
Abstract
Background:
Pelvic organ prolapse is among the common gynecologic problems worldwide. Although mortality from pelvic organ prolapse is rare, it burdens social, psychological, economic, daily activities, and sexual life.
Objectives:
To assess the quality of life and associated factors among women with pelvic organ prolapse attending hospitals in Western, Ethiopia.
Methods:
A cross-sectional study was conducted at four hospitals in West Ethiopia, from January 1 to June 15, 2023, involving women with pelvic organ prolapse. A single population proportion formula (95% confidence, 23.52% prevalence, 0.05 margin of error) yielded a sample size of 276. A validated quality of life tool by Digesu (2005) on the Prolapse quality of life questionnaire was administered by trained staff to assess quality of life. Data were analyzed using SPSS (version 26), employing descriptive statistics and bivariate analyses, with candidate variables for multivariable analysis selected at a p value of 0.25. Multivariable linear regression was performed after assessing model fit, considering a p < 0.05 as statistically significant.
Results:
A total of 232 (84.1% response rate) women attending or followed by four participating hospitals were involved in the study. The mean age of all women was 50.7 ± 9.2 years. Most of the participants (81.9%) were married; however, three women (1.3%) who were not married also developed a prolapse. Nearly a third (30.2%) had attended primary school; however, only 70 (30.2%) had no formal education. More than three-fourths (78.9%) had no mental or medical illnesses. The prolapse quality of life score was 45.3 ± 4.1. The higher quality of life was contributed to by sleep/energy and severity measures. Attending tertiary education and living with comorbidities were associated with quality of life.
Conclusion:
The quality of life of women living with pelvic organ prolapse was similar. It is affected by education levels and the presence of comorbidities. Further studies are warranted to establish the factors associated with quality of life by recruiting subjects through probability sampling methods.
Background
Pelvic organ prolapse (POP) is the descent of pelvic organs from their normal anatomic sites. No source specified.1,2 The bones of the pelvis are the rigid foundation to which all of the pelvic structures are ultimately supported. 2 POP is either the descent of the anterior vaginal wall (cystocele), uterus/cervix (uterovaginal prolapse (UVP)), or the posterior vaginal wall (rectocele), the vaginal apex after hysterectomy, rectum, or perineum, alone or in combination. 2 Patients may have uterine prolapse or, after hysterectomy, the vaginal cuff may prolapse, resulting in apical vaginal prolapse. 3 The rectum, small bowel, and sigmoid colon also may prolapse in posterior vaginal wall prolapse, resulting in rectoceles, enteroceles, and sigmoidoceles, respectively. There is no consistent definition of POP, and its prevalence is not exactly known. 3 In contrast, studies that define prolapse solely based on patient symptoms showed a prevalence ranging from 3% to 6% in the United States. 2 Although mortality from POP is negligible, significant deterioration of lifestyle is associated with prolapse. It has socioeconomic and health consequences affecting overall health, sexual function, daily activities, and family relationships. 3 Currently, available treatment options are pelvic floor muscle exercise, vaginal pessaries, and surgeries. In Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, POP was the major (41.1%) indication for hysterectomy. A study conducted in Gondar Hospital, Ethiopia, showed that UVP accounted for 19.9% of gynecologic operations. POP accounted for 40.7% of the major gynecologic operations done in Jimma University Specialized Hospital, Ethiopia. 3
The risk for POPs is multifactorial. Among these, vaginal childbirth is most associated with POP. In some studies, pregnancy itself is predisposed to POP. In the Pelvic Organ Support Study, the risk of POP rose 1.2 times with each vaginal delivery, with high rates among multiparous women.1,2 These include big baby, episiotomy, prolonged second-stage labor, anal sphincter laceration, instrumental delivery, epidural analgesia, and induction or augmentation of labor. 2 In addition to obstetric factors, menopause, aging, hypoestrogenism, chronically increased intraabdominal pressure, chronic obstructive pulmonary disease, constipation, obesity, pelvic floor trauma, genetic factors, race, connective tissue disorders, spina bifida. 1 Although mortality from POP is negligible, significant deterioration of lifestyle is associated with prolapse.
Currently, available treatment options are pelvic floor muscle exercise, vaginal pessaries, and surgeries.7,8
POP has several effects on their emotional state, in sexual intercourse and urinary incontinence, and it causes a significant financial burden: in economic terms. It is an important contributor to anxiety and depression, especially by urinary and defecatory symptoms.3,5
Bulge is the commonest symptom; other symptoms including pelvic pressure, vaginal or perineal protrusions are among common symptoms. These symptoms worsen with prolapse progression. Women with prolapse beyond the hymen are more likely to report a vaginal bulge and have more symptoms than those with prolapse above the hymen. If bulge symptoms are the primary complaint, successful replacement of the prolapse with nonsurgical or surgical therapy will usually provide adequate symptom relief. 3
Urinary symptoms are common symptoms in patients with POP and may include urine frequency, stress urinary incontinence, urgency urinary incontinence, urinary retention, voiding dysfunction, and recurrent urinary tract infection. Correction of prolapse does not guarantee a cure of these symptoms, even though these symptoms are caused or worsened by POP.1,2 Constipation is one of the common symptoms in women with POP, but POP generally is not the cause of constipation. 9 But a posterior vaginal wall defect that bulges as it fills with hard stool can cause constipation. This affects the normal mechanics of defecation to create obstruction-type constipation. 10 In one study of defect-directed posterior repair, constipation resolved postoperatively in only 43% of patients. 1 Thus, constipation symptoms should be thoroughly assessed before proceeding with surgery. Surgical repair or treatment with a pessary usually will not cure constipation, and it should be evaluated separately. 5
Female sexual dysfunction is also seen in patients with POP, multifactorial and includes urogenital atrophy, aging, and male sexual dysfunction. However, study findings are inconsistent. POP is not a fatal medical problem, but it might have a considerable impact on female quality of life (QOL). 13 Only 17% of women with POP in Ethiopia receive care on the grounds of fear of disclosure, social stigma, and lack of money. Despite the severity of the problem, the government has no separate strategy to manage the problem in the health system. This women’s health disorder often disrupts marital and sexual relationships in addition to causing great physical discomfort. Because of the condition, women suffering from POP frequently receive physical and verbal abuse from their husbands and mothers-in-law, which leads to divorce.2,4
We can treat most of the above symptoms surgically. The four hospitals provide a lot of services to the population. But there is no published information on patients or POP on their QOL. The primary objective of our study is to determine the QOL and its associated factors among women with POP at hospitals in West Ethiopia.
The four hospitals serve millions of people with different medical problems. Knowledge of patients with POP visiting outpatient departments on local demographic data, risk factors of POP, their QOL, and their need for treatments will help in outlining the plans for early detection, diagnosis, and management of POP. The information in the present study may be considered as baseline data for POP in the four hospitals. To further the knowledge of the investigators, there is no previous study done on the QOL in patients with POP and factors associated with POP in the study area. Hence, the results of this study may serve as the cornerstone finding that creates insight among healthcare planners and administrators.
Further, Zonal and town healthcare sectors and stakeholders, including the health bureau and other concerned bodies, may consider the findings while planning healthcare interventions. This study will provide baseline information regarding QOL in patients with POP and factors associated with POP. It helps other researchers for studies to be conducted in the future.
Methods and Materials
Study area
This study took place in four hospitals in Western Ethiopia: Wollega University Referral Hospital and Nekemte Specialized Hospital (both in Nekemte city) and Ayira General Hospital, and Gimbi General Hospital (West Wollega Zone). Nekemte, 331 km west of Addis Ababa, had a population of 75,219 in 2007. The hospitals offer various services, including surgical, medical, obstetric, gynecologic, pediatric, and neonatal care. Nekemte Specialized Hospital serves a catchment population of 3.5 million (referral center for 10 million). Wollega University Hospital serves five million. Ayira General Hospital (NGO-owned) conducts POP screening campaigns, while Gimbi General Hospital is government-owned.
Study period
The data was collected at the four mentioned hospitals between January 1 and June 15, 2023.
Study design
A facility-based cross-sectional study was conducted to assess the QOL and associated factors among women with POP at the selected health facilities.
Sample size estimation
A single population proportion formula was used, with assumptions of a 95% confidence level, 23.52% national POP prevalence from a meta-analysis, 11 a margin of error of 0.05, and an 84.1% response rate. The formula is n = (Zα/22 × p × q)/d2.
Accordingly, n = ((1.96)2 × 0.2352 × 0.7648)/0.0025, n = 276. So, the minimum sample size required for this study was 276.
Sampling technique
A purposive sampling technique was applied to select all women with POP, and those who fulfilled the inclusion criteria during data collection were included in the study.
Inclusion and exclusion criteria
Inclusion criteria
Women who were diagnosed with any stage of POP (the diagnosis was retrieved from their medical records), who were aged 18 and above.
Women who did not undergo surgery or were managed with a pessary.
Women who volunteered to participate in the study.
Exclusion criteria
Women who were medically/gynecologically unstable were excluded from the study.
Data collection tool
The questionnaire was used to collect information from the participants. The questionnaire contains four tools in this study comprising four sections. Section 1: “Socio-demographic characteristics,” section 2: “Maternal obstetric and gynecologic characteristics,” and section 3: “Prolapse quality of life (P-QOL) version 4.” While sections “Socio-demographic characteristics” and “Maternal obstetric and gynecologic characteristics” were developed by the author from literature,3,4,6,10,12 section 3 was adopted from the original developers, which was validated by Digesu (2005). The scale achieved face and content validity (Supplemental Material). Similarly, Cronbach’s alpha of each item was >0.8, and test-retest reliability also achieved a high correlation between items. The P-QOL scale aimed to measure the impact of prolapse on the woman’s QOL. Responses ranged from “none/not at all,” to “slightly/a little” and “moderately” to “a lot.” Thus, a scoring system for each item was used for severity measurement of urogenital prolapse symptoms. Scores in each domain range from 0 to 100, with a high score indicating a greater impairment of QOL, while a low score indicates a good QOL.
The adopted scale, P-QOL, was forward-translated by two Afaan Oromo experts, and backward translations were done by experts in both Afaan Oromo and English. The discrepancies in the translations were solved through discussions. Finally, a common Afaan Oromo version (Annex 2) was used for data collection.
Clinicians collected data (one midwife, two gynecology and obstetrics residents, and one health officer). The principal investigator gave a brief orientation on the questionnaire to create a common understanding of the questions. An interviewer administered a face-to-face interview. The data were collected while the woman visited the gynecology clinic of the hospital. However, data were collected after a POP screening campaign was conducted by staff from Ayira Hospital in the community. Four data collection supervisors (one at each hospital) were involved in the supervision of data collection processes.
Quality control
Data quality was ensured through four techniques: (1) training data collectors, (2) continuous supervision from the principal investigator, (3) using an adopted and psychometrically tested tool, and (4) continuous reviewing and checking for completeness of the data. Pretesting was not done as the case is rare.
Variables
Independent variables
The independent variables include individual variables under the socioeconomic and demographic characteristics, namely age, education level, employment status, marital status, place of residence, income of the family in birr per month, and maternal medical, obstetrics and gynecologic characteristics, including medical illnesses, parity at event, mental illnesses, number of living children, and mode of delivery, and status of menopause on symptom onset.
Dependent variable
The dependent variable was QOL.
Operational definitions
POP: A woman with prolapsed pelvic organs.
Sexually active: A woman having sex currently.
Bulge symptoms: Sensation of vaginal bulging or protrusion, seeing or feeling a vaginal or perineal bulge, pelvic or vaginal pressure, heaviness in the pelvis or vagina.
Urinary symptoms: Urinary incontinence, urinary frequency, urinary urgency, weak or prolonged urinary stream, hesitancy, feeling of incomplete emptying, manual reduction of prolapse to start or complete voiding, position change to start or complete voiding.
Bowel symptoms: Incontinence of flatus or liquid/solid stool, feeling of incomplete emptying, hard straining to defecate, urgency to defecate, digital evacuation to complete defecation, splinting vagina or perineum to start or complete defecation, feeling of blockage or obstruction during defecation.
Sexual symptoms: Dyspareunia, decreased lubrication, decreased sensation, decreased arousal or orgasm.
Pain: Pain in vagina, bladder, rectum, pelvic pain, and low back pain.
Data processing and analysis
The statistical analyses were performed using SPSS (version 26). Descriptive statistics were calculated for sociodemographic characteristics, maternal medical, obstetric, and gynecologic characteristics, and P-QOL. The frequency and percentage were calculated for categorical variables, whereas the mean and standard deviation were calculated for continuous data. Model assumptions, including normality, linearity, multicollinearity, and equal variance, were checked. Bivariate analyses of overall P-QOL with other variables were conducted using (a) the Pearson product–moment correlation for continuous variables, (b) the independent samples t-test for binary variables, and (c) ANOVA for categorical variables with three or more options. Variables with p < 0.25 were considered candidates for multivariable linear regression. Multivariable analyses were conducted with a linear regression model using variables that are significant in bivariate analyses. p < 0.05 in bivariate and multivariable analyses was considered statistically significant.
Ethical considerations
The ethical review committee of Wollega University Institute of Health Sciences granted ethical clearance for the study under reference number WU/REC/797, with minutes recorded as 1026/2023. An approval letter was secured from the Department of Obstetrics and Gynecology and was submitted to each participating hospital to request their permission and cooperation. All data obtained from the records will remain anonymous. Integrity will be upheld throughout the processes of data collection, analysis, and interpretation. Written consent was obtained from participants with formal education, while oral consent with a fingerprint signature was collected from participants lacking formal education.
Results
Sociodemographic characteristics of the participants
A total of 232 (84.1% response rate) women attending or followed by four participating hospitals were involved in the study. The mean age of all women was 50.7 ± 9.2 years. Their ages range from 32 to 82 years. Most of the participants (81.9%) were married. Half of the women who participated in the study (50.4%) were farmers, followed by housewives (35.8%). Nearly a third (30.2%) attended primary school; however, only 70 (30.2%) had no formal education. The mean monthly income of the participants was 1839.7 ± 1052.3 ETB. The mean body mass index (BMI) of the participants was 20.3 ± 14.7. The result shows that the BMI of women was in a normal weight range (Table 1).
Sociodemographic characteristics of the participants, 2023.
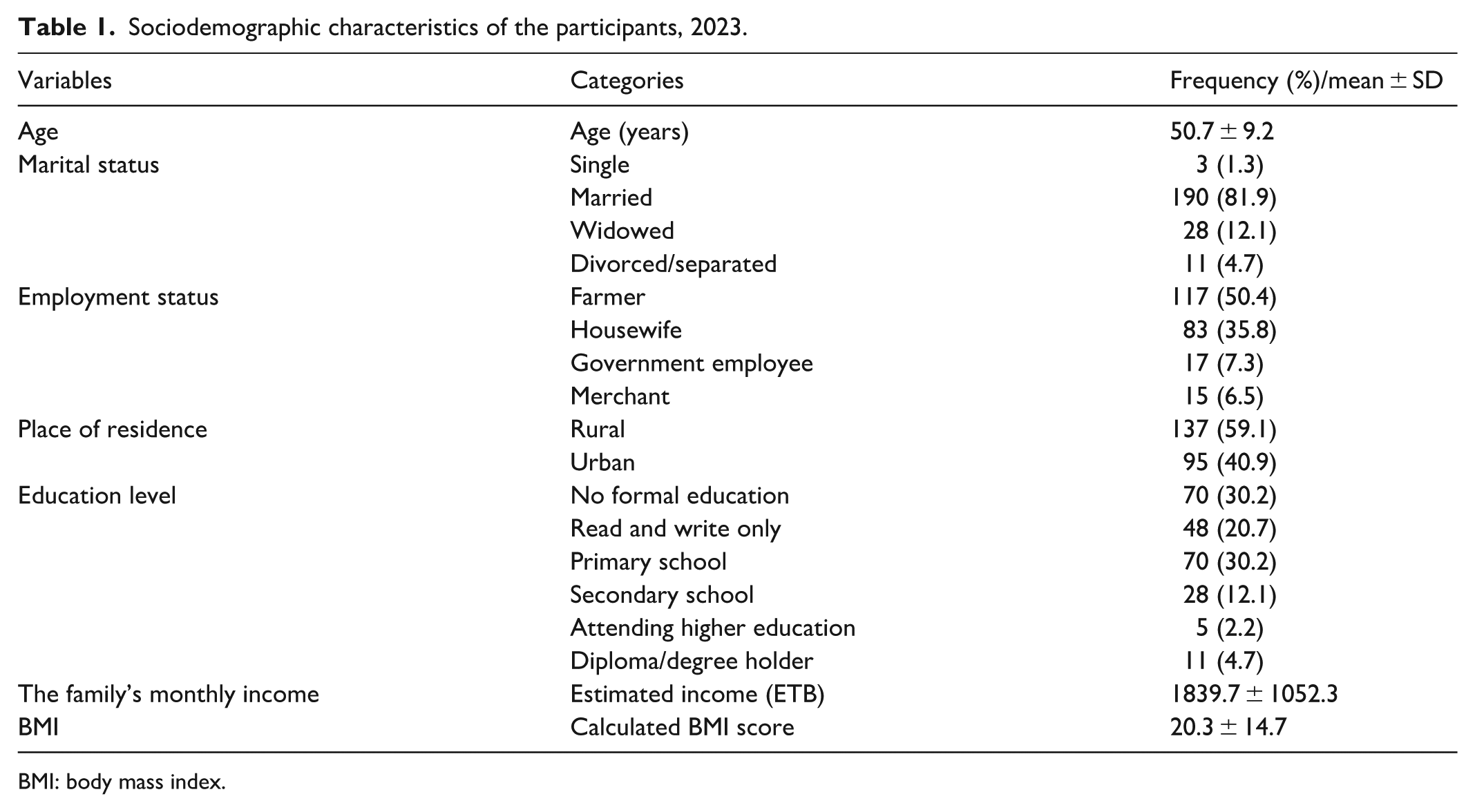
BMI: body mass index.
Maternal obstetrics and gynecologic characteristics
The mean parity of the women was 4.3, with a range of 1–9 births. The mean duration of POPs ranged from 5 to 48 months, with a mean of 18.6 ± 7.7. More than three-fourths (77.2%) of women gave birth via spontaneous vaginal delivery, whereas only one in 10 women were assisted with the instrument. Among identified risk factors, age contributed to half (50.6%), followed by chronic coughing (20.8%). A quarter (26.7%) were not sexually active due to urinary incontinence or bulge in the vagina (54.8%), followed by pain during sexual intercourse (27.4%; Table 2).
Maternal obstetrics and gynecologic characteristics of the participants, 2023.

POP: pelvic organ prolapse.
QOL among women with POP
A prolapse quality of life questionnaire (P-QOL) was used to measure the QOL among women with POP. The score was rated out of 100, with the higher score indicating a better QOL and vice versa. P-POP questionnaire is composed of eight domains (see the “Materials and methods” section).
The general health perceptions of the women were 35.5 ± 11.8, the prolapse impact was 46.0 ± 4.8, role limitations were 35.2 ± 8.1, physical/social limitations were 50.8 ± 11.0, and personal relationships were 47.2 ± 11.5. The emotions of the women about prolapse were 46.6 ± 14.3, its impact on the sleep/energy of the women was 57.2 (18.0), and the severity measures were 51.7 ± 12.1. As the score indicated on each domain reveals, the prolapse limited the women’s roles and lowered their general health perceptions. Conversely, higher QOL was attributed to the low impact of prolapse on sleep and energy. Overall P-QOL was 45.3 ± 4.1, indicating the P-QOL was scored to less than half of the 100 score (Table 3).
Quality of life among women with pelvic organ prolapse, 2023.

P-QOL: prolapse quality of life.
Associated factors of prolapse, QOL
Among eighteen variables tested for bivariate analyses, only six variables, namely marital status (F = 11.742, p = 0.194), employment status (F = 11.743, p = 0.183), education level (F = 2.037, p = 0.109), being on menopause (t = −2.593, p = 0.015), reasons for sexually not active (F = 9.449, p = 0.031), and presence of medical or mental illnesses (t = −2.226, p = 0.034) were associated with QOL at p < 0.25 (Table 4). These variables were used in the multivariable analyses.
Bivariate and multivariable analyses of variables with overall prolapse quality of life.

The bold font in the p value indicates statistically significant findings.
β: linear regression coefficient; BMI: body mass index; POP: pelvic organ prolapse.
Pearson correlation.
Reference category.
ANOVA F-statistics.
Independent samples t-test statistics.
Two variables, education level and status of medical/mental illnesses, remained statistically significant in the multivariable analysis of QOL, and statistically significant 76% variability was found among factors (R 2 = 0.760, p = 0.006). Compared with women with no formal education, those attending tertiary education (β = 1.900, 95% CI = 0.589; 3.211, p = 0.001) were significantly associated with higher P-QOL. Those who were combined with mental or medical illnesses (β = −3.288, 95% CI = −6.368; −0.207, p = 0.038) were associated with low QOL, compared with those without any mental or medical illnesses (Table 4).
Discussion
This study examined the QOL and its predictors among women with POP in West Ethiopia. The P-QOL of participants was 45.3 ± 4.1, which is slightly lower than the P-QOL (48.35) of women who attended Felega Hiwot Comprehensive Specialized Hospital, Northwest Ethiopia. 2 This slight variation might be attributed to age variation, as older adults participated in this study. This implies that providing healthcare support might be warranted for older women with POP. A better QOL was obtained than in the study conducted in Bangladesh, 3 which might be due to the co-existence of urinary incontinence among the women who participated in a study conducted in Bangladesh. This indicates that providing care for affected physical, psychological, and sexual health might be needed to improve QOL. However, the result of my study is lower than the QOL score of studies conducted in Turkey (78.58).3,4 The better QOL in studies conducted in Turkey might be attributed to better living standards. It is comparable to the result of a systematic review and meta-analysis of seven studies (44.59). 5 Overall QOL of women is moderate (48.35) when compared with other empirical studies. However, there are limited studies conducted in Ethiopia and Africa to make an integral discussion.
Education level and status of medical/mental illnesses were identified as associated factors of QOL. Women who are attending tertiary education are associated with high QOL. This may be due to the chance of getting information about reproductive issues, perhaps POP. Another possible reason could be exposure to information via online and social media. Those who did not attend formal education, however, may not seek information about reproductive issues. Another reason could be that most of the women came from the rural areas where accessibility to health care is difficult, and this may be due to the social and political crises in the region. Thus, providing information about POP could be the best option to increase their awareness so that they can boost their quality-of-life domains.
The second factor associated with P-QOL was the presence of comorbid diseases. Comorbid with mental or medical conditions negatively influences P-QOL. Comorbidities predict the outcomes and prolapse management-seeking behavior. A case-control study identified that women seeking advanced POP treatment could lower their body image and QOL. 6 Another possible justification could be that medical comorbidities may reduce their immunity, and cause multiple burdens and emotions. Hence, treating comorbidities is essential to improving QOL.
Strengths and limitations of the study
Strengths of the study
The recruitment of subjects from multiple centers, that is, pertinent hospitals in the west region were used to recruit the subjects.
The study used all women who attended the hospitals or were screened by the hospitals.
The P-QOL was measured using a validated P-POP questionnaire, which is specific to measure QOL.
Limitations of the study
No sampling techniques were applied due to difficulties in achieving the required samples in the study period.
We used purposive sampling techniques to achieve the required sample size; hence, generalizing to the whole population is difficult.
No pretest was conducted since it is a rare case.
Conclusion
The QOL of women with POP is almost similar. Sleep/energy and severity measures contributed to better QOL. Attending tertiary education and living with other comorbidities were associated with QOL among women living in West Ethiopia. Further study should employ random sampling methods to recruit participants.
Based on the findings of the study, the following recommendations have been proposed: we recommend that another researcher conduct probability sampling techniques. We also recommend that another researcher conduct a study on the study topic.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251372748 – Supplemental material for Quality of life among women with pelvic organ prolapse in West Ethiopia: A hospital-based study
Supplemental material, sj-docx-1-smo-10.1177_20503121251372748 for Quality of life among women with pelvic organ prolapse in West Ethiopia: A hospital-based study by Leta Hinkosa Dinsa, Asfaw Tadesse Mengesha, Dereje Chala Diriba and Demisew Amenu Sori in SAGE Open Medicine
Footnotes
Acknowledgements
I would like to extend my heartfelt thanks to study participants, data collectors, participating hospitals’ medical directors, and obstetricians and gynecologists for participating, permitting, and facilitating data collection. I also thank the Oromia Health Bureau for funding this study.
Ethical considerations
An ethical clearance letter with a WU/REC/797 ethical clearance number was obtained from Wollega University, Institute of Health Science, Institutional Research Ethics Review Committee. A formal letter was given to the respective departments. All ethical principles were maintained according to the Declaration of Helsinki.
Consent to participate
Written consent was obtained from participants with formal education, while oral consent with a fingerprint signature was collected from participants lacking formal education.
Author contributions
Conceptualizations: L.H.D. and A.T.M. Formal analysis: L.H.D., A.T.M., and D.C.D. Funding acquisitions: D.A.S. Investigations: L.H.D., A.T.M., D.C.D., and D.A.S. Investigations: Methodology: L.H.D., A.T.M., and D.C.D. Software: L.H.D. Supervision: A.T.M. and D.A.S. Validation: L.H.D., A.T.M., and D.C.D. Original draft: L.H.D., A.T.M., D.C.D., and D.A.S. Writing: review and editing: L.H.D. and D.C.D. L.H.D.: the corresponding author is declared as a guarantor, who accepts full responsibility for the finished work and/or the conduct of the study, has access to the data, and controls the decision to publish.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.