
Abstract
Tuberculosis endometritis is a pathological diagnosis and has been always over shadowed by pelvic tuberculosis. It is usually asymptomatic, but patients could complain of menstrual irregularity and per vaginal discharge. We report a case of a 37-year-old female who presented with per vaginal discharge for 2 years. Histopathology showed numerous caseating and non-caseating granulomas with plasma cells, Ziehl–Neelsen stain for acid fast bacillus is positive, and she was initiated on anti-tuberculosis treatment. On subsequent follow-up visits, patient was doing well with complete resolution of symptoms. Genital tuberculosis is usually caused by reactivation of organism from systemic distribution during primary infection. It is estimated that approximately 8 million cases of tuberculosis occur worldwide every year, 95% of which are from developing countries. Tuberculosis usually affects the lung but about one-third of patients have extra pulmonary involvement which include female genitals organs and other organs. Genital tuberculosis is an indolent infection: its common symptoms include pelvic pain, vaginal bleeding, amenorrhea, vaginal discharge, and infertility. Most of the patients respond quickly after initiating anti-tuberculosis medications. We recommend that all patients with a positive Ziehl–Neelsen stain and menstrual abnormalities undergo aggressive evaluation for genital tuberculosis.
Introduction
Tuberculosis (TB) is a life-threatening chronic granulomatous inflammatory disease caused by mycobacterium TB, an aerobic bacterium and predominantly presenting with pulmonary disease.1,2 It remains a worldwide problem despite discovery of the causative organism for more than a century ago. 1 TB of the genitourinary tract is rare but can become a secondary complication in women diagnosed with TB of the lungs. 3
TB endometritis was first described in 1847 by Morgani: it continues to exist as a pathological diagnosis; however, it has always been shadowed by pelvic TB. 1 Patients usually asymptomatic but could present with menstrual irregularity and infertility.1,3
We report a case of a woman with a history of menstrual irregularity who was diagnosed to have TB endometritis and was initiated on anti-TB treatment. This case report from Aga Khan Hospital, Dar-es-Salaam, Tanzania, will highlight our approach to diagnosis and treatment of TB endometritis.
Case presentation
A 37-year-old lady (para 2 living 2) reported to have last normal menses period 2 years ago. Presented with per vaginal discharge for 2 years which was copious, yellowish, and non-itchy, which made her use one pad each day. She reports to have an intra-uterine device inserted 2 years ago which was later removed. She denies any history of lower abdominal pain, postcoital bleeding or cough, fever, loss of weight and night sweats. During her illness, she has been treated with variety of antibiotics and antifungal medications without improvement. She was otherwise well and with no significant medical history. She has no known drug or food allergy. There is no any family history of gynecological or other malignancies that was reported. She has delivered two times through cesarean section, and there is no history of other gynecological procedures reported. She is non-smoker and does not consume any alcohol. During childhood, she received Bacillus Calmette–Guerin (BCG) vaccination.
On examination, she was alert, not pale, no lower limb edema, and had stable vital signs. The abdominal examination revealed normal contour, a pfannenstiel scar, soft and non-tender. There was no mass palpable, and uterus was not bulky. The rest of the systemic examination was normal.
Speculum examination was unremarkable except with blood oozing from the cervix. Bimanual examination was unremarkable, endocervical swab was done which was negative on gram stain and no organism growth on culture media.
Pap smear was not performed due to vaginal bleeding; however, a pap smear done 1 year ago revealed inflammatory cells.
Transvaginal ultrasound was performed which showed an anteverted uterus with a grossly abnormal endometrial echo pattern. The endometrium was heterogenous and had an irregular surface (Figure 1).

Transvaginal pelvic ultrasound showed an abnormal endometrial echo pattern.
After the history and physical examination, we had a differential diagnosis of endometritis; the patient was then scheduled for diagnostic hysteroscopy. Preoperative investigations included a hemoglobin level of 11.4 g/dL, white blood cell 5.61/L, platelets 181/L, and CA-125 (Serum) 41.78 U/mL (0–35). The patient’s hepatitis and HIV status were negative. A chest X-ray showed no evidence of pulmonary TB.
Intra-operative findings revealed a stenosed cervical canal and uterine synechiae was present. Release of uterine synechiae and endometrial biopsy via curetting was done. Blood loss was not excessive and the patient was discharged home the same day. Histopathology of the curettings showed numerous caseating and non-caseating granulomas with plasma cells, Ziehl–Neelsen stain for acid fast bacilli was positive (Figure 2).
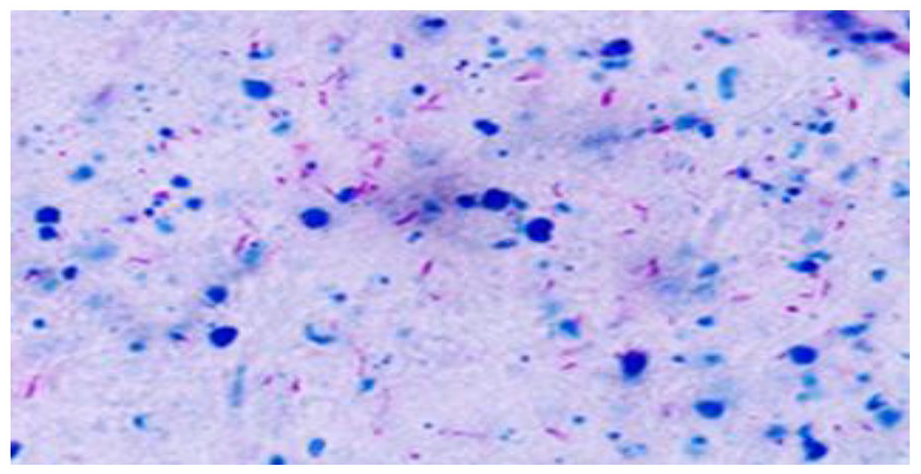
Ziehl–Neelsen smear showing AFB positive in our patient.
Based on the history and results of endometrial biopsy, our provisional diagnosis was endometrial TB. The department of internal medicine was consulted and initiated the patient on one combined tab daily, consisting isoniazid, rifampicin, ethambutol, and pyrazinamide for 2 months (Intensive phase), then tab (isoniazid, rifampicin) for 4 months (Continuation phase).
Upon follow-up, she reports bleeding to have ended in the fourth week of her treatment. She has been doing well and disease-free after completion of the treatment.
Discussion
Genital TB is usually caused by reactivation of organism from systemic distribution during primary infection. 4 It is estimated that approximately 8 million cases of TB occur worldwide every year, 95% of which are from developing countries. 4 In Tanzania, the current incidence of TB is 222 per 100,000 in 2020, this makes Tanzania among the top 22 high-burden countries with TB worldwide. 2 TB usually affects the lung, but about one-third of patients have extra-pulmonary involvement which include female genitals organs and other organs. 4 Extra-pulmonary TB is shown in a greater proportion of new cases in developed countries, and this trend is increasing.4,5
The research in TB in developed countries may be explained by the increase of immigrants from areas where the disease is endemic, as well as with increasing prevalence of HIV infection. 6 People with latent TB infection are at a higher risk of progression to active disease if co-infected with HIV.
Genital TB is an indolent infection, whose common symptoms include pelvic pain, vaginal bleeding, amenorrhea, vaginal discharge, and infertility. A rare presentation comprises of abdominal mass, ascites, and ischio-rectal abscess. 7
There are limited data on optimal medical management of genital TB. Treatment guidelines recommend isoniazid, rifampicin, ethambutol, and pyrazinamide for the first 2 months and isoniazid, rifampicin for the following 4 months, 7 which was a similar treatment provided to our patient.
Surgical treatment which include total abdominal hysterectomy and bilateral salpino-oophorectomy is usually indicated for the patients with persistent pelvic mass, oracles of pain or bleeding after 9 months of treatment. Surgery should be performed at least 6 weeks after initiation of anti-TB medication and thus reduce the risk of post-operative complication. 7
Conclusion
Genital TB is not a common condition in women in developing countries and has been a diagnosis dilemma, however, should always be considered as differential diagnosis in women with persistent vaginal discharge or bleeding and infertility. We recommend that all patients with a positive Ziehl–Neelsen stain and menstrual abnormalities undergo aggressive evaluation for Genital TB such as diagnostic hysteroscopy, depending on availability in certain facilities.
Footnotes
Acknowledgements
The authors thank all the physician, pathologist, and staff who have worked very hard to take care of this patient. Also, they thank the patient for allowing us to learn from her clinical presentation
Authorship
All authors contributed to conceptualization, writing, and critical review of this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.