
Abstract
Central neurocytoma is a rare intraventricular tumor, occurring typically in the lateral ventricle of young adults. It is considered as a neuronal-glial benign tumor with favorable prognosis. Imaging is a cornerstone allowing the accurate preoperative diagnosis on the basis of several characteristic features. We report the case of a 31-year-old man who has been complaining of progressive headaches and in whom brain magnetic resonance imaging revealed a central neurocytoma. We remind then, through a literature review, the main criteria to set the diagnosis of this tumor and rule out the other possible diagnoses.
Introduction
Central neurocytoma (CN) is a rare intraventricular tumor arranged as grade 2 by the latest World Health Organization (WHO) classification. 1 First described in 1982 by Hassoun et al., 2 it is a neuronal-glial tumor with an incidence of 0.25%–0.5% of all intracranial tumors. 3 Symptoms generated by this tumor are non-specific and resulting from increased intracranial pressure. Magnetic resonance imaging (MRI) is the accurate imaging modality to raise the diagnosis with some characteristic features such as the “spongy appearance” and “the broad-based attachment.” The prognosis of this tumor is considered to be good when total resection is possible; therefore, the adequate preoperative diagnosis should be made to rule out other imaging similar tumors, especially ependymoma, astrocytoma and choroid plexus papilloma.
Case representation and imaging findings
A 31-year-old man with no medical history complained of headaches for 6 months. They were progressively increasing in their intensity, becoming resistant to drugs and accompanied by visual disorders and vomiting. At physical examination, no neurological deficit was found but a bilateral papilledema was noticed. Brain MRI was performed, it revealed a left intraventricular mass attached to the septum pellucidum isointense on T1WI and T2WI with some foci of mild enhancement at the gadolinium injection (Figure 1). The diagnosis of CN was set by radiologists; the patient underwent gross tumor resection, and histological examination confirmed it. The patient is being followed up to this date with no recent symptoms or worsening. Imaging is scheduled on demand or if a recent complaint occurs.

Brain MRI according to sagittal T1WI (a), axial T2WI (b), axial FLAIR WI (c) and axial T1WI with gadolinium injection (d) showing an intraventricular mass of the left lateral ventricle, isointense in T1 sequence with a broad-based attachment to the septum pellucidum, abutting the wall of the ventricle realizing a scalloping sign (a), isointense to slightly hyperintense in T2WI and FLAIR WI (b, c) with a well-defined strikingly enhanced areas at gadolinium injection (arrow).
Discussion
CN is a slowly growing intraventricular tumor occurring in young adults generally between 20 and 40 years. It is a rare tumor with no sex predilection and no specific symptoms. Clinically, individuals present with signs of intracranial hypertension due the obstruction of CSF (Cerebrospinal fluid) drainage. Other clinical features like behavioral disorders and seizures can be reported.4,5
The tumor develops usually in the lateral ventricles, attached to the foramen of Monro or the septum pellucidum. Despite its benign histology, it can spread through the CSF and infiltrate the cerebellum, the brainstem and the peritoneum in patients with ventriculoperitoneal shunt.
Extraventricular CNs are rare and behave as their intraventricular counterpart. They can occur in any brain location outside the ventricle. Among these sites, they have been described in cerebral hemispheres, deep nuclei, including thalamus, cerebellum, brainstem, spinal cord and retina.6,7
On computed tomography (CT), CN is usually a well-demarked intraventricular mass isoattenuating or slightly hyperattenuating. Calcification is encountered in half cases, and cystic changes are reported. The key of diagnosis is the location, typically attached to the foramen of Monro or the septum pellucidum with a broad-based attachment.8,9 However, other intraventricular tumors occurring in adults represent a differential diagnosis. The table summarizes the main criteria to distinguish each one.
MRI allows the elimination of the other diagnoses through a better analysis to the details of the tumor and its different components. CN is heterogeneous, appears as an isointense mass on T1-weighted images and iso-to hyperintense on T2-weighted images. Calcifications, vessels, cysts or hemorrhage, when present, show hyposignal or asignal on both T1 and T2 sequences except for cysts that are hyperintense on T2WI. However, these cysts, even if usually present and have some characteristic features, may lack at imaging. 10 At gadolinium injection, a degree of enhancement is seen.11–13
In the largest MRI cohort driven by Li et al., 14 six characteristic features were validated to improve the diagnosis of CN, in which three new criteria were reported. The “scalloping sign,” considered as a combination of ventricular wall undulations and spicules of peripheral cysts, was the most specific sign and is better depicted on sagittal views.14,15 The “broad-based attachment” is another imaging feature with the highest sensitivity. It is related to the origin of this intraventricular tumor, which is explained by its derivation from the small gray nuclei of the septum pellucidum or the bipotential progenitor cells on the periventricular matrix.16,17 As astrocytomas and ependymomas show the same aspect in their lateral ventricular location, it is important to analyze the tumor borders that are conspicuous in CN unlike ependymoma and astrocytoma where they are more aggressive and invade the adjacent parenchyma.18,19 Cysts that are usually described in CN take, by themselves, three characteristic patterns. The “bubble-soap sign” consists on a large number of cysts varying in size conferring to the tumor a sponge form. Multiple cysts are also displayed by multiple tumors, 20 most of the times central as a result of hemorrhage and necrosis occurring there. In CN, this rule is broken, and peripheral cysts are of excellent specificity to raise the diagnosis with no pathological basis to date to explain this sign. 14 The other particularity of CN’s cysts is a “fluid–fluid level” appearance which is the consequence of bleeding, an infrequent event in CN, thus, less sensitive.
The “Gemstone” sign is a recent feature considered as highly specific for CN and consists in one or several well-demarked enhanced areas compared to the surrounding non-enhanced or mildly enhanced tumor as clearly evident in our case (Figure 1(d)). Hemangioma-like changes have been advanced to explain its pathophysiological mechanism still unknown. 21
Magnetic resonance spectroscopy (MRS) is helpful to differentiate CN from meningioma and other intraventricular tumors. The spectroscopic profile of CN is characterized by the presence of high levels of choline and glycine, low levels of NAA and absent or low level of Ala compared to intraventricular meningioma. The choline/creatinine and NAA/creatinine ratios seem to be significantly higher in CN compared to other intraventricular tumors, including oligodendroglioma, astrocytoma, subependymoma and glioblastoma multiforme.22,23
At dynamic susceptibility contrast-enhanced MRI perfusion, CN has an intermediate vascularity compared to highly vascularized tumors such as meningiomas, papillomas and renal carcinoma metastases, but higher than that of the ependymomas and subependymomas. Its relative cerebral blood volume (rCBV) is between 2 and 3.24,25 The main differential diagnoses of CN are referred to in Table 1.
Main differential diagnoses of CN.
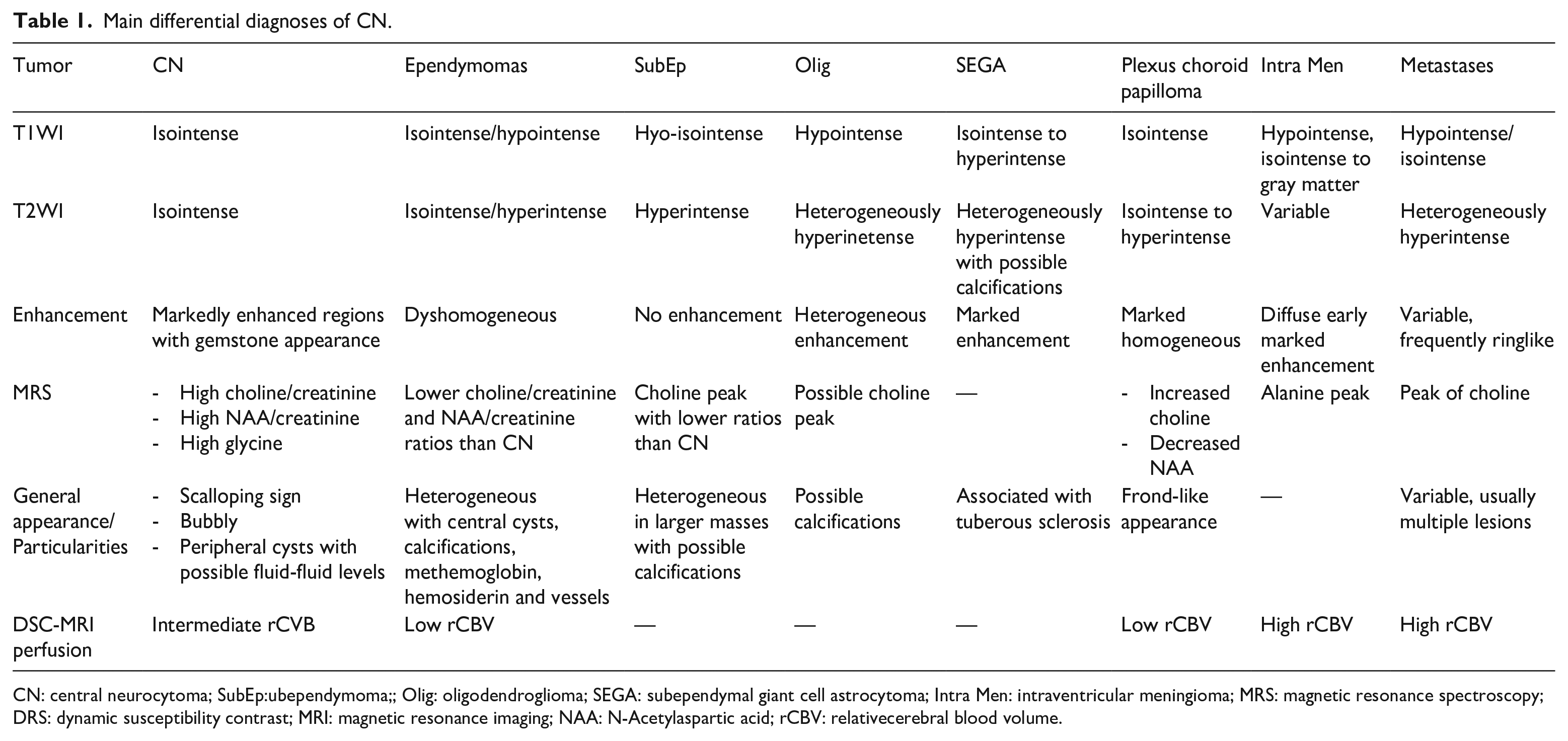
CN: central neurocytoma; SubEp:ubependymoma;; Olig: oligodendroglioma; SEGA: subependymal giant cell astrocytoma; Intra Men: intraventricular meningioma; MRS: magnetic resonance spectroscopy; DRS: dynamic susceptibility contrast; MRI: magnetic resonance imaging; NAA: N-Acetylaspartic acid; rCBV: relativecerebral blood volume.
The treatment of CN is surgical resection with an excellent prognosis demonstrated by reported survival rates at 5-year follow-up between 65.1% and 92.3%. 26 Post-operative radiation is indicated if the resection is incomplete.
Histologically, CN was thought originally to be an oligodendroglioma, but transmission electron microscopy and immunostaining established its neuronal character through a positive immunoreactivity to neuron-specific enolase (NSE) and synaptophysin. 1 However, CN is considered as a neuronal-glial tumor showing also some glial phenotypes, with predominantly neurocytic differentiation.
The pathological diagnosis of CN is based on the proliferation architecture generally evenly distributed on moderately to strongly present cell forms, on nuclear details usually made of monotonous to moderately pleomorphic round nuclei and on background features dominated by stippled chromatin and eosinophilic cytoplasm. However, this pathological diagnosis can be difficult. Next-generation sequencing (NGS) helps identify cumulative copy variants of a tumor. Even so, it is sometimes uncertain to make a diagnosis, especially in atypical tumors with unique changes. Methylation analysis is a promising technique to help confirm diagnosis and rule out confusing ones, but is less available and requires a minimum of 50% of tumor volume with a requested calibrated score greater than 0.7. Distinguishing typical CN from atypical CN is of great interest as atypical forms have been associated with a high rate of recurrence and a poorer prognosis. This distinction is not yet made by the methylation profile. And high levels of MIB-1 (cell proliferation marker), which is a monoclonal antibody against Ki-67, are now thought to be consistent with atypical forms and is considered as the best predictor of proliferative potential and recurrence risk with a cut-off value of 2%–3%.27–29
Although CN is graded as one of “WHO 2” tumors according to the latest classification, it is assumed that those with an aggressive behavior and a higher cutoff of MIB-1 labeling indices (LI) of 10% associated with cellular atypia represent much more a “WHO grade 3.” 29 Thus, reported relapse rates are highly variable from 22% with a labeling index of MIB less than 2% till 63% when higher than it. 30
Conclusion
CN is a rare benign intraventricular tumor with characteristic features at brain MRI. “Scalloping sign,” “broad-based attachment” and “gemstone enhancement” are the most relevant. Neuroradiologist must be aware of to set the adequate diagnosis allowing a curative therapy of excellent prognosis particularly in typical forms.
Footnotes
Author contributions
All authors participated actively to elaboration of this scientific document: the first author, who is the correspondent one, wrote the text; the second and third authors helped at its elaboration; the other authors set the diagnosis and the latest one, in addition, corrected it.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.