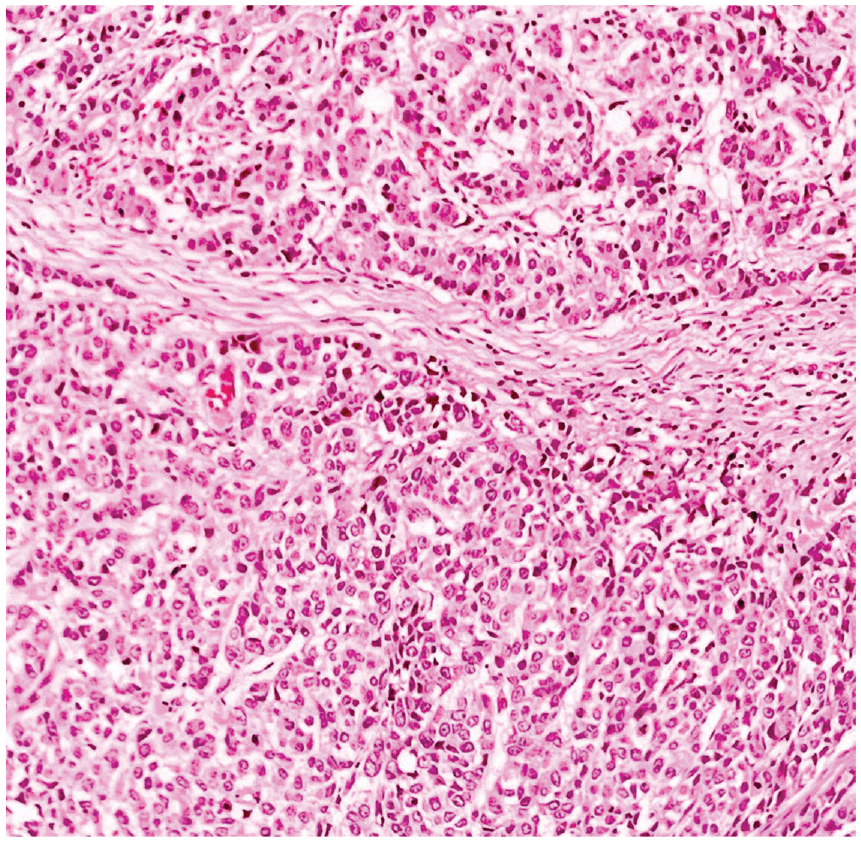
Microscopic view of metaplastic breast cancer.

Microscopic view of metaplastic breast cancer.
The blood tests analyzed presented leukocytosis (white blood cells (WBC) = 14,200 g/dL with a neutrophilia ratio of 78%) but other factors were in normal range.
A positron emission tomography (PET) scan was performed for the patient due to the suspicion of metastasis, and the results were unrevealing.
Due to the pathology report, open surgery was performed. The patient underwent wide radical excision with modified mastectomy due to the adhesion of the mass to the right pectoralis major muscle. Also, the axillary lymph nodes were removed for further investigation. The mass and the pectoralis major muscle were removed with a safe and wide margin (Figures 4 and 5), two drains were installed, and the surgical wound was closed (Figure 6).

Modified radical mastectomy process.

Metaplastic breast cancer tumor with pectoralis muscle.

Modified radical mastectomy and axilla dissection in MBC patient.
Macroscopically, the cut surface shows the tumor and pectorals major muscle. The maximal tumor diameter was approximately at 8 cm with a primarily brownish appearance. The mass did not infiltrate the skin or the surrounding lymph nodes.
She had an uneventful recovery and was transferred to the department of surgery. After 2 days, she was transferred to the oncology department to receive chemotherapy. She was administered 10 cycles of a combination of cyclophosphamide and Epirubicin as adjuvant chemotherapy. Drains were removed after 5 days. Finally on the postoperative day 7, she was discharged.
The final pathology report demonstrates metaplastic carcinoma with mesenchymal differentiation, also known as carcinosarcoma, as a diagnosis with skeletal muscle involvement but without skin and nipple involvement, lymphovascular invasion, and lymph nodes involvement (all six lymph nodes were examined). Ductal carcinoma in situ was not identified. The histological grade was III (Nuclear pleomorphism: score 3, Miotic rate: score 3, Glandular/Tubular differentiation: score 3. So, the overall grade was III), and the pathological staging identified pT3, N0. On the other hand, fibrocystic changes and ductal ectasia were found. (ICD-0, C50.9)
The patient is doing well after 6 months of follow-up after adjuvant therapy. She was asked to do left breast mammography for a follow-up investigation, which revealed nothing.
Discussion
Carcinosarcoma of the breast, also known as metaplastic or biphasic metaplastic, or metaplastic sarcomatoid carcinoma, is a rare and aggressive type of breast cancer that includes 0.2%–5 % of all breast cancers.5,9 This type of breast cancer is more aggressive and poor prognostic than others because of heterogeneity, diverse histology, and rarity. On the other hand, no targeted treatment way and approach exists for breast carcinosarcoma. 4
Studies have shown that the 5-year survival rate of MBC is approximately 49%, and the age of most reported cases was between 33 and 74 years old.10,11 Factors affecting the patients’ survival rate with MBC are tumor size of more than 5 cm, lymph node involvement, high Ki-67 > 14%, and distant metastasis. On the other hand, skin involvement, being in a younger age group, and lymph node metastasis could increase the probability of local recurrence and distant metastasis and lead to poor prognosis.10,12 According to the study by Ullah et al. age of more than 60 years, grade IV tumors, tumor size more than 50 mm, and brain metastasis could affect patients’ survival rate and increase patients’ mortality rate. 13
Breast carcinosarcoma usually shaped solid, well-defined, nodular, and firm tumors. 14 It is a malignant tumor, especially a large tumor, which could lead to skin and/or chest wall fixation, nipple retraction, skin redness, erythema, and ulceration. 15
Based on the latest classification of WHO for breast cancer tumors, metaplastic carcinoma (MC) is divided into five different subtypes: Low-grade adenosquamous carcinoma, fibromatosis-like metaplastic carcinoma, squamous cell carcinoma, spindle cell carcinoma, and metaplastic carcinoma with mesenchymal. Although metaplastic carcinoma shows different and separated invasive breast cancer differentiation into squamous or mesenchymal-looking components, including spindle, chondroid, osseous, and rhabdoid cells, but it is not just limited to them, MC could mix with other types of usual carcinoma, and this feature makes it have a poorer prognosis than other breast cancer types. 16 Most MBC is typically a triple-negative breast cancer, meaning estrogen receptor, progesterone receptor, and human epidermal growth factor 2 (HER-2) receptor expression is lacking in the tumor. Still, this type is poor prognostic than other types of triple-negative breast tumors. 17
Different imaging methods exist to diagnose breast tumors, such as ultrasonography, mammography, MRI, and PET scans. 2 The first step is using ultrasonography and mammography, and MRI and PET scans, if available, could improve the quality and accuracy of the diagnosis. 8 Although using these methods is not sufficient to diagnose metaplastic breast carcinoma because of the similarity of shape features to other breast tumors, it could be helpful to determine the approximate size and location of the tumor or reveal the distance of metastasis.18,19 Histopathological methods such as pre-surgery core needle biopsy or pathological review of frozen sections during surgery could help diagnose MBC. However, due to its poorly differentiated characteristics, making an accurate diagnosis of carcinosarcoma of the breast is complex and challenging. 15
There is no standard and targeted treatment strategy for breast carcinosarcoma yet, and treatments that are currently being performed are similar to those for invasive ductal carcinoma. 14 Most carcinosarcoma breast cases are triple negative, so hormonal therapy is rarely conducted for their treatment. 12 Surgery is one of the most important parts of the treatment in patients with metaplastic breast carcinoma. The surgery method used in patients like ours with skeletal muscle involvement is MRM (Modified Radical Mastectomy) with axillary dissection, particularly for patients with T2 or higher stage of the disease. 20 Some medical centers conduct radiotherapy and/ or chemotherapy to improve patients’ treatment, but some studies revealed that these methods do not help control or recurrence inhibiting.21,22 Also, the patient refused to do one-step nucleic acid amplification due to his personal concerns.
As it mentioned before, there is no standard treatment method for MBC. Various studies have been conducted to investigate the effect of neoadjuvant chemotherapy (NAC) on MBC prognosis, such as the studies by Haque et al., 23 Wong et al., 24 and Al-Hilli et al., 25 all of them demonstrate that MBC is poorly responsive to NAC. Studies conducted by He et al. 26 and Moreno et al. 27 showed that chemotherapy could improve the survival outcomes in MBC patients but the study conducted by Lan et al. 28 demonstrated that chemotherapy did not improve patients’ survival rate for operable patients and recommended to avoid chemotherapy as an overtreatment for those patients. So, it can be concluded that there are different points of view about the effect of using NAC or adjuvant chemotherapy on patients’ survival rates. In one of the most extensive studies conducted recently by Ullah et al. 13 the results show that the simultaneous use of surgery, radiotherapy, and chemotherapy, compared to the use of each of them alone or the combination of two methods, can increase patients’ survival rate.
In our case, A 62-year-old female diagnosed with a breast tumor was admitted to the surgical ward. Medical investigation revealed the suspicious malignant tumor, and finally, the patients underwent MRM and axillary dissection with a diagnosis of metaplastic carcinoma, which was proven by pre-surgery core needle biopsy. The surgery team decided to perform this operation because the pathological reports and the growth rate had grown rapidly within 6 months. The post-surgery pathology report confirms the core needle biopsy diagnosis. Although some studies showed that adjuvant chemotherapy’s benefit is not yet proven, our team decided to refer the patient to the oncology department. They finally decided to start 10 cycles of a combination of cyclophosphamide and Epirubicin as adjuvant chemotherapy based on the beneficial results of some studies that have used this compound to treat these patients.20,29
Conclusion
MBC is one of the most aggressive and rare types of breast cancer that threatens patients’ lives worldwide, especially women. Although there is no standard treatment method for MBC, different studies show the positive effect of using a combination of surgery; the technique depends on the surgical team and the patient’s condition, radiotherapy, and adjuvant chemotherapy. On the other hand, several studies demonstrate that neoadjuvant chemotherapy has no useful effect on MBC patients.
Footnotes
Acknowledgements
None.
Author contributions
All authors contributed equally to the article and read and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.