
Abstract
Objectives:
Atrial fibrillation after surgery is associated with increased rates of heart failure and ischemic stroke, and extension of hospitalization. Bisoprolol is a β-blocker used to reduce heart rate and manage arrhythmias during atrial fibrillation. However, the safety and efficacy of bisoprolol transdermal patch treatment in patients with postoperative atrial fibrillation remain unclear.
Methods:
We retrospectively assessed the electronic health records of our hospital between September 2013 and July 2018 and identified patients with postoperative atrial fibrillation who had been treated with a bisoprolol transdermal patch. We excluded patients with sinus rhythm using bisoprolol transdermal patch to prevent atrial fibrillation recurrence and those with sustained atrial fibrillation before surgery. Data on heart rhythm, heart rate, and blood pressure at the baseline and after 24 h of treatment were obtained from the electronic health records.
Results:
Of the 603 patients treated with the bisoprolol transdermal patch, 61 patients with postoperative atrial fibrillation after noncardiac surgery were included. The bisoprolol transdermal patch was discontinued due to bradycardia in two patients (3.3%). In both cases, the heart rate increased after the removal of the bisoprolol transdermal patch and no additional treatment was necessary. Among the 61 patients, sinus rhythm was restored within 24 h of bisoprolol treatment in 47 patients (77.0%). The heart rate significantly decreased from 124.8 ± 26.3 bpm at the baseline to 78.9 ± 16.6 bpm at 24 h after treatment (p < 0.001). There were no significant differences in the systolic and diastolic blood pressures between patients before and at 24 h after treatment.
Conclusion:
The results of this study indicate that the bisoprolol transdermal patch is well tolerated and effective in patients with atrial fibrillation after noncardiac surgery.
Keywords
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia during the postoperative period. Postoperative AF (POAF) occurs in approximately 3% of patients after noncardiac surgery. 1 In patients who undergo noncardiac thoracic surgery, the rate of POAF is considerably higher (30%) than that in patients subjected to other types of noncardiac surgery. 2 The causes of POAF are still unclear; sympathetic nerve hyperactivation due to stress during surgery may be a contributing factor. 2 The development of POAF increases the short- and long-term risks of ischemic stroke and heart failure, rate of mortality rate, and length of hospitalization.3–5
In hemodynamically stable patients with POAF, the heart rate control strategy (i.e. to reduce heart rate) is a viable option for initial treatment.6,7 Intravenous administration of β-blockers, non-dihydropyridine calcium-channel blockers, or digoxin is recommended for heart rate control. Moreover, in asymptomatic or mildly symptomatic patients, rate control agents can be orally administered. However, oral administration immediately after surgery might not be the best option, especially after a gastrointestinal surgery.
Bisoprolol is a β-blocker available as a transdermal formulation in Japan. Recently, bisoprolol transdermal patch has been reported to be effective and safe for the treatment of AF tachycardia.8,9 However, the safety and efficacy of the bisoprolol transdermal patch in patients with POAF remain unclear. In this study, we primarily aimed to evaluate the safety of bisoprolol transdermal patch treatment in patients with POAF after noncardiac surgery. For this purpose, we examined the discontinuation of bisoprolol transdermal patch treatment due to adverse effects within 24 h of its use. We also aimed to evaluate the effect of bisoprolol transdermal patch treatment in patients with POAF after noncardiac surgery. Therefore, we examined the rate of sinus conversion at 24 h after treatment and heart rate at the baseline and 24 h after treatment.
Methods
Study population
This study was approved by the Osaka International Cancer Institute Ethics Committee. The need for informed consent was waived because of the retrospective nature of this study. An opt-out approach was used with the disclosure of our institute website. We retrospectively assessed the electronic health records of patients in our hospital between September 2013 and July 2018 and identified 603 patients who had been treated with Bisono® tape (Toa Eiyo Ltd., Tokyo, Japan), a bisoprolol transdermal patch. The inclusion criterion was the occurrence of POAF after noncardiac surgery treated with a bisoprolol transdermal patch. The exclusion criterion was preventive use of the bisoprolol transdermal patch in patients with sinus rhythm and in those with sustained AF before surgery.
Data collection
Data on age, sex, comorbidities, AF history, preoperative medication use, concomitant use of antiarrhythmic drugs, and surgery type were collected for all patients. To evaluate the safety of the bisoprolol transdermal patch in patients with POAF, we obtained data related to drug discontinuation due to adverse effects within 24 h. Moreover, information on heart rhythm, heart rate, and blood pressure at the baseline and 24 h after treatment was collected from the electronic health records.
Statistical analysis
Categorical variables are presented as n (%). Continuous variables are presented as median (interquartile range). The paired t-test was used to compare the measurements obtained at 24 h with those at the baseline. A logistic regression analysis was performed to evaluate the association between concomitantly used antiarrhythmic drugs and sinus rhythm recovery. All statistical analyses were performed using JMP® software (version 13.2; SAS Institute Inc., Cary, NC, USA). A p value of <0.05 indicated statistical significance.
Results
Among the 603 patients, 127 patients were administered the bisoprolol transdermal patch to treat POAF after noncardiac surgery. We excluded 66 patients who used the bisoprolol transdermal patch after sinus rhythm conversion to prevent AF recurrence. We also excluded patients with sustained AF before surgery. The final sample included 61 patients who had received the bisoprolol transdermal patch treatment for AF after noncardiac surgery (Figure 1). Eleven patients (18.0%) had a history of AF (Table 1). Ultra-short-acting β-blockers were used by 16 patients (26.2%) prior to the administration of the bisoprolol transdermal patch. Non-dihydropyridine calcium-channel blockers, digoxin, and other antiarrhythmic drugs were concomitantly used with the bisoprolol transdermal patch by 27 (44.3%), 7 (11.5%), and 15 (24.6%) patients, respectively. Class III antiarrhythmic drugs, such as amiodarone, were not used by any patient.

Study workflow and patient inclusion and exclusion criteria.
Characteristics of the patients and procedures.
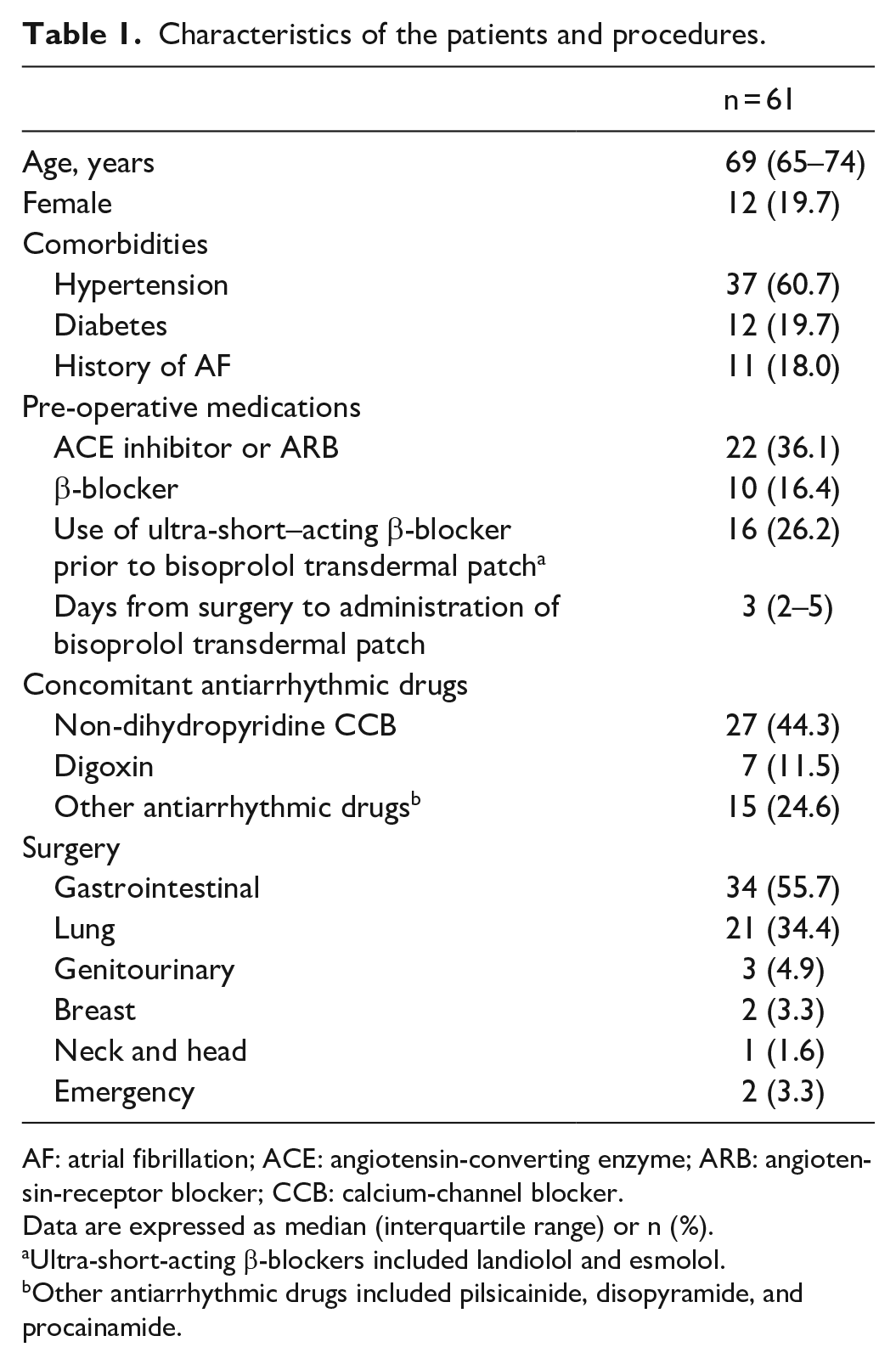
AF: atrial fibrillation; ACE: angiotensin-converting enzyme; ARB: angiotensin-receptor blocker; CCB: calcium-channel blocker.
Data are expressed as median (interquartile range) or n (%).
Ultra-short-acting β-blockers included landiolol and esmolol.
Other antiarrhythmic drugs included pilsicainide, disopyramide, and procainamide.
Two patients (3.3%) discontinued bisoprolol transdermal patch because of sinus bradycardia without evident symptoms. In these patients, the heart rate recovered to 50–70 bpm spontaneously after the removal of bisoprolol transdermal patch. Other adverse effects such as hypotension, atrioventricular block, and bronchospasm were not observed in any patient. The other four patients shortly discontinued the use of the bisoprolol transdermal patch because of conversion from AF to sinus rhythm (n = 1), achievement of optimal heart rate (n = 1), and switch to oral bisoprolol (n = 2).
Among the 61 patients, 47 (77.0%) were in sinus rhythm at 24 h after treatment. There was no significant association between calcium-channel blockers and digoxin and sinus rhythm recovery; however, the use of calcium-channel blocker had the tendency to increase the rate of sinus rhythm recovery (odds ratio, 3.68; 95% confidence interval (CI), 0.85–15.9, p = 0.081) (Table 2). The heart rate significantly decreased from 124.8 ± 26.3 bpm at the baseline to 78.9 ± 16.6 bpm at 24 h after treatment (p < 0.001) (Figure 2(a)). There were no significant differences in the systolic blood pressure (122.6 ± 20.4 vs 122.5 ± 17.3 mmHg, p = 0.97) and diastolic blood pressure (73.1 ± 14.5 vs 70.5 ± 12.7 mmHg, p = 0.15) before and at 24 h after treatment (Figure 2(b) and (c)).
Association between other antiarrhythmic agents and sinus rhythm recovery.

CI: confidence interval.
Odds ratios were estimated by logistic regression analysis.
Antiarrhythmic drugs included pilsicainide, disopyramide, and procainamide.
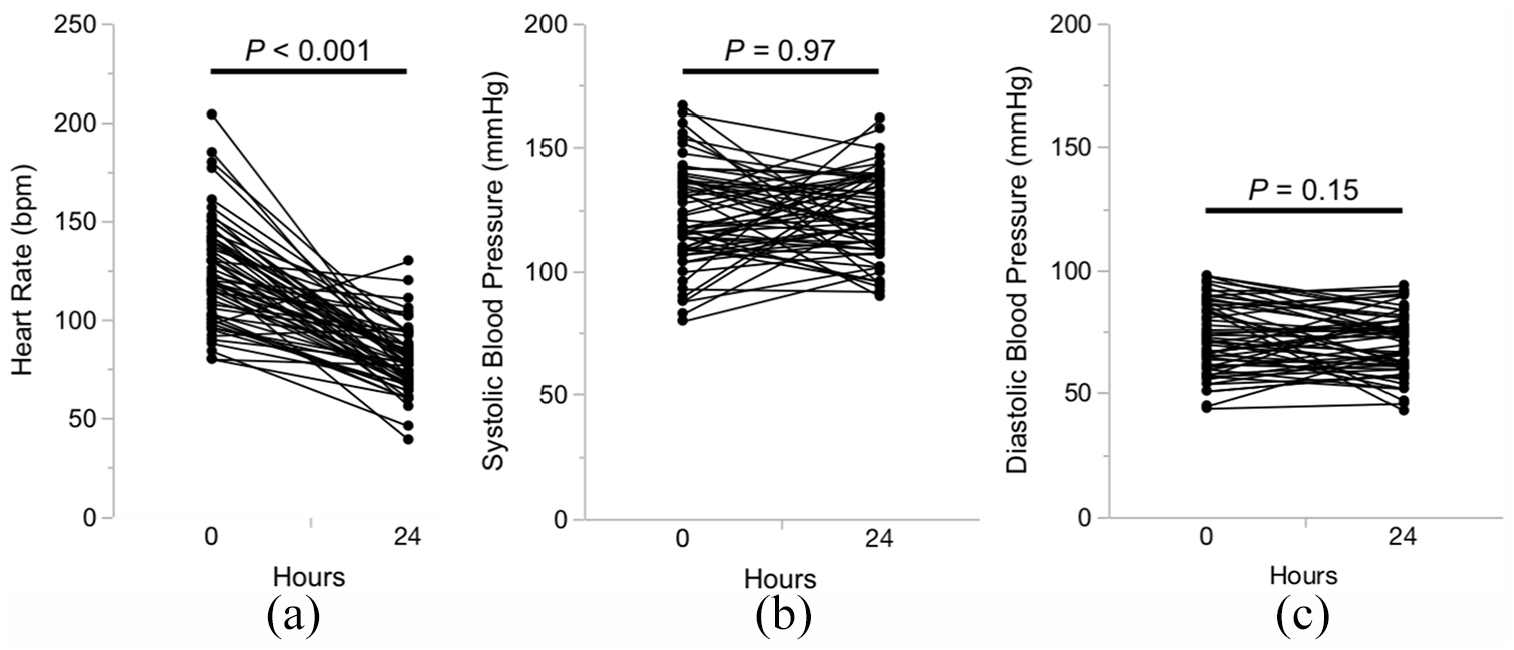
(a) Changes in the heart rate, (b) systolic blood pressure, and (c) diastolic blood pressure from the baseline to 24 h after the administration of bisoprolol transdermal patch in patients with postoperative atrial fibrillation after noncardiac surgery.
Discussion
In the present study, we investigated the safety and efficacy of the bisoprolol transdermal patch in patients with POAF after noncardiac surgery. The bisoprolol transdermal patch treatment for POAF reduced the incidence of discontinuation associated with adverse events, increased the conversion rate to sinus rhythm, and significantly decreased the heart rate in patients with POAF at 24 h after treatment. These results indicated that the bisoprolol transdermal patch is safe and effective for POAF after noncardiac surgery.
The bisoprolol transdermal patch has unique features associated with the cutaneous absorption pathway and pharmacokinetics of bisoprolol. Unlike oral bisoprolol, the bisoprolol transdermal patch leads to a slow increase in drug concentrations in the blood and maintenance of stable concentrations, 10 which may contribute to its safety and stable effects. The bisoprolol transdermal patch can be used in patients for whom oral administration is difficult. Oral administration of rate control agents can be used in patients with asymptomatic or mildly symptomatic POAF who can take medicines orally, unlike patients who have undergone gastrointestinal surgery, or during the immediate postoperative period. In our study, 55.7% of patients underwent gastrointestinal surgery, and the median time from surgery to administration of the bisoprolol transdermal patch was 3 days. In such patients, the bisoprolol transdermal patch may be an optimal option for POAF management.
Bisoprolol is a β1 adrenergic receptor-selective β-blocker and has negative chronotropic and inotropic effects. In this study, the bisoprolol transdermal patch was discontinued due to sinus bradycardia in two patients (3.3%), although systolic and diastolic blood pressure values were not affected. A previous study reported that the prevalence of bradycardia in patients treated with the intravenous ultra-short-acting β-blocker landiolol and the calcium-channel blocker diltiazem to manage AF after cardiac surgery was 0% and 11.1%, respectively; 11 however, our study indicated the clinical safety and usability of the bisoprolol transdermal patch for POAF. Sinus bradycardia observed during the bisoprolol transdermal patch treatment period was resolved after its removal without additional treatment to maintain the heart rate (e.g. atropine, catecholamine, and temporary cardiac pacing), which suggests the controllability of the bisoprolol transdermal patch.
The pathophysiology of POAF is not well understood; however, the activation of the sympathetic system is thought to contribute to the onset and persistence of POAF.2,11 β-Blockers can control excessive sympathetic activity and may be effective for achieving conversion to sinus rhythm and reducing the heart rate. Our study further revealed a high rate (77.0%) of conversion from AF to sinus rhythm, almost similar to that reported in previous studies on the intravenous administration of ultra-short-acting β-blockers (landiolol and esmolol), in which these drugs were reported to be more effective than diltiazem in the management of POAF.11–13
Although our findings indicate the safety and efficacy of the bisoprolol transdermal patch treatment, there were some limitations to this study that do not allow a definitive evaluation of the treatment. First, this was a single-center retrospective study, which may have led to selection bias. Second, we did not include a control group. The effect of the bisoprolol transdermal patch could be overestimated, because we also found that some patients with POAF converted from AF to sinus rhythm spontaneously without the bisoprolol transdermal patch. This indicates the possibility that spontaneous conversion patients without the bisoprolol transdermal patch were included among the 77.0% of patients who were treated with the bisoprolol transdermal patch. Prospective studies with control groups are necessary to validate our findings. Finally, antiarrhythmic agents were concomitantly used in more than half of the patients in this study. We could not completely isolate the effects of the bisoprolol transdermal patch from those of other antiarrhythmic agents. Regardless of these limitations, our data indicate that the bisoprolol transdermal patch can be considered an optimal treatment option for POAF. Prospective randomized controlled study is required to validate the safety and efficacy of the bisoprolol transdermal patch in patients with POAF.
Conclusion
Bisoprolol transdermal patch treatment is safe and efficacious for patients with POAF after noncardiac surgery and can be a promising option to control POAF clinically.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Osaka International Cancer Institute Ethics Committee (approval number: 18063).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
As this was retrospective study, the need for informed consent was waived by the Osaka International Cancer Institute Ethics Committee. An opt-out approach was used with disclosure of our institute website.