
Abstract
Pyostomatitis-pyodermatitis vegetans is an uncommon mucocutaneous dermatosis of unknown etiology. It presents as erythematous pustules that coalesce to form exudative vegetating plaques on the oral mucosa and/or skin. Diagnosis is largely based on clinical assessment, although histopathology should be used as supporting evidence. Pyostomatitis-pyodermatitis vegetans is associated with inflammatory bowel disease, liver dysfunction, and others. We report a case of a 48-year-old man who presented with erythematous eroded plaques involving his nares and upper lip. Investigations revealed a dense mixed inflammatory infiltrate and pronounced peripheral eosinophilia. Uniquely, the patient did not have inflammatory bowel disease or any other systemic condition. Systemic corticosteroids were helpful in clearing mucocutaneous lesions; however, this effect was only sustained at high doses. There are few reports of pyostomatitis-pyodermatitis vegetans in the medical literature. This case highlights key aspects of this extremely rare dermatosis, especially in otherwise healthy patients without inflammatory bowel disease.
Keywords
Introduction
Pyostomatitis-pyodermatitis vegetans (PSV-PDV) is a rare and chronic mucocutaneous dermatosis initially described by Hallopeau in 1898, yet it remains poorly understood today. 1 PSV-PDV is clinically characterized by multiple erythematous pustules that coalesce into well-defined exudative vegetating plaques with characteristic “snail track” erosions on the surface.1,2 The oral mucosa (i.e. gingivae, lips, vestibule, buccal mucosa, tonsils) is most commonly involved, although other mucosal surfaces can be affected; oral lesions are termed pyostomatitis. Cutaneous lesions are usually limited to the groin, axillae, or scalp and are termed pyodermatitis. 2 Pyostomatitis and pyodermatitis lesions do not always coexist, although they are considered to be manifestations of the same condition and have nearly identical histopathological profiles. 2
PSV-PDV predominately presents in males in early adulthood.1,2 Although the term PSV-PDV is suggestive of mucosal and/or skin infection, the exact etiology is unknown and no pathogenic agent has been consistently implicated in the disease. 3 PSV-PDV is likely a consequence of immunologic dysfunction given its strong association with immune dysregulation, most notably inflammatory bowel disease (IBD). There may also be associations with chronic liver dysfunction (primary sclerosing cholangitis, chronic hepatitis, cirrhosis) and HIV. 4 While not all patients have underlying systemic disease, PSV-PDV is almost always reported in the setting of IBD and most patients have gastrointestinal symptoms prior to its onset.3,5 We report a rare case of PSV-PDV in an otherwise healthy male without gastrointestinal or other involvement.
Case report
A 48-year-old male auto mechanic presented with a 3-month history of expanding eroded plaques involving his upper lip and anterior nares bilaterally. This resulted in nasal obstruction, difficulty breathing, and an inability to work. He was previously well with no significant medical history including immunodeficiencies and no constitutional symptoms. There was no history of abdominal pain, diarrhea, bloody stool, or weight loss. He had not recently traveled outside Ontario. There was no family history of IBD.
Clinical examination revealed erythematous and eroded plaques involving his nares and upper lip (Figure 1). The surface demonstrated the snail track sign. There were no other areas of involvement, and there was no cervical lymphadenopathy. Initial investigations showed eosinophilia (1.3 × 109/L), negative HIV and anti-neutrophil cytoplasmic antibodies serology, a normal chest X-ray, and a computed tomography (CT) scan which revealed narrowing of the nasal airways with no involvement of the nasal cavity or bones.

(a) Coalescing eroded plaques with a snail track appearance obstructing anterior nares. (b) Presentation 3 weeks after initiating treatment with systemic corticosteroids.
A skin biopsy showed a dense mixed inflammatory infiltrate including numerous plasma cells and eosinophils (Figure 2). There were destructive changes to the epidermis and hair follicles but no granulomas. The lymphoid cells showed no atypical histologic or immunophenotypic features. Stains for fungal organisms, tissue culture, and direct immunofluorescence were negative. Further investigations including liver transaminases, endoscopy, and fecal calprotectin showed no evidence of liver disease or IBD.
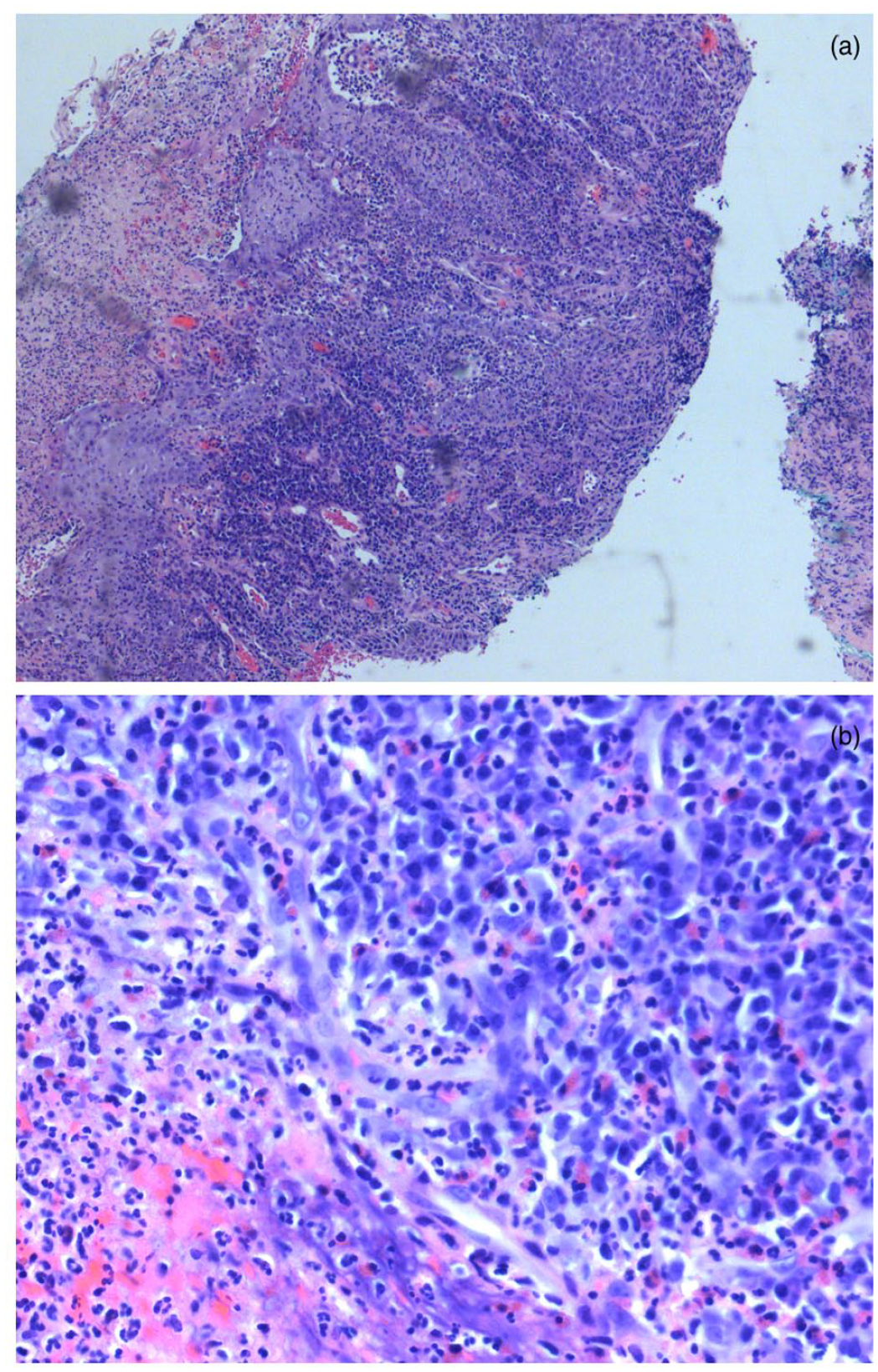
(a) Low-power H + E micrograph depicting a dense infiltrate of plasma cells and eosinophils with destruction of epidermis and appendageal structures. (b) High-power H + E micrograph showing dense eosinophilic infiltrate without cellular atypia.
The patient was started on prednisone (40 mg/day), which resulted in marked improvement after 2 weeks. As the dose was tapered, the nasal lesions regrew. Dapsone (100 mg/day) was begun, and the prednisone was successfully tapered over 3 months.
Discussion
The etiology of PSV-PDV remains poorly understood and there is a wide differential diagnosis.1,2 This should include deep fungal or mycobacterial infections, halogenodermas, pyoderma gangrenosum, pemphigus vegetans, granulomatosis with polyangiitis, and cutaneous B- and T-cell lymphomas.2,4 A skin biopsy including culture is essential to differentiate PSV-PDV from these conditions. The characteristic histopathologic features include epidermal hyperplasia and a dense mixed inflammatory infiltrate with eosinophilic or neutrophilic microabscesses. 2 Immunofluorescence studies can also help to differentiate PSV-PDV from immunobullous dermatoses such as pemphigus vegetans; results are typically negative for PSV-PDV, although positive immunofluorescence findings should not exclude PSV-PDV. 5 Fungal cultures and stains for acid-fast bacilli may identify pathogenic organisms and can also facilitate diagnosis. Peripheral blood eosinophilia is a hallmark feature of PSV-PDV.1,4
Some authors consider PSV-PDV a variant of pyoderma gangrenosum that affects mucosal surfaces. Like pyoderma gangrenosum, it may be associated with IBD; however, as this case demonstrates, some cases have no identifiable associations or skin lesions may long precede the development of IBD.1,2,4 The mean age of onset is in the third decade and there is a male predominance. 2 Recognition of PSV-PDV should prompt further investigations to rule out underlying bowel disease.
Medical or surgical management of associated IBD is often helpful in clearing PSV-PDV lesions, and this should be prioritized in patients with both conditions. 2 Because of the rarity of this dermatosis, there are no evidence-based treatment algorithms. Moderate to high doses of systemic corticosteroids are considered to be effective first-line therapy, but relapse during tapering or withdrawal of medication is likely.2,4,5 PSV-PDV is usually resistant to topical corticosteroids. 2 Steroid-sparing agents such as cyclosporine, tacrolimus, azathioprine, mycophenolate mofetil, methotrexate, and dapsone have been used as second-line therapies, although their efficacy is variable. 1 Tumor necrosis factor (TNF)-alpha blocking biologics have been useful in some refractory cases. 3 As seen in this case, patients may require long-term suppressive therapy and steroid-sparing agents should be preferred.2,4,5 Perhaps agents targeting eosinophils such as anti-interleukin (IL)-4, IL-5, and IL-13 blocking agents may also be useful given the predominant eosinophilic infiltrates and peripheral eosinophilia present in most cases. In this case, long-term follow-up is planned to rule out later-onset IBD.
Footnotes
Acknowledgements
The authors thank Dr Dalal Assaad for her review and assistance with the pathology of the case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient provided consent for publication of the case report and images.