
Abstract
Baseball is unique in its multiple facets: pitching, hitting, base rounding, and fielding are distinct activities that require different athletic skills to perform at a high level. Likewise, these different aspects of the game can contribute to a multitude of varying injuries. While high-velocity overhead throwing, along with batting, can produce a plethora of upper extremity injuries that often garner attention, injuries to the lower extremity can severely impact a player’s performance and ability to compete. The rigors of the short, explosive sprinting required for base running, as well as the dynamic movement required for fielding, create ample opportunity for lower limb injury, and even subtle pathology can affect a pitcher’s ability to perform or increase their long-term risk of injury. Chronic injury from conditions such as femoroacetabular impingement and hip labral tears can also occur. The purpose of the present review is to summarize the relevant epidemiology, pathophysiology, and treatment of lower extremity injuries in baseball athletes, with reference to current research into the prevention and management of such injuries.
Keywords
Introduction
Baseball remains one of the most popular sports in North America and is commonly played by athletes at the high school, collegiate, and professional level. The sport is characterized by activities such as pitching, batting, and fielding, with throwing and sprinting fundamental for all participating athletes. With baseball being a throwing sport, there is significant attention in the sports medicine literature on upper extremity injuries in baseball, as baseball is known for characteristic injuries to the shoulder and elbow.1–3 However, high-energy lower extremity (LE) activity, which includes sprinting to round bases, sliding, jumping to catch, and the execution of a pitch, contributes to a relatively understudied incidence of LE injuries in baseball players.4,5
LE injuries are the most common type of injury seen in sports as a whole, consistent across all levels of play. 6 The multiple phases of baseball, which include batting, base running, pitching/throwing, and fielding, each present with unique demands that individual athletes can rapidly cycle through, all with the potential to produce injury. Sliding, in which players make either an aggressive head-first or feet-first dive toward a plate, can result in LE injury, with ankle injuries accounting for 23.8% of feet-first slide injuries. 7 Hip dynamics are heavily involved in the throwing process, particularly among pitchers, while swift running in the outfield can contribute to a multitude of acute and chronic pathologies of the thigh and knee.4,8 Epidemiological studies into the rates of LE injuries in baseball players have been carried out at the level of collegiate baseball, Minor League Baseball (MiLB), and Major League Baseball (MLB), as well as collegiate softball.4,5,9–11 An investigation of the MLB disabled list (DL) between 2002 and 2008 by Posner et al. 4 identified 30.6% of total MLB injuries to be of the LE, with lower limb injuries accounting for 47.5% of fielders’ injuries versus 16.9% of pitchers’ injuries. Of these injuries, the hamstring was the most common region, and rates of injuries have continued to rise despite advances in training, diagnosis, and management. In pitchers specifically, Marshall et al. 9 found LE injuries to account for 14% of all injuries resulting in placement on the DL during the 2014–2015 season, with LE conditions resulting in less missed time on average than upper extremity injuries. A similar study of the MLB DL between 2010 and 2016 found LE injuries to represent 29.7% of total reported injuries, consistent with the rates previously observed, with an average of 45.7 days of play missed. 5 The thigh, consisting of the quadriceps and the hamstring, was the most commonly injured area (42% of LE injures). At the collegiate level, McFarland and Wasik 10 found 27% of baseball injuries to occur in the LE (Table 1).
Summary of lower extremity (LE) findings in baseball injury epidemiological studies.
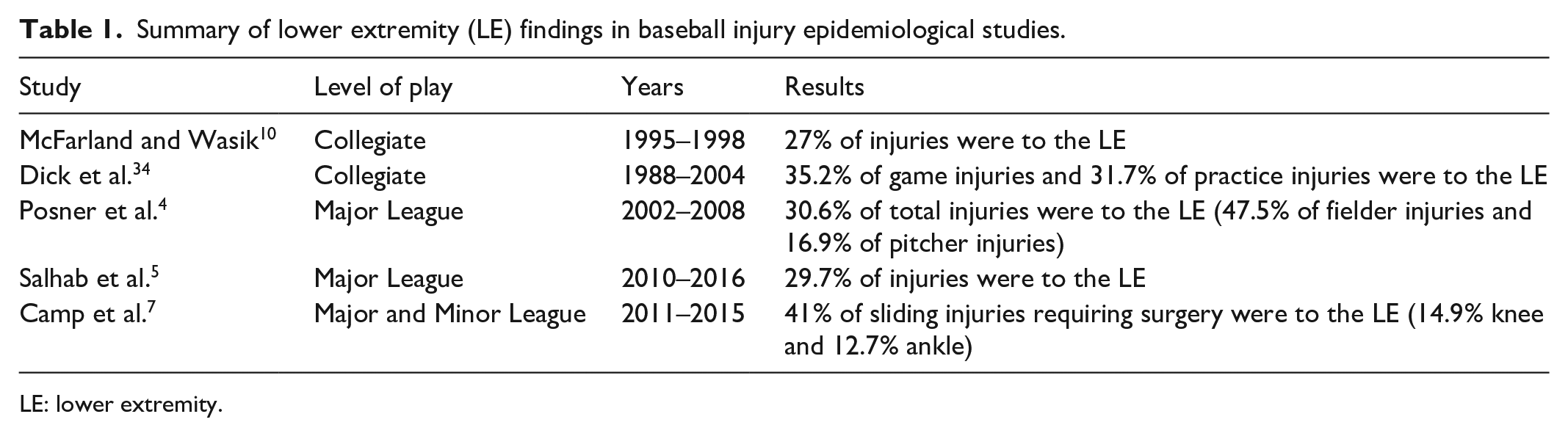
LE: lower extremity.
Management of athletic injuries is multidisciplinary and often requires shared understanding and expectations between athletes, athletic trainers, physical therapists, and physicians. Despite the increasing body of literature examining the epidemiology of such injuries and increased attention toward management and prevention, there are no comprehensive reviews of LE injuries to consolidate this evolving field of research. This study seeks to review the common LE injuries experienced by baseball players across competitive levels, with emphasis on the epidemiology, pathophysiology, and management of these injuries.
Methods
Two authors (D.A.H. and J.D.M.) searched PubMed/MEDLINE and the Google Scholar academic databases utilizing the Boolean search terms (baseball hip) OR (baseball hamstring) OR (baseball thigh) OR (baseball knee) OR (baseball calf) OR (baseball ankle) OR (baseball foot) on 29 July 2021. Exclusion criteria included duplicate studies, studies published in a non-English language, and studies not focused on the LE or the throwing athlete, as well as the studies that were purely biomechanical or performance-based and did not address injuries or pathology. The final articles were selected by the authors as the most relevant for inclusion in this review, with preferential subjective selection of epidemiological studies, pertinent reviews of major injuries, and randomized controlled trials of treatment modalities (Figure 1).
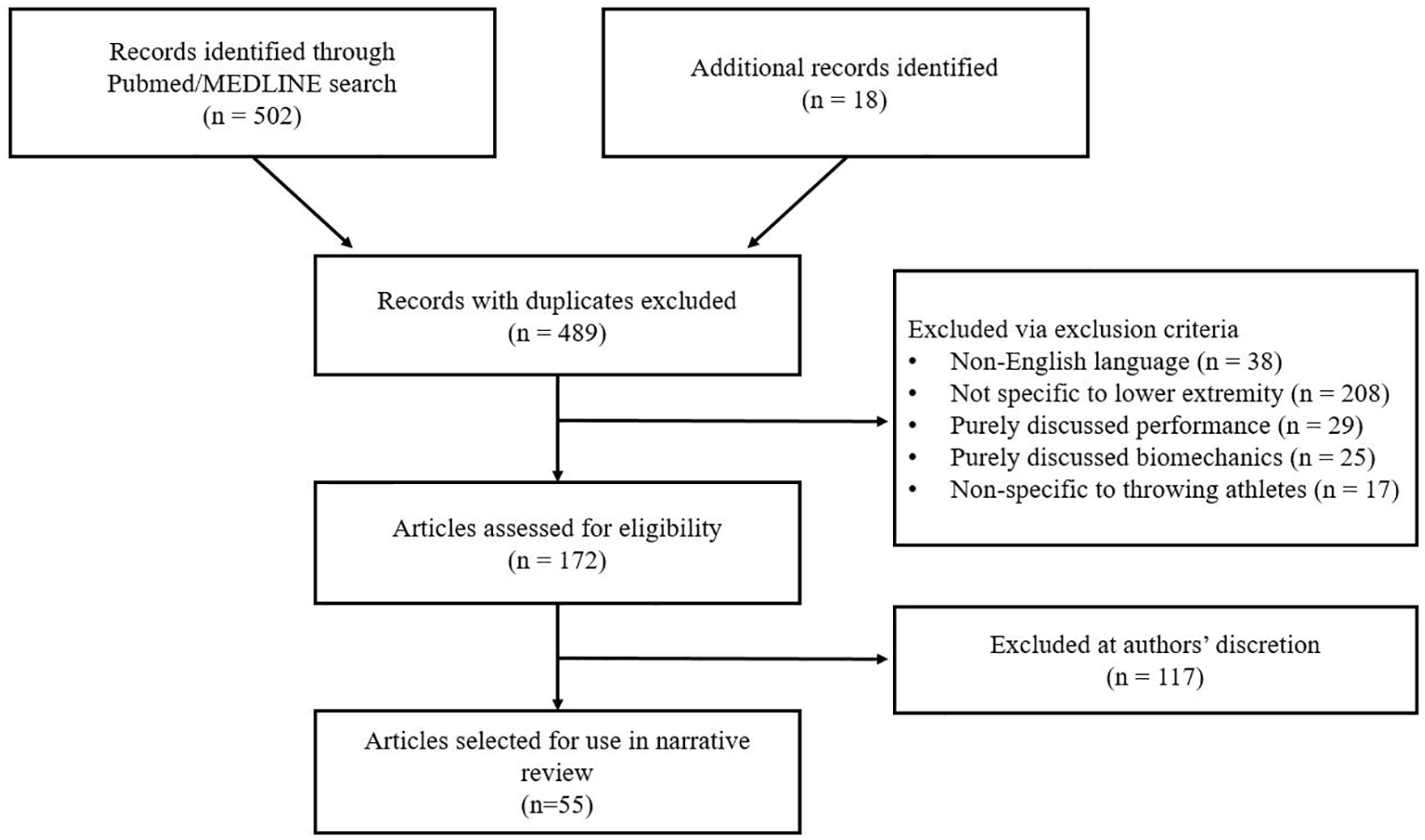
Flow diagram illustrating results of search query and exclusion of articles based on prespecified criteria.
Hip
The hip joint and surrounding musculature is fundamental in generating the force required for explosive athletic activities and play an important role in all phases of baseball. The hip has been extensively studied for its essential role in the overhead throwing kinetic chain, and misalignment of hip mechanics can contribute to both downstream chronic issues and an increased risk of acute injury in multiple body parts.13–16 In addition, the hip is responsible for quick pivot movements of the trunk and pelvis, and these movements may be required in the field to track a fly ball or turn a double play. The active use of the hips in baseball can lead to the development of both acute injuries and chronic pathology, not only within the hips themselves but also throughout the kinetic chain. 17
Proper hip range of motion (ROM) and kinematics are well regarded as integral to proper baseball mechanics. The hips are crucial in developing force during batting, primarily during the acceleration phase following swing initiation during which the lead hip undergoes maximum external rotation, while the trail hip undergoes maximum passive extension during swing follow-through. 18 The role of hip mobility and strength has been studied even more extensively in relationship to overhead throwing mechanics. 13 During the first two stages of the overhead throwing motion as defined by Fleisig et al., 19 windup and stride, the lead leg of the thrower is raised and then extends out to contact the ground. This motion produces hip internal rotation by positioning the trunk over the stance leg, and generates force for the pitch via forcible external rotation and extension of the lead hip.
Adequate hip rotation is clearly required to achieve maximal rotational forces while pitching and hitting in baseball. 20 Sauers et al. 13 found healthy baseball players have been shown to display hip ROM considered by the authors to be within a normal range (average if 37.0–37.7 degrees of internal rotation, 30.8–32.8 degrees of external rotation), suggesting that the sport does not inherently produce maladaptive kinetics or asymmetries. Likewise, the femoral torsion angle of elite baseball players was found to be similar between healthy and unhealthy players across positions, suggesting that limitations in hip ROM are likely associated with soft tissue imbalances or specific bony pathology, such as femoroacetabular impingement (FAI). 16 The musculature of the hip joint is linked intrinsically to the core, with stable rotation influencing the timing and dynamic motion of the glenohumeral joint during the subsequent stages of throwing (arm cocking, arm acceleration, ball release, and arm deceleration). Oliver and Keeley 14 found the rate of pelvis and torso axial rotation to be strongly correlated with shoulder elevation in high school pitchers, with an unstable core producing increased angles of abduction, placing these athletes at increased risk of injury.
Disruption of the kinetic chain, which originates from the hip, has been demonstrated in the literature to both adversely affect throwing mechanics and predispose baseball athletes to downstream injury.20–22 Fatigue throughout a season can alone be sufficient to disrupt hip kinetics, with overall decreases in hip ROM observed in both pitchers and position players as individual seasons progressed. 23 Decreased internal rotation ROM while the hip is at 90 degrees of flexion has been identified as a risk factor for shoulder, elbow, back, groin, abdominal, and hamstring injuries in baseball players.20,24–26 Reduced ROM or hip instability results in subtle, maladaptive compensation throughout the throwing motion, as force that is not properly transmitted throughout the kinetic chain places an increased burden on the distal elements, resulting in accumulation of damage through repeated activity. In addition, injuries to the ulnar collateral ligament (UCL) have been correlated with hip/groin pathology both prior to and after UCL surgery, and although the nature of this relationship is not well-understood, it provides further evidence that altered hip mechanics can be related to both proximal LE injuries and dysfunction of distal kinetic chain components. 27 Conventional physical therapy techniques, including hip mobility drills, stretching, gluteus medius/minimus strengthening, and dedicated core stability work have been suggested as essential elements of baseball athletic training for injury prevention, particularly among high school athletes in which pelvic and core stability may be relatively underdeveloped.25,26
Aside from its importance to the kinetic chain, injuries to the groin and hip joint itself can be significant in baseball athletes. These injuries account for 5.5%–7% of observed injuries across positions, and were to found to result in an average of 37.7 days missed.8,28 These injuries were most frequently groin strains, with hip inflammation/impingement accounting for a smaller proportion of injuries. There is a 10% chance of reinjury in pitchers, although pitchers with core, hip, or groin injuries demonstrate substantially higher rates of reinjury. 28 FAI results from abnormal engagement of the femoral head with the acetabular rim during hip ROM and has been increasingly recognized as a cause of intra-articular hip pain, particularly in young adults. 8 Coleman et al. 29 found over 47% of intra-articular hip pain among MLB and MiLB players to be FAI, frequently requiring surgery and resulting in an average of 123 days missed. Non-operative management of FAI can be attempted, which involves oral and intra-articular pain management with strengthening of the supporting musculature, but arthroscopic surgery is often warranted to relieve the impingement. Outcomes of hip arthroscopy in baseball players are very positive. Frangiamore et al. 30 reported a 95% return to play rate following arthroscopy in professional baseball players, with no significant decrease in performance or career length, while Klingenstein et al. 31 likewise reported a 97% return to play rate in high school overhead throwing athletes. Recognition of FAI, which requires suspicion of intra-articular pathology confirmed with radiographic imaging, is crucial in allowing baseball athletes to return to sport as promptly as possible.
Thigh
Any athlete engaging in rigorous running and jumping are at risk for injuries to the muscles and tendons of the thigh, and baseball players are no exception. The thigh refers to the quadriceps and hamstring musculature as well as the associated tendons. Overall, hamstring injuries are among the most common in athletics, accounting for nearly a third of professional and collegiate athletic injuries.12,32,33 Salhab et al. 5 identified the thigh as the most commonly injured part of the LE among MLB athletes, accounting for 42% of LE injuries. A substantial majority of these injures were non-operative strains (93.1%, 407/437 thigh injuries). Posner et al. 4 found 8% of MLB injuries to involve the hamstring, with no specification of other thigh muscles. In collegiate baseball, upper leg musculotendinous strains have been observed as the single most common injury during games, accounting for 11% of injuries. 34
Using data collected in the MLB’s Injury Surveillance System, Ahmad et al. 33 found hamstring muscle strains to be the most common time-loss injury in both the MLB and MiLB, accounting for 5.7% and 5.9% of injuries, respectively. A majority of these strains occurred while base running (62% of MLB hamstring injuries and 70.6% of MiLB hamstring injuries), followed by fielding. This is unsurprising given the nature of base running: multiple rapid transitions from standing to full-speed sprinting. The run to first base from batting is unique due to the preceding truncal rotation, urgent acceleration without the ability to lead, and the ability to maximize speed as first base need not be stopped on, with this particular run previously identified in the literature as posing the highest risk for LE muscular sprain.33,35 The average time missed due to hamstring strains was 24 days in the major leagues and 27 days in the minor leagues. Pitching accounted for 4%–6% of hamstring strains. 33 The relatively low prevalence of hamstring strains among pitchers was likewise observed by Howard et al., 36 who found only 78 instances of MLB pitchers being placed on the DL for hamstring injuries across 10 MLB seasons. The relationship between pitching and hamstring injury is important, however, due to the higher likelihood of requiring UCL surgery in pitchers and the potential use of hamstring tendons as autografts for UCL reconstruction. Howard et al. 36 found 67.9% of hamstring injuries in pitchers to occur in the landing leg, with no differences in severity, return to play, or performance related to which leg the sprain occurred in. The influence of UCL autograft harvesting on the impact and rate of hamstring injuries among pitchers is subject to ongoing study, with the most recent evidence suggesting that UCL autograft harvest does not affect subsequent performance or rates of future hamstring injury in professional pitchers. 37
Quadriceps strains also occur in baseball athletes, but there is a relative paucity of literature given their low prevalence. Rapid acceleration requires a forceful eccentric contraction of the powerful quadriceps muscle, which when done from rest such as in base running, can overload the muscle and produce painful partial tears. Ahmad et al. 33 noted that quadriceps strains accounted for 2.9% of MLB injuries, a substantially smaller proportion than hamstring injuries. A study by Kokubu et al. 38 of Japanese professional baseball players observed only six quadriceps sprains among a single team in a near year period, compared to 33 hamstring and 10 calf sprains.
Given the prevalence of thigh muscle strains and the impact these injuries can have on a player’s season, there is continued attention on injury prevention. Eccentric training has been proposed as a useful training modality for injury prevention. 39 In a prospective trial utilizing MLB players, Seagrave et al. 40 found that hamstring training involving use of the Nordic hamstring eccentric exercise resulted in decreased incidence of hamstring sprains, consistent with previous literature regarding soccer and rugby players. There is limited standardization of preventive hamstring training among baseball players, but a conscious focus on eccentric strengthening likely produces positive results, supported by a 2019 meta-analysis finding that Nordic Hamstring use in injury prevention programs halved the rate of hamstring injuries across multiple sports. 41 Ahmad et al. 33 found hamstring strains among MLB athletes were more likely to occur early in the regular season, potentially related to inflexibility or fatigability among athletes, or secondary to colder temperatures during the early April and May months compared to the rest of the summer. An emphasis on offseason training with eccentric exercises and neuromuscular conditioning may be the optimal way to minimize in-season strains of thigh musculature, with strong evidence in particular supporting such training to minimize hamstring injury risk.
Knee
The knee joint and the ligaments which support it are loaded constantly during rigorous athletic activity. The knee is primarily stabilized by four ligaments: two collateral ligaments and two cruciate ligaments, with two menisci distributing force across and diminishing point loading in the joint space; any of these structures can become injured with sudden deceleration, landing, and pivoting. The anterior cruciate ligament (ACL) does not require external contact to tear. ACL tears are one of the most common injuries across sports, with potentially substantial effects on subsequent performance and return to sport. 42 Salhab et al. 5 identified knee injuries as the second most frequent site of MLB player LE injury (23%), resulting in the second most average days on the DL (56.4 days) after hip injuries. Knee injuries account for approximately 6.5%–7% of all MLB injuries, with knee surgeries accounting for 5% of surgeries in players across playing levels.4,43
While baseball is not inherently a contact sport, loose balls, sliding players, and the presence of defensive players at bases create opportunities for contact injuries. Dahm et al. 43 identified that 44% of knee injuries in the MLB and MiLB were completely non-contact, with knee injuries occurring most frequently during base running. Contact with the ground was the observed cause of 18.8% of knee trauma, and knee injuries account for 11.9% of injuries experienced while sliding. 7 Examining the epidemiology of knee injuries in the MLB and MiLB, Dahm et al. 43 found that injuries were most frequently contusions or hematomas (30.5% of observed knee injuries) which only resulted in an average of 6 days missed. In contrast, complete ACL tears were uncommon, accounting for only 2% of knee injuries, but resulted in a mean absence from play of 156.2 days, by far the most of all knee injuries. 12% of reported knee injuries required surgery. 43
Despite the relative infrequency of ACL injuries in baseball, the substantial impact these injuries can have, and the need for surgery in the competitive athlete has drawn attention toward both prevention and management of ACL tears in baseball. Dugas et al. 44 reviewed baseball players who had undergone surgical ACL reconstruction across all levels of competitive play, finding a majority of ACL tears to occur during fielding (68%), or base running (29%), with outfielders at the greatest positional risk. Given the inability of the avascular ACL to heal independently, arthroscopic reconstruction is the gold standard for restoring stability in an athlete. Return to play is high following ACL reconstruction with 94% of baseball players managed by Dugas et al. 44 returning to their preinjury level of play, superior to the return rates seen among American football players.45,46 Fabricant et al. 47 identified a 88% return to play rate among MLB players following ACL reconstruction, although consequent changes in performance were noted; athletes played an average of 21.2% less career games than their teammates, and batting average was significantly affected in players with a rear batting leg (plant leg) ACL reconstruction. It is worth noting that given the relative infrequency of this injury in baseball players, epidemiological studies are limited by small patient populations (Dugas et al.: 44 42 players; Fabricant et al.: 47 26 players). At present, there is a paucity of literature examining the long-term outcomes of ACL injuries in baseball players, although studies examining other athletes have demonstrated increased risk of knee osteoarthritis development in those with prior surgery.48,49
Other knee pathology among baseball players is relatively understudied. Conditions such as patellar tendinopathy, medial collateral ligament (MCL) sprains, and meniscal tears can occur in any high-level athlete, and the mechanics of the baseball do not inherently increase the risk of these particular injuries more than would be expected. Given the comparatively lower volume of sprinting and reduced incidence of contact in baseball, the sport presents less risk of these injuries than sports such as soccer or American football.50,51 Dahm et al. 43 found patellar tendinopathy to account for 10.2% of MLB and MiLB knee injuries, with MCL sprains and medical meniscal tears representing 5.5% and 4.4% of knee injuries, respectively. Unspecified knee injuries account for 15.5% of those observed, suggesting room for improvement in further epidemiological studies. Quadriceps tendon tears are particularly uncommon, especially in the young, athletic population. An isolated case report notes a high school baseball player who experienced a quadriceps tendon rupture from a rapid deceleration while fielding, managed operatively with a full recovery, with this singular case report highlighting the rarity of such an injury. 52 This also may occur in a fielder who collides with another player, or wall trying to make a catch, once again resulting in a rapid deceleration and eccentric contraction of the extensor mechanism.
Lower leg/ankle
Injuries to the lower leg, ankle, and foot of baseball players account for approximately 14%–17% of player injuries, with these sites representing 8%, 11%, and 10% of LE injuries, respectively.4,5,53 As with the knee, the ankle and foot are placed under constant varying stresses during athletics, contributing to the risk of acute injury or development of chronic symptoms. Sliding creates an additional opportunity for lower leg injury, with ankle injuries identified as the second most common site of injury when sliding (13.7% of slide injuries) and the most common site during feet-first slides (23.8%). 7 Similar to the knee, contusions are the most commonly reported lower leg injury. 54
The muscles of the calf, in particular the gastrocnemius and soleus, contribute predominantly to plantarflexion of the ankle through their insertion into the calcaneus via the Achilles tendon. 55 Rapid acceleration, which regularly occurs during the initiation of base running, can result in partial tearing of the gastrocnemius muscle as it forcibly plantarflexes the ankle to begin movement. Hultman et al. 35 identified 402 gastrocnemius injuries in the MLB and MiLB between 2011 and 2016, with injuries occurring most frequently during base running (36.1%) and fielding (23.6%). While these injuries only resulted in a mean absence of 12.7 days for MLB players, gastrocnemius injuries are notorious for lingering, with persistent pain or discomfort even as the player returns to participating. 53 As with other musculotendinous injuries, prompt recognition and management of gastrocnemius strains can help reduced the impact of the injury. Rest, ice, and compression followed by a progression of dynamic stretching and controlled strengthening with gradual return to play are recognized as the standard management pathway. 56
Ankle injuries represent approximately 11% of LE injuries. Low ankle sprains are the most common and result in a mean number of missed days ranging from 9 to 54.4.5,54 The ligaments of the ankle can be easily sprained with rotation or prono/supination of the foot, as can happen during running, jumping, or sliding. A review of MLB and MiLB ankle injuries by Lucasti et al. 54 found ligamentous injury to be the most common lower leg injury type, resulting in a mean of 11 days missed, and subsequent surgery occurring in 16% of injuries. These injuries were most likely to occur while base running, and outfielders saw the highest rate of injuries among player positions (15%). These findings are consistent with those observed regarding the knee, and it is not surprising that injuries to joints of the LE occur most commonly with high-energy running and among players responsible for the most in-game movement. Injuries identified as specific to the anterior talofibular ligament were the most common ligamentous injury (41% of ligamentous injuries) and resulted in an average of 10 days missed. Accounting for only 8.5% of lower leg injuries by position, catchers were the most likely position to undergo surgery for a lower leg injury (5% of injuries in the MLB and 3% in the MiLB). 54 Catchers are at increased risk for collision injuries given their position over home plate, with 30% of collision-related injuries in catchers involving the ankle. 57 Despite a relatively low number of mean days missed following an ankle injury, acute injuries can still prove season-ending if severe, and athletes who experience severe or repeat ligamentous injuries are at increased risk for the development of chronic ankle instability. 58
At present, there are minimal studies investigating the prevention of lower leg injuries in baseball. As with hamstring injuries, eccentric strengthening exercises targeting ankle stabilizers may play a role in athletic training and preventive management. 54 Given the association between ankle injuries and running, there may be value to minimizing overexertion through reduced training days or an appropriate balance between stretching, strengthening, and running. 59 Proprioceptive training, which places emphasis on balance and sensorimotor adaptation, has been found to be effective in both prevention and rehabilitation of ankle injuries. 60 While there exists a role for prophylactic bracing or taping, particularly in players with previous ankle injuries, there is insufficient evidence suggesting the value of prophylactically bracing a healthy ankle.61,62
Conclusion
Baseball is unique in its multiple facets: pitching, hitting, base rounding, and fielding are distinct activities that require different athletic skills to perform at a high level. Likewise, these different aspects of the game can contribute to a multitude of varying injuries. While high-velocity overhead throwing, along with batting, can produce a plethora of upper extremity injuries that often garner attention, injuries to the LE can severely impact a player’s performance and ability to compete. The rigors of the short, explosive sprinting required for base running, as well as the dynamic movement required for fielding, create ample opportunity for lower limb injury, and even subtle pathology can affect a pitcher’s ability to perform or increase their long-term risk of injury.
The present review is limited by the availability of research available on LE injuries in baseball athletes, a field which remains constantly evolving as new literature emerges although understudied relative to upper body injuries. Although referenced studies were chosen for quality and applicability, this study is not a meta-analysis, and there exists substantial variability in the methods and investigative techniques of the cited studies.
Management of athletic injuries such as those in baseball players requires a multidisciplinary effort from physicians, trainers, staff, coaches, and players. The present review provides a comprehensive overview of common LE injuries in these athletes with the purpose of providing information accessible to all members of the interdisciplinary care team. Recognition of the epidemiology and sequelae of these injuries is important as research into prevention and management of LE injuries continues to evolve.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.