
Abstract
Maxillary sinus is frequently presented as a single space within each maxilla. It drains directly into the nose through the middle meatus. We are reporting the second rare case of a mucocele in a separate compartment of maxillary sinus in a 26-year-old patient without a history of facial trauma. The non-contrast computed tomography of paranasal sinuses showed an expansile right infraorbital cystic lesion developed in an upper lateral position of the maxillary sinus. An excision biopsy was performed, which showed histopathological findings of a maxillary sinus mucocele.
Keywords
Introduction
Paranasal mucocele develops as an obstructive complication of chronic sinusitis, tumor, or trauma at paranasal sinuses. Frontoethmoidal mucoceles are considered the most common ones to be developed, whereas maxillary and sphenoid sinus mucoceles are rare. 1 When mucocele gets infected, it usually turns into pyocele that contains pus cells. 2
Accumulation of the mucus within paranasal cystic lesions leads to their expansion along with complications depending on their origins and direction of expansion. Because of the orbit proximity and thin wall of lamina papyracea, ophthalmologic manifestations are common to be seen as proptosis, diplopia, visual disturbance, periorbital swelling, and edema.3,4 The anatomic location of ethmoid and sphenoid sinus mucoceles can cause disturbance of the optic nerve function, thus resulting in irreversible damage without appropriate surgical intervention.4,5
We are presenting a rare case of a mucocele developed in a separate compartment of the maxillary sinus without any facial trauma. The previous literature only showed one similar case. 6
Case report
A 26-year-old male referred from the ophthalmology clinic for non-contrast computed tomography of paranasal sinuses (NCCTPNS) presented with complaints of headache, right visual disturbance, and right cheek swelling for 2 months duration (Figures 1–3).

Non-contrast computed tomography of paranasal sinuses (NCCTPNS) axial section.
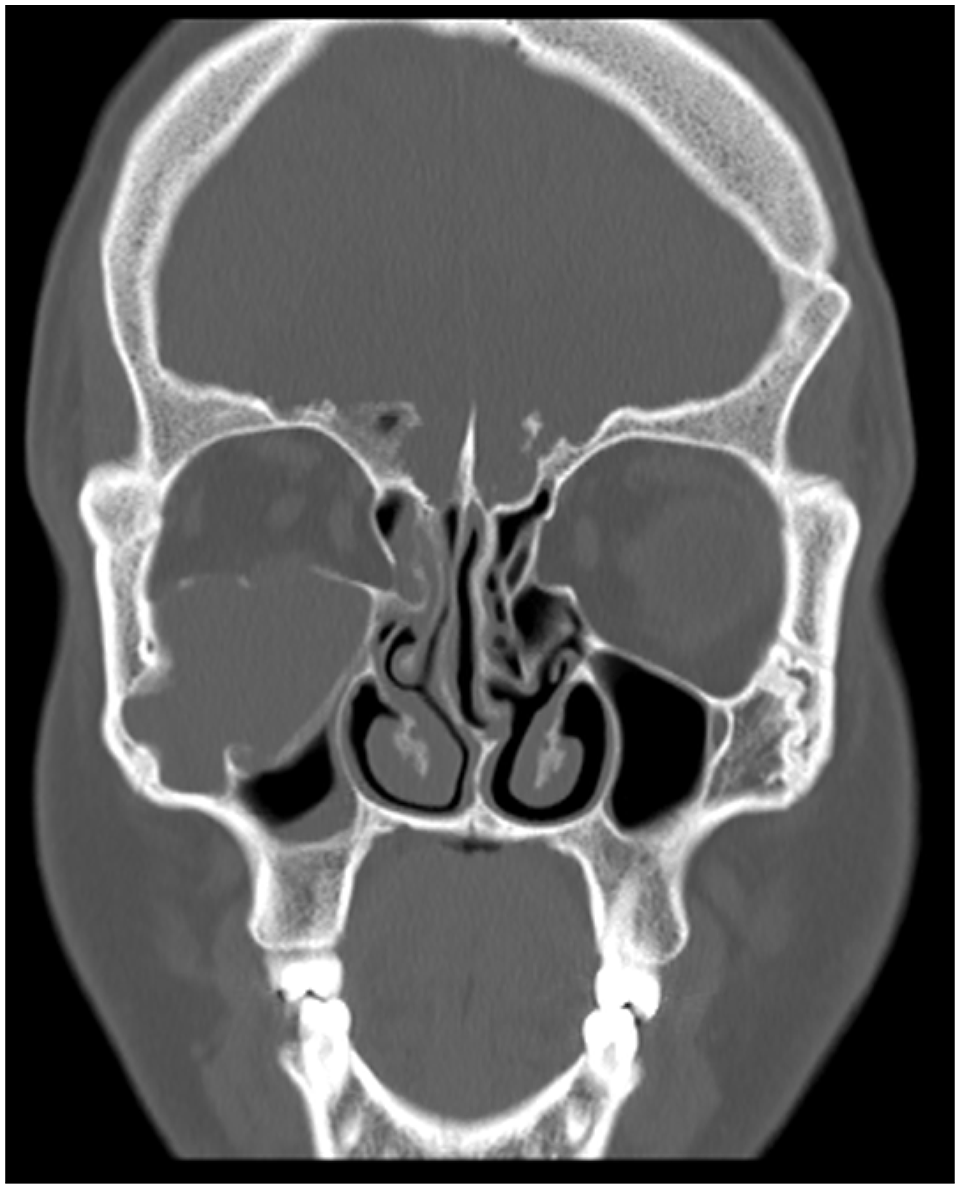
NCCT PNS coronal section.

NCCT PNS axial section.
Despite treatment with analgesics, the patient continued to experience a persistent headache. The patient denied anyfacial trauma or sinonasal surgery. Furthermore, he reported no significant health problems. Physical examination revealed a large, firm, and non-tender swelling over the right cheek. Laboratory investigations including a blood panel, liver function tests, and renal function tests were within normal range.
Management of our patients was in the form of surgical intervention with right endoscopic sinus surgery. Under general anesthesia, the rigid nasal endoscopy was performed. The middle concha is medialized to better expose the ostiomeatal complex. Uncinectomy and middle meatal antrostomy were performed to better expose the maxillary sinus to obtain an access to the mucocele which was completely excised with a yellowish to brownish mucus content. Histological sections of the cyst lining revealed stratified squamous epithelium resting on a fibrous stroma (Figure 4). For the postoperative period, amoxicillin 500 mg was prescribed every 8 h for 5 days and ibuprofen 400 mg every 6 h for 3 days as analgesic and anti-inflammatory agent. The patient’s symptoms had completely resolved post-operatively in 2 months duration.

Photomicrograph of the excised maxillary sinus mucocele shows a cystic cavity lined by pseudostratified ciliated columnar epithelium rested on fibrous stroma (magnification 200×).
Discussion
Maxillary sinus usually develops as a single space within each maxillary bone, which drains directly into the nose through the middle meatus. Sometimes, partial bony septations have been identified within the maxillary antrum, dividing it into two or more communicating recesses or compartments. Rarely to view a complete bony septum that can completely divide the sinus into two separate compartments, each of which drains via its own ostium into the nasal cavity. Moreover, it is extremely rare to see a completely isolated walled-off separate sinus compartment or recess. 6 In general, mucocele develops gradually and has a higher incidence between the third and fourth decade of life, and there is no reported sex predilection.4,5
Here, we are presenting a rare case of double maxillary compartments, with a mucocele developed in the superiorly located one. To the best of our knowledge, only one case of a separate maxillary antral mucocele superolateral to the other maxillary antral compartment has been reported. 6 While the previously reported case had a history of a preceding facial trauma, our case shows no history of facial trauma. Another two cases of separate maxillary antral mucocele located posteriorly to the main maxillary sinus compartment were reported by Som et al. 7 The authors interpreted this radiographic finding as “sinus within a sinus.”
East 8 hypothesized such compartmentalization may develop naturally without trauma or surgical intervention, thus accounting for some mucoceles developing de novo, as in our reported case. However, such cases are considered very rare.
Various cystic lesions could develop because of the anatomic variations in the area between the orbital floor, maxillary sinus roof, and posterior ethmoidal air cells. They include extra maxillary antral lesions as neuroma of the infraorbital nerve, cavernous hemangioma of the infraorbital canal, Haller’s cell mucocele, mucocele of a septate compartment of the maxillary sinus, or mucocele arises from the maxillary sinus proper that pushes the roof of the antrum superiorly.9–11
In our case, the detected infraorbital maxillary mucocele does not show any draining pathway to the nasal cavity or connection to the inferiorly located maxillary sinus. It is seen laterally extending into the zygomatic process of the right maxilla and is not related to the orbitoethmoidal air cell’s location.
Som and Shugar 14 suggested that postsurgical intervention and postoperative adhesions may divide the antrum into two or more compartments or recesses. These walled-off compartments are considered to be ideal environments for mucocele development.
Maxillary sinus mucoceles mostly develop late as long-term complications of Caldwell Luc operations or following trauma. Endoscopic surgery is the best treatment option for mucocele in ethmoidal, maxillary, and sphenoidal sinuses, as they can be reached via the nasal cavity.12–14
Conclusion
Our case illustrates a rare congenital maxillary sinus compartment without identified ostium. Retention of mucous within a closed space results in its expansion and predisposition to atypical isolated mucocele development that supports the theory of mucocele pathogenesis.
Footnotes
Acknowledgements
We would like to thank the surgical team at Sharm-Elsheikh International Hospital for their valuable contribution to this case.
Author contributions
All authors had a role in writing and revising this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Patient’s consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.