
Abstract
Eosinophilic annular erythema is a rare eosinophilic dermatosis, characterized by arcuate erythematous urticarial plaques of unclear etiology. Vesiculobullous forms are even rarer, with only few cases described in the English literature. We report a case of vesiculobullous eosinophilic annular erythema with extensive cutaneous involvement poorly responsive to prednisone but showing complete remission with dapsone.
Case
A 57-year-old Caucasian woman presented at the dermatology clinic for an itchy cutaneous eruption. It started on her left thigh and progressively expands in a month.
She was in general good health besides a mitral prolapsus operated in 2018. She was not known for any cutaneous disease nor asthma or nasal polyps. She had been taking aspirin since her cardiac surgery and bupropion, citalopram, and zopiclone for a year. Her last vaccine shot for COVID-19 was 2 months before. She was doing office work for living and did not travel in the past years. She was up to date in her age-appropriate cancer screening which was normal.
She presented with large annular and arcuate erythematous and edematous plaques throughout her body, sparing palms and soles, genitalia, and face. Plaques on the legs were more purpuric with annular configuration (Figures 1–3). Vesicles were visible at the periphery of her plaques on her arms. Her eruption was fixed and accompanied by fatigue, loss of appetite, and peripheral edema. Review of system was otherwise negative. She had no fever and no risk factor for parasitic infection. She had no peripheral adenopathy, and her physical exam was otherwise normal.

Large annular and arcuate erythematous and edematous plaques.

Vesicles were visible at the periphery of the plaques on the arms.

Plaques on the legs were more purpuric with annular configuration.
A 4-mm punch biopsy revealed spongiotic dermatitis with intraepidermal vesicles and abundant eosinophils without flame figures or vasculitis (Figure 4). Perilesional direct immunofluorescence was negative.
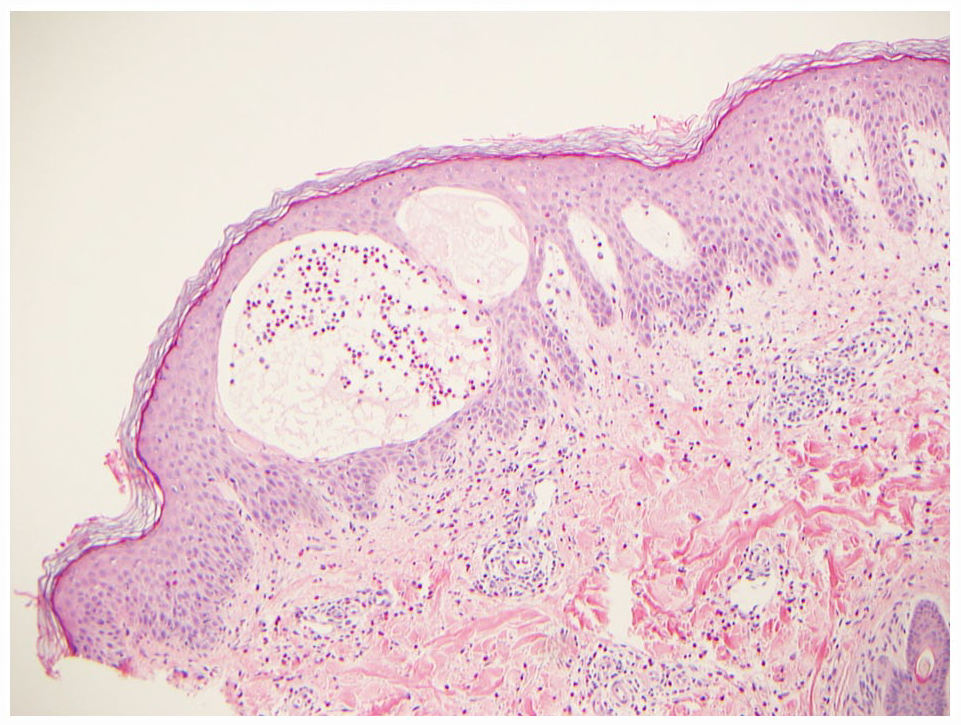
Skin biopsy revealed spongiotic dermatitis with intraepidermal vesicles and abundant eosinophils without flame figures or vasculitis.
Her blood count showed absolute eosinophil counts of 2.7 × 10e9/L without lymphocytosis. She had slightly elevated c-reactive protein (CRP) (12.8), but erythrocyte sedimentation rate (ESR) was normal. Hemoglobin, platelets, renal function, urinalysis, complement level, liver function tests, thyroid function test, and hemoglobin A1c were normal. Indirect immunofluorescence for cutaneous basal membrane antibodies was negative.
She was first treated by prednisone 50 mg a day for 5 days, decreasing of 5 mg every 5 days with betamethasone valerate 0.1% cream as topical therapy. A blood count performed a week after she started prednisone showed an even more elevated absolute eosinophil counts of 5.3 × 10e9/L without lymphocytosis.
Hematology work-up was performed to rule out secondary cause of eosinophilia. Serum immunoglobulins, B12, and tryptase levels were normal. Hepatitis B and C serologies were negative. Serum protein electrophoresis and immunofixation failed to demonstrate a monoclonal spike. Molecular genetic studies were all negative, including FIP1L1-PDGFRA and BCR-ABL fusion genes, JAK2 V617F and KIT D816V mutation, PDGFRB, and T-cell beta and gamma receptor gene rearrangements. Flow cytometry did not reveal a monoclonal lymphocytic population. Interleukin (IL)-5 dosage was of 2.4 pg/mL. An abdominal ultrasound did not show hepatosplenomegaly.
The clinical presentation with a negative thorough etiologic work-up, notably for hypereosinophilic syndrome, was highly suggestive of vesiculobullous eosinophilic annular erythema (EAE).
Dapsone was then started because of persistent peripheral eosinophilia and lack of effectiveness of prednisone on the skin. After a month of dapsone monotherapy at a dose of 100 mg per day, complete clinical and hematological response were achieved. The dose was then slowly reduced to 75 mg per day, still maintaining blood and clinical remission after 5 months.
Discussion
EAE is a rare eosinophilic skin condition of unknown etiology. Its presentation is usually characterized by annular and arcuate urticarial plaques; however, it can also be vesiculobullous1,2 as in our patient.
Annular erythematous plaques have a broad differential diagnosis including figurate erythemas, urticaria, urticarial vasculitis, erythema multiforme, annular psoriasis or lichen planus, polymorphous light eruption, granuloma annulare, cutaneous sarcoidosis, and so on. Clinical characteristics that should be kept in mind for EAE are fixed, often itchy, edematous and erythematous annular plaques with pigmented center and elevated borders in long-lasting lesions. 3 EAE shows initial superficial dermal eosinophil infiltrate which gets deeper in longer-lasting lesions and can show flame figures without vasculitis. 3
In our case, we did a thorough hematologic work-up to rule out hypereosinophilic syndrome because of the persistent hypereosinophilia. Hypereosinophilic syndromes may present with highly polymorphic cutaneous eruption and their diagnosis may be challenging only based on cutaneous presentation. 4
Compared to other vesiculobullous EAE cases, our patient had more extensive skin involvement and higher peripheral eosinophilia. Indeed, she had persistent skin lesions and higher eosinophilia after a week of systemic prednisone at a dose of 1 mg/kg/day.
This may suggest that EAE patients with more extensive skin involvement and peripheral eosinophilia can be refractory to systemic prednisone as a monotherapy and may need other treatments like dapsone which has been described as a therapeutical option with good clinical response. 5 Other treatments described for classical EAE includes hydroxychloroquine, hydroxychloroquine combined with systemic corticosteroids, thalidomide, ultraviolet B (UVB) phototherapy, IL-5 inhibitor, dupilumab, or baricitinib. 5
EAE is a rare eosinophilic dermatosis that should be kept in mind in front of annular, arcuate cutaneous eruption. In even rarer forms, it can be vesiculobullous, like in our patient. In these cases, if the eruption is extensive and associated with peripheral eosinophilia, dapsone can be an option if no response is achieved with systemic prednisone monotherapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Authors obtained verbal informed consent for information and images to be published.