
Abstract
Cervical leiomyoma is a relatively uncommon type of uterine leiomyoma. Prolapse of a cervical leiomyoma with inversion of the cervix is an extremely rare phenomenon, especially in a non-puerperal woman. Only a handful of cases are reported in the English literature. The case discussed here is of a vaginal prolapse of a submucous cervical fibroid complicated by cervical inversion in a South Asian perimenopausal woman with multiple comorbidities who had defaulted medical follow-up during the second wave of the COVID-19 pandemic. Being one of the largest reported cervical fibroids to date is another particularity of this case. Emphasis is given to the clinical diagnostic, anaesthetic, and surgical challenges encountered with a brief note on the impact of COVID-19 on outpatient clinic follow-up.
Introduction
Uterine fibroids are the most common neoplasm of the genital tract in females of reproductive age, classified according to the site of occurrence: subserosal, submucosal, intramural, and hybrid types. 1 Despite being benign tumours, the complications of leiomyomas are not uncommon, largely determined by their location and size, including abnormal uterine bleeding, abdominal pain, increased abdominal girth, urinary frequency, pregnancy loss, and infertility. 2 Asymptomatic, slow-growing fibroids are seen among perimenopausal women constituting 30% of the total. 3 The prevalence of cervical leiomyomas is considered to be less than 5% 4 where abnormal uterine bleeding, dyspareunia, and constipation are common presentations. 5 Although very rare, acute yet more serious complications such as vaginal prolapse, thromboembolism, acute torsion, urinary retention and renal failure, vaginal or intraperitoneal haemorrhage, mesenteric vein thrombosis, and bowel gangrene could lead to serious morbidity and mortality, suggesting the need for close follow-up and conservative or definitive therapy as indicated. 6 The probability of prolapse increases among submucosal and pedunculated fibroids. Complications specific to prolapsed fibroids include necrosis due to reduced blood supply (from the pedicle) and sepsis. 7 Concurrent cervical inversion in the non-puerperal period is an extremely rare occurrence, especially in the absence of uterine malignancy, with only a few cases reported in the literature.4,8
Herein, we present a case of vaginal prolapse of a large cervical fibroid with the inversion of the uterine cervix requiring excision vaginally and transabdominal hysterectomy with a brief discussion on surgical techniques adopted in such settings, anaesthetic goals, and the effect of COVID-19 on outpatient follow-up.
Case presentation
A 48-year-old South Asian mother of two, a diagnosed patient with hypothyroidism, type 2 diabetes mellitus, and hypertension presented to the routine gynaecological clinic with complaints of progressive aching type lower abdominal pain and heavy menstrual bleeding for 3 months. Initial abdominal examination revealed a large uterine mass of 20 weeks’ size. An ultrasound scan of the pelvis revealed a large uterine cervical fibroid measuring 300 mm × 90 mm × 10 mm. Her haemoglobin level was 9.1 g/dL, and the initial clotting parameters were normal. She was prescribed symptomatic medication to control vaginal bleeding, oral iron therapy, and analgesics and discharged with an early date for myomectomy and instructions to attend an outpatient gynaecology clinic during the waiting period (6–8 weeks), for which the patient defaulted. After 3 months, the patient presented to the emergency treatment unit with complaints of acute severe lower abdominal pain, vaginal bleeding, and a lump at the vulva. On examination, she was afebrile, in pain (visual analogue scale 6), mildly pale, and tachycardic with a pulse rate of 120, and had normal non-invasive blood pressure (130/80 mmHg). Her body mass index (BMI) was 27 kg/m2. On vaginal examination, there was a large friable, prolapsed uterine fibroid with apical necrosis, tightly impacted vaginally (Figure 1).

Prolapsed cervical leiomyoma impacted at the vaginal introitus. (a) The degenerative changes of the tumour at the apical segment.
The bimanual examination of the pelvis was not possible. Her haemoglobin level was 7.8 g/L. The platelet count and the coagulation profile were normal. Random capillary blood sugar measurement was 250 mg/dL with normal acid-base status and lactate level (<2 mmol/L). She was clinically euthyroid. The most recent thyroid-stimulating hormonal assay was 1.9 mIU/L (0.4–4). Hyperglycaemia was corrected by subcutaneous soluble insulin (6 units). The patient was scheduled for an urgent vaginal myomectomy and abdominal hysterectomy after a detailed explanation of the anaesthesia and surgery and informed written consent. Her fasting was completed for solids. The provision of analgesia with subcutaneous morphine 6 mg, intravenous paracetamol 1 g, and resuscitation with one unit of packed red cells was carried out.
The surgery was done under general anaesthesia. Core body temperature was maintained above 35°C. The pelvic examination was conducted revealing the inverted cervix covered by the prolapsed fibroid. The fibroid was resected vaginally with a gentle pull and the distorted cervix was isolated (Figures 2 and 3).

Resected leiomyoma.

The resected myoma and the uterus: (a) resected cervical myoma, (b) uterus, and (c) uterine cervix. Note the altered architecture of the uterine cervix.
Transient bradycardia (which was anticipated) of 45 beats per minute was managed with temporary discontinuation of the procedure and intravenous atropine of 0.8 mg. The uterus and adnexa were in normal confines and a routine abdominal hysterectomy with salpingectomy was performed via a Pfannenstiel incision (Figure 4).
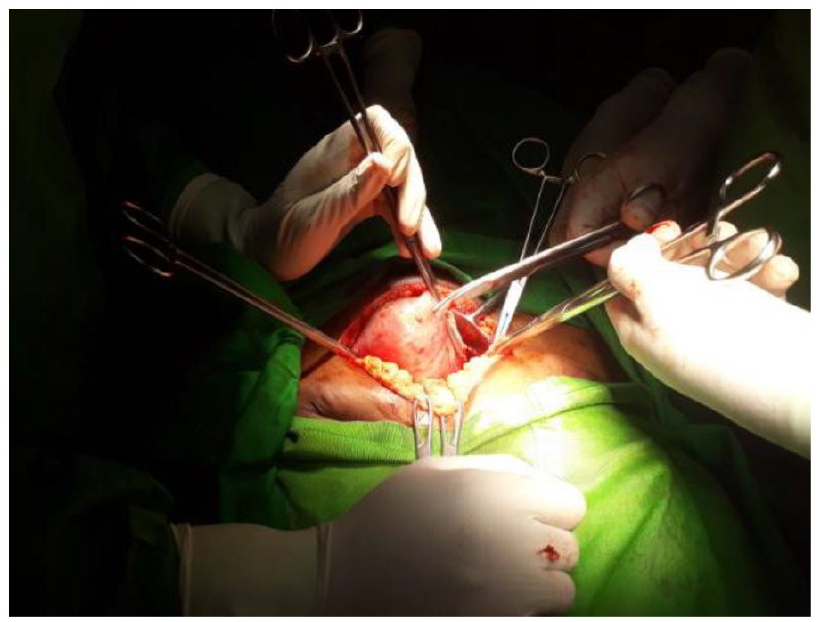
Abdominal approach for the hysterectomy and salpingectomy.
The bilateral ovaries were preserved. The resected specimen was sent for histopathology. The estimated blood loss was 1 L for which another unit of packed red cells was transfused. The patient was sent to the ward following extubation of the trachea. Glycaemic control was achieved with a basal-bolus regimen. The surgical site was closely monitored for infection. Enhanced recovery protocol was followed and she was discharged after 3 days with oral iron treatment. The histopathological report revealed a cervical submucous fibroid of 300 mm × 150 mm × 100 mm with degenerative changes and a distorted cervix measuring 35 mm in length. Microscopically, the typical appearance of a leiomyoma with the degenerative changes was noted (Figure 5(a) and (b)).

(a) Interlacing fascicles of smooth muscle bundles (H&E, ×10) and (b) spindle cells with bland nuclei in myxoid stroma (H&E, ×40).
Discussion
Being the most prevalent benign neoplasm of the female uterus, leiomyomas have a prevalence of 40% at 35 years in Caucasian women, with a peak incidence between the ages of 35–40. It accounts for one-third of gynaecological-related admissions. 1 The growth of leiomyoma is thought to be influenced by oestrogen, progesterone, growth factors such as insulin-like growth factors, and transforming growth factor-beta. 2 The degree of prolapse outside the uterine cavity is variable. It might partially prolapse into the cervix, completely into the vagina, or outside the vagina and the introitus. 9 Most prolapsed leiomyomas are small but variable in size, between 1 and 6 cm in diameter. There are a few case reports in the literature of large prolapsed leiomyomas of more than 10 cm in diameter. 4 The factors affecting the inversion of the fibroid uterus include thinning and weakening of the uterine wall at the seating point of the tumour implantation due to the pressure atrophy; the larger the tumour, the more the pressure effect and the risk of prolapse. The contractions of the uterine musculature excited by the tumour promote prolapse. 10
What makes this case distinctive is that apart from the location itself, the size of the fibroid and the acute presentation of vaginal prolapse and cervical inversion are unusual. Cervical leiomyomas are a rare entity, so much so that it has been found in only 0.6% of hysterectomy specimens. 11 Similarly, only very few reported cases of non-puerperal cervical inversion occurred due to cervical myomas. In 2019, Ribeiro et al. 12 reported a cervical myoma of 12 cm × 9 cm in size, presented with cervical inversion which was managed with vaginal myomectomy, abdominal hysterectomy, and bilateral adnexectomy. In 2013, Turhan et al. 4 reported a case of 12 cm × 8 cm sized cervical fibroid with vaginal prolapse and cervical inversion which mimicked uterine inversion and was subsequently treated with a vaginal myomectomy and a vaginal hysterectomy. Furthermore, in 2013, another case of cervical myoma mimicking chronic uterine inversion was treated with open myomectomy and hysterectomy. 13
There is a lack of data linked with prolapse and inversion of the cervix in cervical fibroids. The size of the fibroid might be a precipitating factor similar to fibroids elsewhere. High BMI could be a risk factor. 1
In this patient, the clinical records of a cervical fibroid made the diagnosis easier in the most recent presentation; however, the differentiation of cervical inversion from uterine inversion can be challenging. 10 Clinically, the absence of uterus and adnexa in bimanual examination confirms the uterine inversion. In our patient, the bimanual examination was difficult due to the prolapsed fibroid completely occupying the introitus, necessitating examination under anaesthesia. Transabdominal ultrasonography might be a useful tool to confirm uterine inversion. A characteristic sonographic feature of complete uterine inversion is a ‘U’-shaped uterine cavity in the longitudinal plane. 14 The clinical diagnosis of prolapsed cervical fibroid and the decision to operate on an urgent basis precluded the need for ultrasonography in our patient. Even though a magnetic resonance imaging (MRI) scan would be indicated for the complete pre-op diagnosis, it was not performed in our patient due to the unavailability. A characteristic ‘broccoli sign’ will be demonstrated in the sagittal MRI view with vaginal prolapse of fibroid. 15 Added to that, it serves the diagnostic purpose of differentiating the mass from a malignant tumour, and the proper anatomical demarcations will be useful to determine the proper surgical approach.
In the case of our patient, the preoperative anaesthetic challenges were analgesia, optimizing her anaemia, and controlling hyperglycaemia. The surgical procedure consisted of two stages. At first, the myomectomy was performed vaginally and then the hysterectomy was done with a laparotomy. The process of removing a myoma requires three steps: devascularization, detachment, and removal. 16 Infiltrating the myoma with vasopressin might help to decrease blood loss. 17 The probability of malignancy increases with the size of the fibroid. If feasible, a frozen section is beneficial pre- or intra-operatively, to determine the presence of malignancy. 10 The technique was not available in our centre. The malignant transformation of a fibroid is extremely rare, and it is commoner for leiomyosarcomas to arise de novo with an incidence of around 0.23% rather than transformed from a benign tumour. 18 Hysterectomy is commonly practised simultaneously with myomectomy, especially in cases of large myomas, and if the patient has completed her family and is willing to lose her uterus,16,19 as in this instance. Furthermore, it was found that the uterus and all its attachments were stretched and pulled down. Therefore, the decision for a hysterectomy was taken as it was necessary to correct the inversion and prevent neurogenic shock. Additionally, there was a degenerated segment at the apex of the tumour with risk of possible sepsis. 20 Although laparoscopic hysterectomy is a less invasive approach, the gynaecologist was more comfortable with the open approach in the given urgent setting. In English literature, there is one occasion where a large prolapsed submucosal fibroid had been resected vaginally while hysterectomy was completed laparoscopically. 21
The treatment method of fibroids depends on factors such as the patient’s future fertility wishes, the importance of uterine preservation, symptom severity, and tumour characteristics. 1 The surgery would be beneficial in abnormal uterine bleeding not responding to conservative treatment or which leads to iron deficiency anaemia, suspicion of pelvic malignancy, growth after menopause, infertility or recurrent pregnancy loss, pain or pressure symptoms that interfere with the quality of life commonly. Additional benefits for menopausal women following hysterectomy for myomas include elimination of the need for pregestational agents, the ability to take oestrogen without experiencing bleeding, and lessened concerns about myoma growth during oestrogen replacement. The need for routine gynaecology follow-up after hysterectomy is also simplified, compared with frequent visits required to assess of myoma growth during conservative therapy. 22
Apart from the conventional general anaesthesia, there are instances where central neuraxial blockade has been utilized for myomectomy. According to Nnaji et al., in a 5-year audit done in a hospital in Nigeria, among a total of 202 anaesthetic services offered for abdominal myomectomy during a 4-year period, 79% had been under general anaesthesia, while 15%, 4.5%, and 1.5% were under spinal anaesthesia, spinal with general anaesthesia combination, and combined spinal-epidural anaesthesia, respectively. However, the specific indications for these less preferred anaesthetic methods were not mentioned. 23
Our patient had defaulted clinic follow-up during the second wave of the COVID-19 pandemic. In this instance, although the underlying anaemia with ongoing heavy menstrual bleeding was indicated for early surgery, due to the prevailing COVID-19 crisis, we were compelled to postpone surgeries except for malignancies as per local hospital protocol to divert human resources, drugs, and equipment for COVID-19 care. Our patient was medically managed during this period with ovulation suppression (oral Progesterone) and oral haematinics.
Various studies have shown that routine clinic attendance and hospital admissions have declined by 15%–80% in various specialities. Furthermore, the negative economic impact that had on the general population24,25 and the common general attitude towards the investigations (COVID-19 polymerase chain reaction testing/rapid antigen testing) may have affected the patient to default. 26 Thus, it is vital to educate the patients regarding the importance of routine follow-up and to seek healthcare early in cases of acute deterioration during such global-scale health-related calamities.
Conclusion
Although leiomyomas are common among women worldwide, cervical leiomyomas are a comparatively uncommon entity. In this article, we have presented a rare case of vaginally prolapsed large cervical fibroid complicated with cervical inversion which required vaginal myomectomy and transabdominal hysterectomy. While appreciating the extreme rarity of the case, attention should also be directed to the factors for patients to be followed up poorly in clinical settings such as the prevailing COVID-19 pandemic to avoid poor outcomes.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of the Gynaecology and Anaesthetic teams of the institution during the management of this patient.
Author contributions
D.A.C.T.C., B.M.M., and E.J.P. managed the patient. All were involved in the conception of the case report. D.A.C.T.C. and B.M.M. drafted the manuscript. All were involved in the critical analysis of the manuscript. All authors approved the final manuscript and certified the originality of the manuscript.
Availability of data and material
All data analysed during this study are included in this published article. Requests for material should be made to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.