
Abstract
Little awareness persists of how pregnancy worsens cardiac diseases. We wish to highlight the challenges in managing pulmonary hypertension (PH) in pregnancy, within low socioeconomic environments. A 31-year-old G3P1A1 of 5 months gestation presented with worsening dyspnea and extremital edema. She had a history of heart disease with no cardiologist follow-up. She was diagnosed with type I/II PH at 4 months gestation. Her ultrasound revealed intrauterine fetal death (IUFD). She was referred for pregnancy termination. At presentation, she was tachypneic with SaO2 at 68%. After labor, she was transferred to a cardiac intensive care unit with SaO2 at 60%. Bedside echocardiography revealed a high probability of PH (pulmonary artery systolic pressure value: 109 mmHg). Unfortunately, she deteriorated and passed away a day later. Cardiac diseases in pregnancy contribute significantly to maternal mortality in Indonesia and other low socioeconomic countries. Traditional views on pregnancy and family and human rights advocate pregnancy as one of the rights, pregnancy complicated with cardiac diseases is detrimental and potentially lethal. Disparities in healthcare practices and low socioeconomic environments also contribute to such outcomes. Lack of awareness and improperly held beliefs on conception and family have led women to conceive amidst severe underlying cardiac diseases with dire outcomes.
Introduction
Pulmonary hypertension (PH) is a contraindication of pregnancy due to its significant mortality rate. Little awareness of cardiac diseases in pregnancy is unfortunately prevalent among Indonesians. Thus, PH in pregnancy often presents late in Indonesia, contributing to our continuously rising maternal mortality rate. A combination of societal, cultural, and demographic factors contributes to the ever-present issue. A previous study reported that 70% of the population with moderate- to high-risk cardiovascular disease failed to access cardiovascular care. 1
Health system-wise, the Indonesian healthcare system is not yet designed to provide a one-stop holistic management of cardiac diseases in pregnancy. There is a big difference between evidence-based medicine and on-field practice. The number of consultants capable of providing quality care is dwarfed by the number of various cardiac diseases in the community.1,2 This case report wishes to highlight the case, its optimal management, an in-depth consideration of human rights, and current disparities in health care regarding reproduction and the shortcomings unique to developing countries such as Indonesia and low socioeconomic status.
Case presentation
A 31-year-old G3P1A1 of 24 weeks of gestation presented to our emergency unit with worsening dyspnea for 1 week. The dyspnea did not improve with resting. She complained of edema in her extremities, which had gotten increasingly pale and bluish.
On her history, she was diagnosed with reduced ejection fraction 3 years ago. She admitted poor compliance with scant cardiology follow-ups. At 4 months gestation, she was referred to a cardiologist for worsening dyspnea and her left ventricular ejection fraction was 74% with a high probability of PH. She was admitted to the intensive care unit due to type I/II cardiogenic PH. She improved on furosemide, digoxin, and sildenafil. No fetal heartbeat was noted upon discharge. She was referred to our facility for pregnancy termination.
At presentation, she was not in labor and she was alert and tachypneic (RR 30×/min). Her oxygen saturation peaked at 60% on room air and 68% with 15 L/min oxygen supplementation. Cardiomegaly and murmur in the lower left sternal border were found with the Carvallo sign present (increase in systolic murmur of tricuspid regurgitation during inspiration). 3 Further examination revealed she was 20–22 weeks pregnant. The bimanual examination revealed no signs of labor.
Laboratory results revealed hyponatremia and metabolic alkalosis from arterial blood gas analysis (pH 7.478; pCO2 21.3, pO2: 17.1, HCO3 15.9, tCO2 16.6) with negative base excess (−5) and oxygen saturation at 30.3%. Chest X-ray revealed cardiomegaly, suspected PH, and aortic atherosclerosis (Figure 1).

Chest X-ray of the patient on 28 May 2022 revealed cardiomegaly with suspected pulmonary hypertension and aorta atherosclerosis.
ECG hallmark ST segment depression on lead II, III, avF, V4–V6 followed by T-wave inversion at V1–V3 and R to S ratio in V1 is >1. These findings revealed normal sinus rhythm and right ventricular hypertrophy (Figure 2).
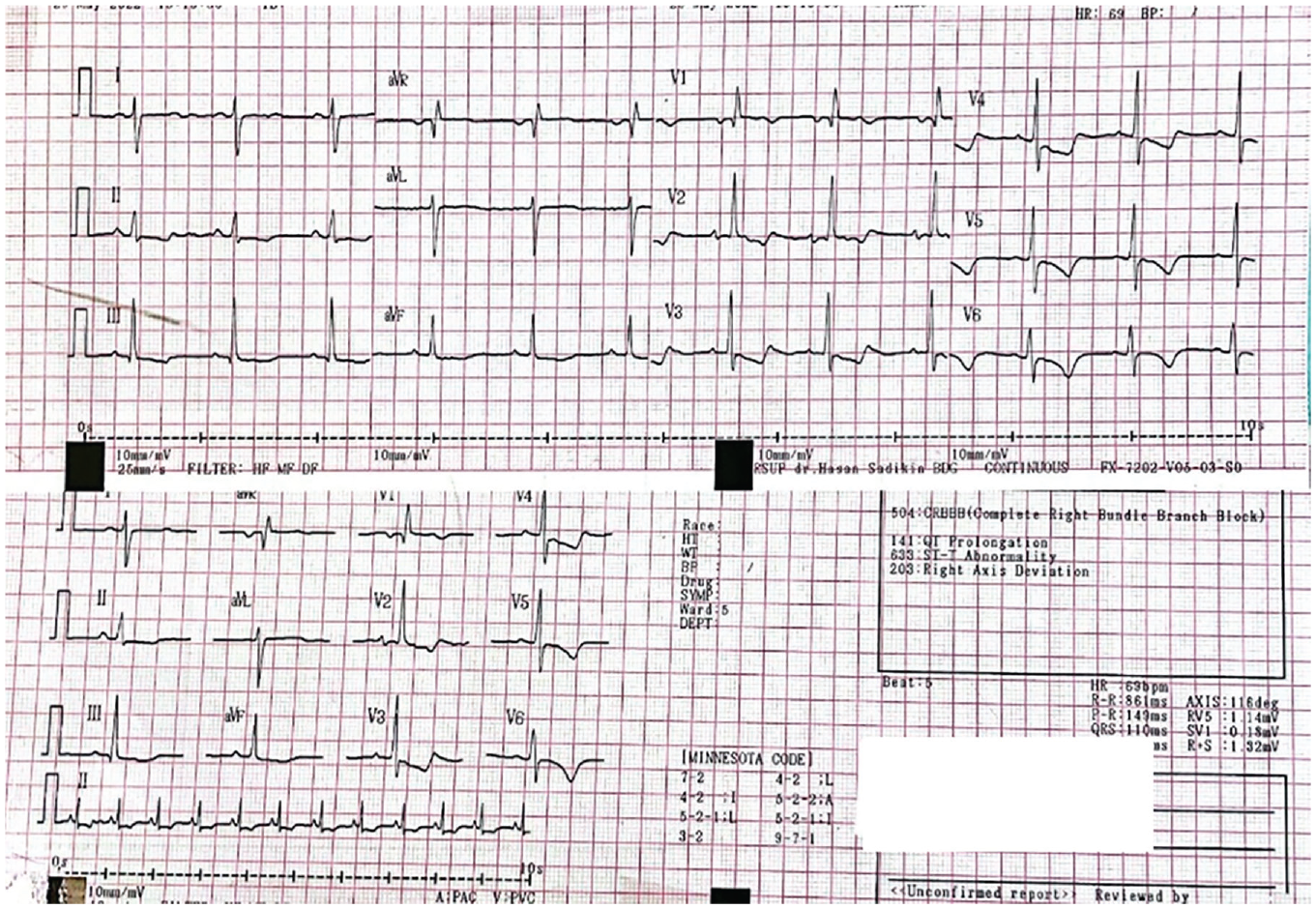
ECG of the patient on 28 May 2022; ECG hallmark ST segment depression on lead II, III, avF, V4–V6 followed by T-wave inversion at V1–V3 and R to S ratio in V1 is >1.
Echocardiography from the referral hospital revealed a left ventricular ejection fraction rate of 74% with a high probability of PH. Pulmonary artery catheterization was not performed in this case. A repeat ultrasound in our emergency unit confirmed IUFD and suspected major congenital anomalies.
She was diagnosed with G3P1A1 23–24 weeks of gestation with suspected PH, history of cesarean section, IUFD, and suspected major congenital anomalies. The patient was induced for labor with 25 mcg of misoprostol per posterior fornix combined with a Foley balloon. In 3 h, stillbirth was delivered, weighing 125 g. Curettage was also performed due to incomplete expulsion of fetal placenta. A bedside echocardiography in the delivery room revealed right atrial dilatation, normal ventricular function (85%), severe tricuspid regurgitation, and a high probability of PH. She was transferred to the cardiac intensive care unit where her oxygen saturation peaked at 60% with maximum oxygen supplementation.
A pulmonary CT scan was postponed due to her unstable condition. She received enoxaparin 1 × 0.6 mg; sildenafil 3 × 40 mg; and iloprost 4 × 5 mcg (nebulizer). Echocardiography was performed when the patient was in a cardiac intensive care unit (31 May 2022), and revealed she had suspected patent ductus arteriosus with 1–1.2 cm in size; left ventricle ejection fraction of 73%; pulmonary artery systolic pressure at 109 mmHg (normal values < 25 mmHg); and indicated PH and severe tricuspid regurgitation with moderate pulmonary regurgitation (Figure 3). She was fitted with a high-flow nasal cannula amidst her persistent hypoxia because her family refused intubation. However, she deteriorated and passed away while in intensive care. An autopsy was not performed in this case because the family did not consent to it.
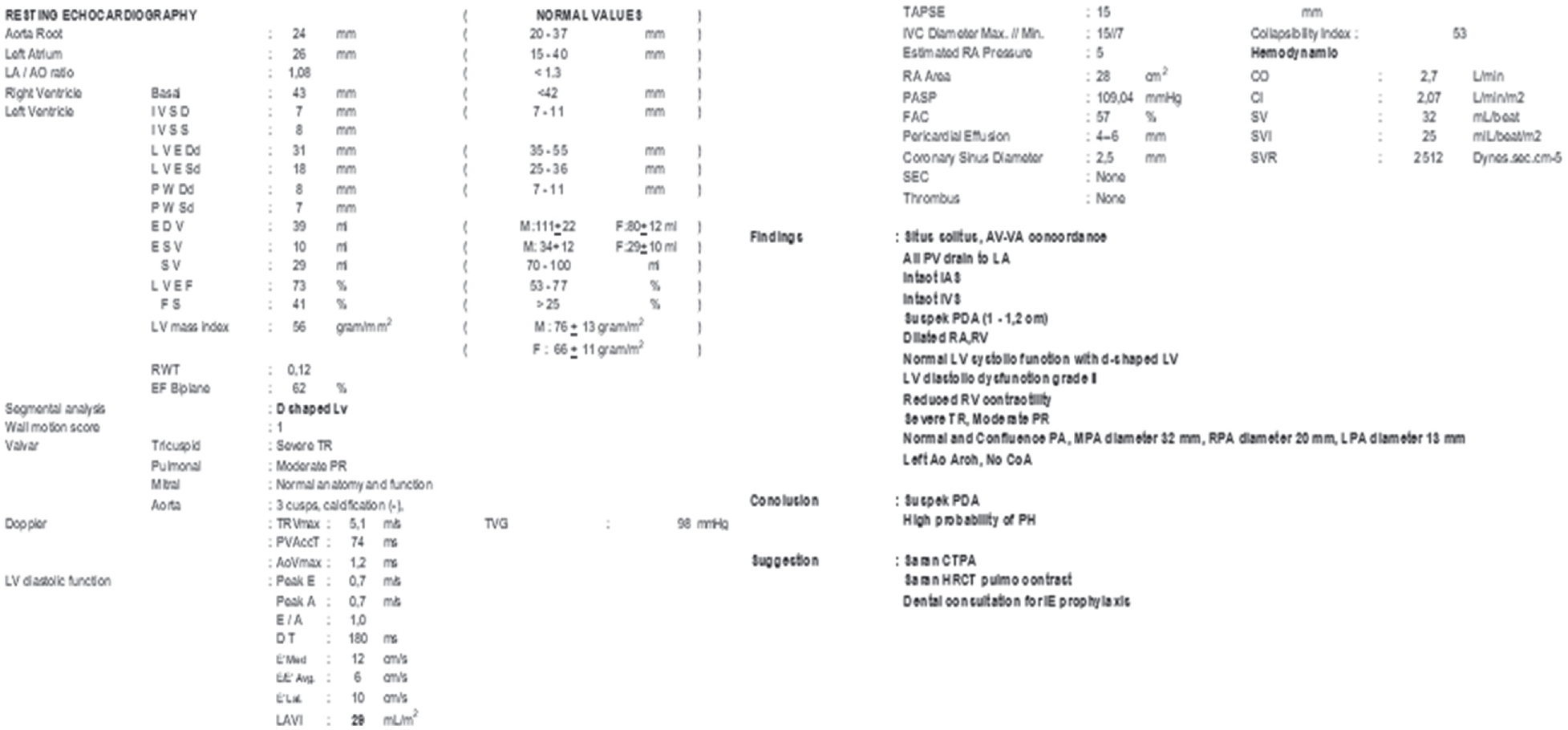
Echocardiography of the patient on 31 May 2022 in CICU.
Discussion
PH is a condition when there is high blood pressure in lung circulation. This condition is defined by an increase in mean pulmonary artery pressure (mPAP) of at least 25 mmHg. PH is divided into five major groups: Group 1, pulmonary arterial hypertension; Group 2, PH owing to left heart disease (PH-LHD); Group 3, PH owing to lung disease and or hypoxia; Group 4, chronic thromboembolic PH (CTEPH); and Group 5, unclear or multifactorial etiologies.3,4 Modified World Health Organization (mWHO) classification of maternal cardiovascular risk classified PH as category 4, which means women with PH are not allowed to pregnant.5,6 This is large because of an inability of the right ventricle to adapt to physiologic changes in pregnancy, labor, and delivery such as increased plasma volume and cardiac output, lower vascular resistance, and increased hypercoagulability state. 7
Pregnancy adds stress to the right chambers and pulmonary vasculature and induces the vasodilatation state due to hormonal changes. This could cause blood turbulence and promote embolism.8,9 Increased pulmonary thrombosis risk further impairs right ventricular function. This results in an increased risk of mortality with an absolute mortality risk of around 20%.4,10 Close observation is required throughout pregnancy and until at least 2 weeks after delivery after successful delivery. 11 Women with PH also develop significantly more preeclampsia/eclampsia syndrome, and eclampsia with preexisting hypertension compared with those women without any heart disease. 12
One of the studies done by Bedard shows a mortality rate of around 25% during the decade ending in 2007 compared with 38% for the decade ending in 1996. 10 Timing for termination depends on the clinical condition of the patient. If the patient is stable, pregnancy may be continued beyond the second trimester. For patients with a new diagnosis of at least WHO FC III and not currently on medication, administration of iloprost followed by sildenafil is recommended. For patients with WHO FC II, close observation and prompt therapy in the second trimester are necessary to minimize the likelihood of future deterioration and adverse effects on the mother and the fetus. 4 A 2010 study, a single-center series of 10 consecutive pregnancies during 2002–2009 reported improved outcomes. A multidisciplinary policy was applied with early administration of targeted prostanoid therapy. Planned cesarean section was instituted at 34 weeks or earlier when deterioration was present. Anticoagulation therapy was prescribed to most patients. All 10 pregnancies resulted in live births with zero maternal death. However, a patient passed away after a month because she one-sidedly halted her treatment and declined hospital admission. 13 Thus, it seems that pregnancy in PH could be allowed with close observation and rapid termination if deterioration occurs.
Pregnancy among those contraindicated due to severe heart lesions is a source of debate on the grounds of human rights. While we would advocate women’s rights to be pregnant, doing so is at the peril of their own lives. International human rights law includes fundamental commitments of states to enable women to survive pregnancy and childbirth as part of their enjoyment of sexual and reproductive health rights and living a life of dignity. Several international human rights organizations such as the International MotherBaby Childbirth Initiative and White Ribbon Alliance stated “every woman has the right to information, informed consent and refusal, and respect for her choices and preferences, including the right to her choice of companionship during maternity care, whenever possible.”14,15 To advocate such rights, we need to have a multidiscipline and integrated system that promotes early detection, affordable, and available cardiovascular disease services in the peripheral area, good surveillance, and early referral if the case is deemed too complicated for the peripheral center.
The main problem in developing countries and low socioeconomic environments such as this case, there are wide disparities in healthcare practices between main centers and peripheral hospitals. Research done by Laili et al. on cardiac disease in pregnancy contributes to 14% of maternal deaths in Soetomo Hospital, Surabaya. 2 Several factors that contribute to this case are non-adequate antenatal visits (OR: 1.7; CI 95%) and delay in heart disease detection (OR: 2.5; CI 95%). 2 Scarcity of cardiologists in Indonesia was mentioned by Qanitha et al. with a cardiologist and population ratio of 1:182.160, with 1485 cardiologists and 270 million people in Indonesia. 1
Despite the patient’s routine control during her current pregnancy at a peripheral center with seven times antenatal care (ANC) with an obstetrician and cardiologist, the lack of standardization in healthcare providers and integration with central health care proves a sufficient number of ANC is still inadequate. Besides termination of pregnancy could be performed before she was referred or the disease progressed. As previously stated by Qanitha et al. authority in decision-making, ignoring the guideline standards, and poor management of after-discharge care are mainly the problems of cardiovascular care in Indonesia. 1
Managing PH in pregnancy requires a multidisciplinary effort by a specialized Pregnancy Heart Team. A Pregnancy Heart Team is led by providers from a cardiologist, maternal–fetal medicine, obstetric anesthesia, pharmacy, and nursing to provide a holistic approach to patient care while facilitating opportunities for cross-disciplinary education. 16 Such a team would only be available at a tertiary hospital and our patient was only referred to us fairly late with IUFD and worsened condition precluding her from earlier detection and better initial management.
This is a case of an adamant patient wishing to conceive despite her severe cardiac disease. From anamnesis, we found the patient had cardiac disease after the delivery of her second child with C-section at 7 months of pregnancy. Following the birth of her second child who passed away after 40 days, she refused to control herself cardiologist. After she had conceived her third pregnancy and had symptoms, she decided to go under the examination of a cardiologist and an obstetrician. It has become a part of the culture in developing countries especially Indonesia, where marriage equates to conception and offspring. Family happiness is said to be dictated by the female’s inability to bear offspring. Research in West Java stated that most respondents viewed pregnancy as a natural phase of life, detached from diseases and/or pathologies. 17 The notion that pregnancy worsens underlying diseases seems alien to most people. As a testament, our patient conceded that she despised her inability to conceive and thus, pursued conception vehemently.
A similar case could happen within a developing country that shares the same cultural impact of pregnancy and emphasizes that patients with similar beliefs are likely to pursue conception even if it is strongly contraindicated; thus, our role is to prevent such outcomes and increase the life quality of mother and child. As proposed by the Standardized Outcomes in Reproductive Cardiovascular Care (STORCC) initiative (Figure 4), pre-conception evaluation is mandatory for all women, and this step is often missed in Indonesia due to scarcity of human resources, low awareness of pregnancy risk, and lack of standardization of health care. This part was also miss-able because heart screening was not covered yet by our National Health Insurance. Even so, early screening and referral are plausible. Delivery mothers with heart problems should be referred to a central hospital for collaborative management by skilled cardiologists, obstetricians, and anesthesiologists. 18 Follow-up after delivery is also mandatory and the mother should routinely checked at least until a year after labor.

Proposed standardized pathway for diagnostic testing during pregnancy for women with cardiovascular disease (adapted from the STORCC initiative). 18
Conclusion
Pregnancy is contraindicated amidst PH. A multidisciplinary approach with rigorous cardiology follow-ups is necessary for PH in pregnancy. Pregnancy termination is immediately mandated to prevent worsening prognosis. High disparities of healthcare providers in developing countries, current socioeconomic views of pregnancy, and un-standardized and late referrals from peripheral hospitals contribute to the higher mortality rate in pregnancy accompanied by cardiovascular disease. Such cases could be prevented with early referral and better treatment in peripheral hospitals, early detection, and referrals. Raising the concern of cardiac disease in pregnancy in society is not an easy task but must be done for better understanding and careful planning of pregnancy.
Footnotes
Acknowledgements
None.
Author contributions
DP and CJC were the attending consultants for the patient involved. AZS, KDT, and DP conceived the design for this case report, collected the data, and interpreted the patient case notes. AZS and KDT wrote the draft. DP, AZS, CJC, and KDT agreed on the following version of the manuscript for publication.
Availability of data and materials
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Consent for publication
Written informed consent was obtained from the legally authorized representative of the deceased subject for the publication of the case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Registration of research studies
Registration of research is not applicable in our case.
Guarantor
The guarantor of this study is Dini Pusianawati.