
Abstract
Pyogenic granuloma or lobular capillary hemangioma is a vascular proliferation of the skin and mucosal surface, most commonly in the oral or nasal cavity. To the best of our knowledge, a few cases of auricular pyogenic granuloma were published in the literature. In our case, a 14-year-old female complained of a recurrent pyogenic granuloma in the external auditory canal that regressed successfully with the oral beta-blocker treatment.
Introduction
Pyogenic granuloma (PG), also known as lobular capillary hemangioma, is a benign vascular tumor arising from the skin and mucosal surface of the oral and nasal cavities. 1 The lesions appear as solitary, well circumscribed, smooth, erythematous nodules that bleed easily. 2 The cause of PG is uncertain, but it may be related to trauma, infections, and hormonal influences.1,2 It can be treated with surgical excision, electrocautery, cryotherapy, silver nitrate cautery, and beta-blockers.2–4 Here, we report a rare case of recurrent PG arising from the external auditory canal (EAC). The lesion showed a complete response to the beta-blocker treatment without any recurrence after a follow-up for a year.
Case report
A 14-year-old female came to the clinic due to severe ear pain, otorrhea, mild hearing loss, and the sensation of a foreign body in her right ear for the past 2 months. She had no history of ear trauma or surgery and had not taken any medication. Physical examination showed a solitary, red, and soft mass in the right EAC, measuring 10 × 12 mm (Figure 1). Histopathology examination showed a proliferation of small blood vessels that arranged in a lobular pattern with an inflammatory infiltration confirming the diagnosis of PG (Figure 2). Based on the clinical and histological examination, no further investigation was needed. Two previous treatment attempts with electrocautery and cryotherapy with a subsequent recurrence were recorded (Figure 3). The lesion was resected completely under general anesthesia, and amoxicillin-clavulanic acid antibiotic (1g twice daily for 10 days) was administered. Post-intervention follow-up showed recurrence 2 months afterward (Figure 4). Silver nitrate (AgNO3) cautery was applied three times over 10 days, but the lesion reappeared after 6 weeks (Figure 5). The co-treatment for a month of silver nitrate cautery and a beta-blocker (3.125 mg PO carvedilol twice daily for 2 weeks, increased to 6.25 mg twice daily for the next 2 weeks) was performed (Figure 6). Subsequent follow-up for a year confirmed complete lesion healing.

First presentation of pyogenic granuloma in the right ear.
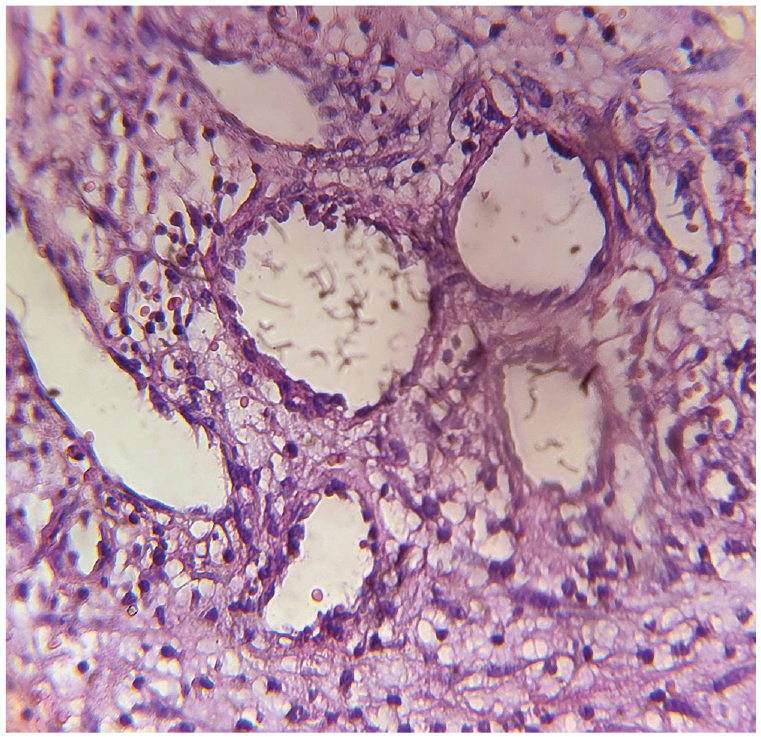
Histological examination shows a vascular proliferation arranged in a lobular pattern with inflammation.

First recurrence after electrocautery and cryotherapy.

Second recurrence after surgical excision.

Third recurrence after silver nitrate cautery.

Healing after beta-blocker with a session of silver nitrate cautery.
Discussion
PG is a benign vascular tumor that appears as a solitary and smooth nodule in the skin and mucosal surface of the head and neck, especially in the oral and nasal mucous membranes.1,2 The most common sites of PG in the oral cavity include gingiva (83%), lip (5.3%), tongue (5.3%), palate (4.5%), and buccal mucosa (0.8%). 1 PG occurs rarely in EAC, larynx, and urethra.1,3–5 It happens commonly in the second decade of life, and many factors like infections, pregnancy, and hormonal influences can predispose to PG development.1,2 Medication such as retinoids, antiretrovirals, and antineoplastic drugs are other accused factors. 3 Few cases of PG without traumatic injury or a history of immune disorder have been reported. 4 Differential diagnosis of PG includes hemangioma, glomus tumors, granulation tissue, and amelanotic melanoma. 5
PG can be treated by electrocautery, cryotherapy, laser ablation, surgical excision, silver nitrate cautery, imiquimod, and beta-blockers.2–4 Posttreatment recurrence of PG is common,2,6,7 with an estimated rate of 16% after the simple excision. 8 The most common site of recurrent PG is the gingival. 8 Accused factors of PG recurrence include blunt excision, repetitive trauma, viral oncogenes, pregnant women due to hormonal influences, and microscopic arteriovenous malformation. 8 In addition, angiopoietin 1, 2, and ephrin b2 agents in vascular tumors play a role in PG recurrence. 8 However, complete surgical excision is associated with the lowest recurrence rate (2.94%). 6 The difficulties accompanied by the blunt removal of PG from the narrow EAC increase the probability of its recurrence.6,7 In our case, although the PG in the external auditory canal was excised deeply to the perichondrium, it reappeared after 2 months. The treatment with oral beta-blockers led to complete lesion remission.
Oral and topical beta-blockers are considered the most effective treatments for many cutaneous lesions, like infantile hemangioma, Kaposi sarcoma, wounds, ulcers, and other vascular lesions. 9 PG, like hemangioma, has beta-adrenergic receptors.9,10 Beta-blockers inhibit vascular endothelial growth factor and basic fibroblast growth factor, leading to reduced angiogenesis, inducing vasoconstriction, and stimulating apoptosis of endothelial cells. 9 Small PG, especially in children, was managed preferably with beta-blockers.9,10 A few cases of PG in EAC have been reported in the literature.4–7 One case of recurrent PG in the external ear canal was reported in a 28-year-old man with a lesion size of 35 mm. 7 It was excised partially under local anesthesia with subsequent recurrence after 3 weeks. Complete excision down to the conchal perichondrium under general anesthesia showed no further relapses during a follow-up period of a year. In this case, we present a 14-year-old female with a recurrent PG in the EAC, despite the various applied treatment methods, including complete excision with electrocautery, cryotherapy, and silver nitrate. The treatment with oral beta-blockers led to lesion healing with no further recurrence.
Conclusion
In conclusion, complete resection of the PG is the preferable initial intervention, which ensures lesion healing without recurrence. However, beta-blockers are also an effective alternative intervention that prevents further recurrences.
Footnotes
Acknowledgements
None.
Author contributions
O.A.s: Writing – original draft; writing – review and editing. I.B.: Writing – original draft; Writing – original draft; O.A.d: Writing – original draft; writing – review and editing. T.D.: Conceptualization; supervision; writing – review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Patient consent
Written Informed Consent was obtained from the legally authorized representative of the minor subject for the publication of this case report.