
Abstract
Omental infarction is a rare but a sinister cause of acute abdomen. Preoperative diagnosis is challenging due to its rare nature. It poses nonspecific abdominal signs that can be easily mistaken with other more common intra-abdominal pathologies. We report a case of a 37-year-old male patient presented with right lower quadrant abdominal pain with an elevation of inflammatory markers. His cross-sectional imaging did not a reveal specific diagnosis; therefore, a diagnostic laparoscopy was performed which revealed a non-inflamed appendix and an inflammatory mass formed by the ischemic omentum attached to the ascending colon. Diagnostic laparoscopy and subsequent laparotomy revealed spontaneous omental infarction. The histology of the resected specimen was in keeping with the omental necrosis. This case reflects the importance of considering omental infarction in patients presenting with abdominal pain and raised inflammatory markers. He made an uneventful recovery following surgery.
Introduction
Spontaneous omental infarction is a rare cause of acute abdomen. The causes can be categorized as primary and secondary. Secondary omental infarction occurs following omental torsion, commonly due to tumor, hernia, localized inflammation, trauma, postoperative adhesions, and other rare causes such as vasculitis, polycythemia, hypercoagulability, and thrombophilia.1–3 It comprises 0.1% of all laparotomies performed for acute abdomen, with a higher incidence in males than in females, common in the “40–50yr” age group. 4 In comparison with secondary omental infarction, the aetiology of primary omental infarction or spontaneous omental infarction is still not clearly understood.
Preoperative diagnosis of omental infarction from other causes of acute abdomen such as appendicitis and acute cholecystitis is challenging as it is clinically indistinguishable. As it is a benign and a mostly self-limiting disease, an accurate preoperative diagnosis prevents the patient from going through the risks of surgery. Therefore, it is important to consider it in the differential diagnosis of a patient presenting with acute abdomen. We present a rare case of spontaneous omental infarction discussing the course of diagnosis and management.
Case presentation
A 37-year-old ASA1 male patient presented with right lower quadrant abdominal pain for 3 days. He did not have a history of fever, nausea, anorexia, urinary tract symptoms, or altered bowel habits. His past surgical history was unremarkable. On physical examination, general examination was unremarkable without pyrexia. On admission, he was hemodynamically stable with pulse rate of 88/min. The abdominal examination revealed significant tenderness and guarding in the right lower quadrant. There was no tenderness over the McBurney’s point. 5 His basic serum biochemistry revealed a mild elevation of the leucocyte count (12.12 × 103/uL) with a marginally elevated C-reactive protein level of 13 mg/L. His liver, renal profiles, electrolytes, serum amylase random blood sugar, and urinalysis were within the normal range. Further investigation with ultrasound abdomen was inconclusive. Initially, he was observed for 24 h with analgesia and resuscitated with intravenous fluids. His analgesic regimen included paracetamol and nonsteroidal anti-inflammatory medications. Subsequently, on 48 h, his clinical status was deteriorated with persistent, progressively worsening pain, increased abdominal tenderness, guarding over right lower quadrant, tachycardia (pulse rate of 120/min), and a fever spike of 101 F. The repeat leucocyte count and C-reactive protein level increased to 16 × 103/Ul, 79 mg/L, respectively. Therefore, he was started on intravenous co-amoxiclav, resuscitation continued with intravenous fluids and vital parameters were monitored.
In view of clinical deterioration and equivocal findings in ultrasound, an emergency computed tomography (CT) abdomen was performed. It showed a thickened area adjacent to right colon with fat stranding (Figure 1). In view of clinical deterioration an equivocal finding on cross-sectional imaging, laparoscopy was performed on day 2 after admission. On survey, the appendix was not inflamed. However, there was an inflammatory mass consisting of necrotic omentum adherent to the mid-ascending colon (Figure 2). There was no evidence of omental torsion. The omentum was dissected off with diathermy, and the right colon was mobilized medially. The surgery was converted to a mini-laparotomy via midline incision as complicated diverticular disease could not be safely excluded on laparoscopy. Omental attachment to ascending colon was released, and omentectomy (Figure 3) was performed along with an appendicectomy. No perforations were noted in the ascending colon. The histology of the omental specimen revealed lobules of adipose tissue showing septal necrosis, a mild-to-moderate infiltrate of acute and chronic inflammatory cells and fat necrosis in the adjacent lobules (Figures 4 and 5). Hemorrhagic areas with hemosiderin-laden macrophages were present without any evidence of thrombi, granuloma formation, or malignancy. These features were in keeping with omental infarction with secondary inflammation. The appendix was histologically unremarkable. He made an uneventful recovery and was discharge on the fourth post-operative day. Three weeks following surgery, he underwent a colonoscopy which revealed normal colonic mucosa without evidence of inflammatory bowel disease or colonic diverticuli. Subsequently, he underwent thrombophilia screening, which was unremarkable.

CT abdomen showing thickened area adjacent to right colon with fat stranding. (a) Coronal view, (b) Axial view.

Laparoscopic images showing necrotic omental mass with inflamed peritoneum over anterior abdominal wall.

Necrotic segment of omentum.

Lobules of omental fat showing areas of necrosis. H&E × 40.
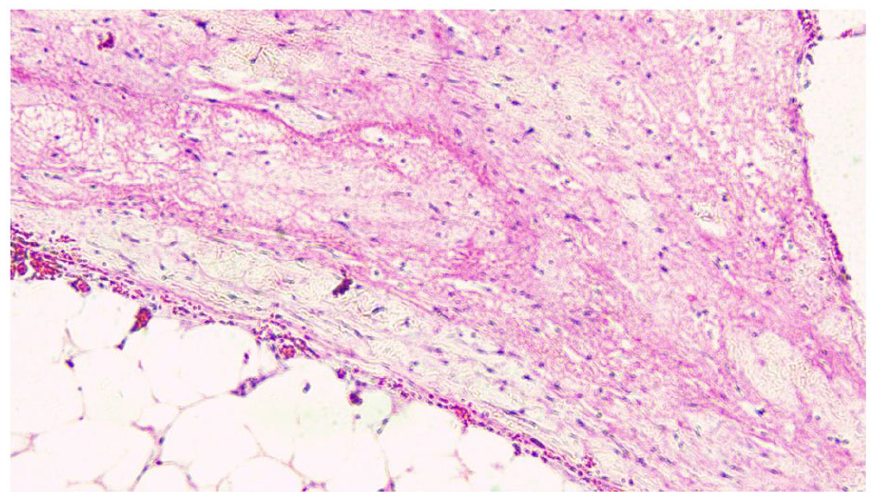
Areas of fat necrosis. H&E × 100.
Discussion
Omental infarction is a rare cause of acute abdomen. The diagnosis is challenging due to unfamiliarity, nonspecific nature of symptoms. Of the reported cases of spontaneous omental infarcts, up to 15% are paediatric. 6
Corvino et al. 7 describe predisposing factors for primary torsion of the omentum, such as omental vascular abnormalities, small root, physical strain, cough, disorders of hemostasis, and hematological abnormalities. The other possible mechanisms suggested are the anomalous arterial supply of the omentum, vascular congestion following ingestion of a large meal, and kinking of veins secondary to increased intra-abdominal pressure. 7 Pathogenesis related to disruption of blood supply causing spontaneous omental infarction is still not known. However, when the right half of the omentum contains altered vasculature, it is less tolerant of spontaneous venous stasis leading to an increased likelihood of thrombosis of omental veins even following slight stretch. 8 In obese children, omental infarction is attributed to adipocytic accumulation within the omentum, impeding the flow of distal right epiploic artery. 9 However, depending on its location the greater omentum can cause site-specific pain as explained by our patient’s presentation with pain in the right lower quadrant of abdomen.
It is commoner on the right side, with most presenting with acute or sub-acute abdominal pain. 2 Abdominal examination may rarely reveal a mass with localized tenderness, which often mimics the presentation of acute appendicitis. The incidence of right colonic diverticular disease is significantly higher in Asian countries. 10 In our patient, we considered right-sided complicated diverticular disease also as differential diagnosis. We had to consider this fact in operative planning of our patient and during intraoperative decision-making.
CT abdomen would occasionally show an ovoid, well-circumscribed soft tissue mass representing the omental fat. Ultrasound may show an oval- or triangular-shaped hyperechoic lesion corresponding to the greater omentum, but CT would usually reveal a mass of mixed attenuation due to the fatty and non-fatty elements of the mass.11,12 CT abdomen is used in several studies for the accurate localization of the pathology.13,14 Concentric linear strands or the “whirl” sign with hyper attenuated streaky infiltration are the radiological signs specific to omental infarction and torsion.In our patient these features were not evident.
Spontaneous omental infarction is a self-limiting condition, and given the associated risks of surgery and anesthesia, surgery is not considered the first line of therapy. 15 Literature reveals that omental infarction can be successfully managed non-operatively and surgery should be reserved for those with deteriorating symptoms. 15 White cell count more than 12 × 103/uL and young age are factors associated with failure of conservative management. 16 This was evident in our patient too, who required surgical intervention. A systematic review by Gallardo et al reveals that surgical management has a shorter duration (mean hospital stay 2.5 days vs 5 days) of hospital stay when compared to conservative management, which is effective in most. 16 Furthermore, the study favors a laparoscopic approach due to its safety and shorter hospital stay. 16 Surgical approach is associated with shorter duration of pain which otherwise would last for an average of 13.5 days with conservative management. 8 Furthermore, conservative management is associated with a 15.6% failure rate with patients being subsequently treated with laparoscopy. 16 After initial resuscitation, antibiotics are not recommended in literature, however since the diagnosis is usually missed most end up using antibiotics.8,17,18 In the present case, a surgical approach was assumed due to the worsening of symptoms with moderately raised inflammatory markers and inconclusive imaging evidence. However, it is recommended in literature that following conservative approach close monitoring for deterioration of symptoms should be done for 48 h and surgery be considered with evidence of clinical deterioration.14,18 A conservative approach is preferred in paediatric patients due to the benign course of the condition and the fact that it can be safely managed with analgesia in most cases. 7
To date, there are no guidelines to suggest the best treatment modality for omental infarction. Furthermore, controversies exist regarding the decision for conservative or surgical management. The literature is limited to only case reports and case series, which highlights the importance of further research to raise awareness. This case highlights the importance of considering spontaneous omental necrosis as a differential diagnosis especially in clinical situation of right-sided acute abdominal pain.
Conclusion
Spontaneous omental infarction is a rare occult cause of acute abdominal pain which poses a diagnostic challenge as the clinical presentation is indistinguishable from other sinister causes of acute abdomen. Cross-sectional imaging is considered helpful in diagnosis, but can often be inconclusive. CT sensitivity and specificity are very high and are not often inconclusive; in fact, it is what helps guide the diagnosis. It is managed conservatively where surgery is considered later in the course of management. During laparoscopic exploration, it is difficult to differentiate between complicated diverticular disease on right colon from omental infarction. Timely surgical intervention is required in patients with clinical deterioration.
Footnotes
Acknowledgements
The authors wish to acknowledge the ward staff who took care of this patient.
Author contributions
DS designed the manuscript and took primary care of the patient. DS and RJ wrote the manuscript. DS critically analyzed the manuscript. UK involved in image interpretation, and GR helped with histopathology report. All authors read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.