
Abstract
Pancreatic duct dilatation occurs in conditions including chronic pancreatitis, pancreatic carcinoma and intraductal papillary mucinous neoplasms. Although several pancreatic benign and malignant tumours have been reported in association with type 1 neurofibromatosis, an association with gross pancreatic duct dilatation or ectasia has not been previously published. We report on a patient with type 1 neurofibromatosis found to have idiopathic gross pancreatic duct dilatation and exocrine insufficiency. A 51-year-old female with type 1 neurofibromatosis presented with weight loss and steatorrhoea. Computed tomography and magnetic resonance cholangiopancreatography showed a possible cystic lesion in the head of the pancreas, a grossly dilated main pancreatic duct and minimal thinned out pancreatic parenchyma. Endosonography confirmed diffuse dilatation of the pancreatic duct with no evidence of a separate cystic neoplasm. Endosonography-guided aspiration revealed non-mucinous, clear fluid with high amylase and normal carcinoembryonic antigen levels. The patient was prescribed pancreatic enzyme supplementation and showed symptomatic improvement. Associations between type 1 neurofibromatosis and pancreatic duct ectasia or chronic pancreatitis have not been reported, and this finding may be coincidental. Clinical presentation in conjunction with multimodal imaging and biochemical and cytological fluid analysis did not reveal the aetiology of the ectatic duct system and attenuated glandular tissue in this patient which is most likely congenital.
Keywords
Introduction
Chronic pancreatitis is the commonest cause of main pancreatic duct (PD) dilatation. 1 Pancreatic carcinoma and intraductal papillary mucinous neoplasms (IPMN) are other important causes, while a proportion have no discernible aetiology. 1
Type 1 neurofibromatosis (NF1) or von Recklinghausen’s disease is an autosomal dominant, multisystem genetic disorder characterized by cutaneous manifestations, most notably café-au-lait spots and axillary freckling; by skeletal dysplasias; and by the growth of both benign and malignant nervous system tumours, most notably benign neurofibromata. 2 Several pancreatic benign and malignant tumours have been reported in association with NF1. These include pancreatic neuroendocrine tumours (PNETs) such as insulinomas, somatostatinomas and neuroendocrine carcinomas.3–7 Mutations in the NF-1 gene and resultant dysfunction of neurofibromin may be involved in the pathogenesis of PNETs, 7 although this requires further study. Gastrointestinal stromal tumours (GIST) are also frequently reported in patients with NF1. 8 However, an association with gross PD dilatation or ectasia has not been previously published. We report on a patient with NF1 with idiopathic gross main PD dilatation and exocrine insufficiency.
Case presentation
A 51-year-old female with NF1 presented with steatorrhoea and weight loss of 6 years. She had dyspeptic symptoms but had been otherwise well. She did not have diabetes mellitus. There was no history of acute pancreatitis, alcohol use, gallstone disease or abdominal surgery. She had a family history of NF1. She was thin and had multiple neurofibromata and café-au-lait patches. Her abdominal examination was unremarkable. Her complete blood count, blood sugar, liver and renal biochemistry, and amylase were normal.
A pancreatic protocol contrast computed tomography (CT) of the abdomen showed a cystic lesion in the head of the pancreas (Figure 1). No calcification, septae or solid lesions were noted within the cyst or in the wall. Gross dilatation of the PD was seen at the neck (2.38 cm), body (2.1 cm) and tail (1.2 cm) of the pancreas. Communication between the cyst and the ectatic PD was not demonstrable. An attenuated rim of pancreatic parenchyma was identified. The bile ducts were of normal calibre.
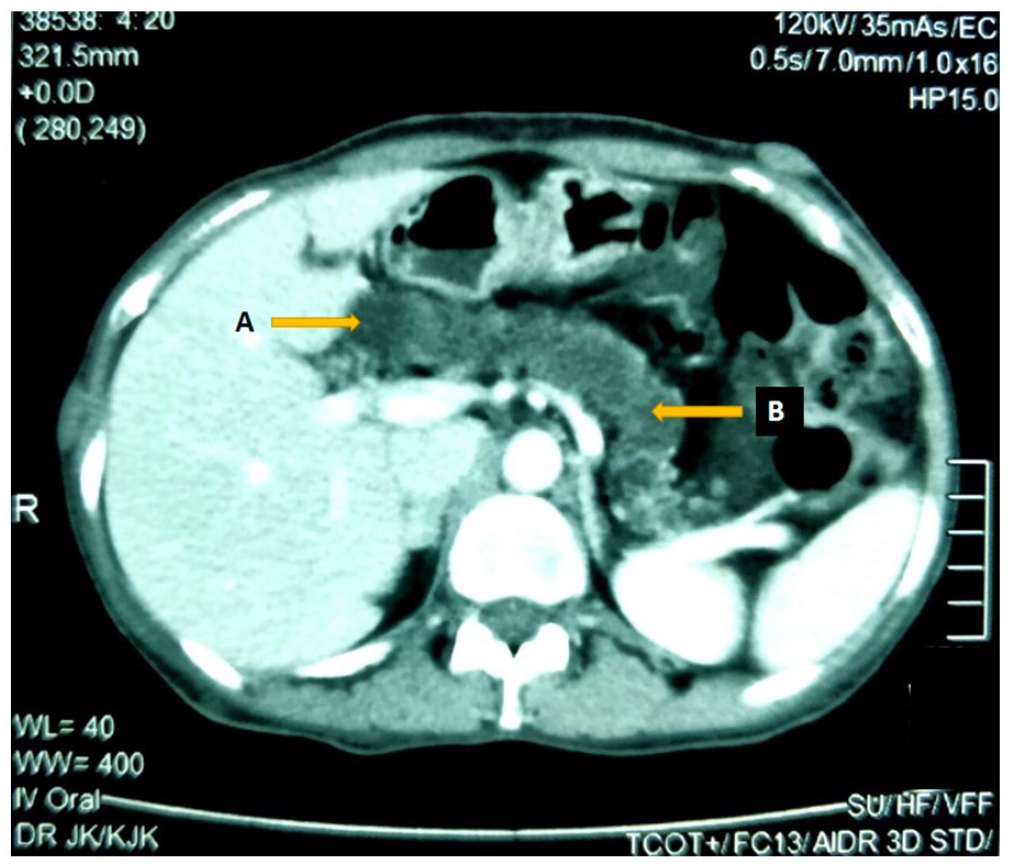
CECT of the abdomen showing a cystic lesion in the region of the head of the pancreas (arrow A) with gross pancreatic duct dilatation (arrow B). Pancreatic duct measured 2.38 cm in the neck, 2.1 cm in the body and 1.2 cm in the tail.
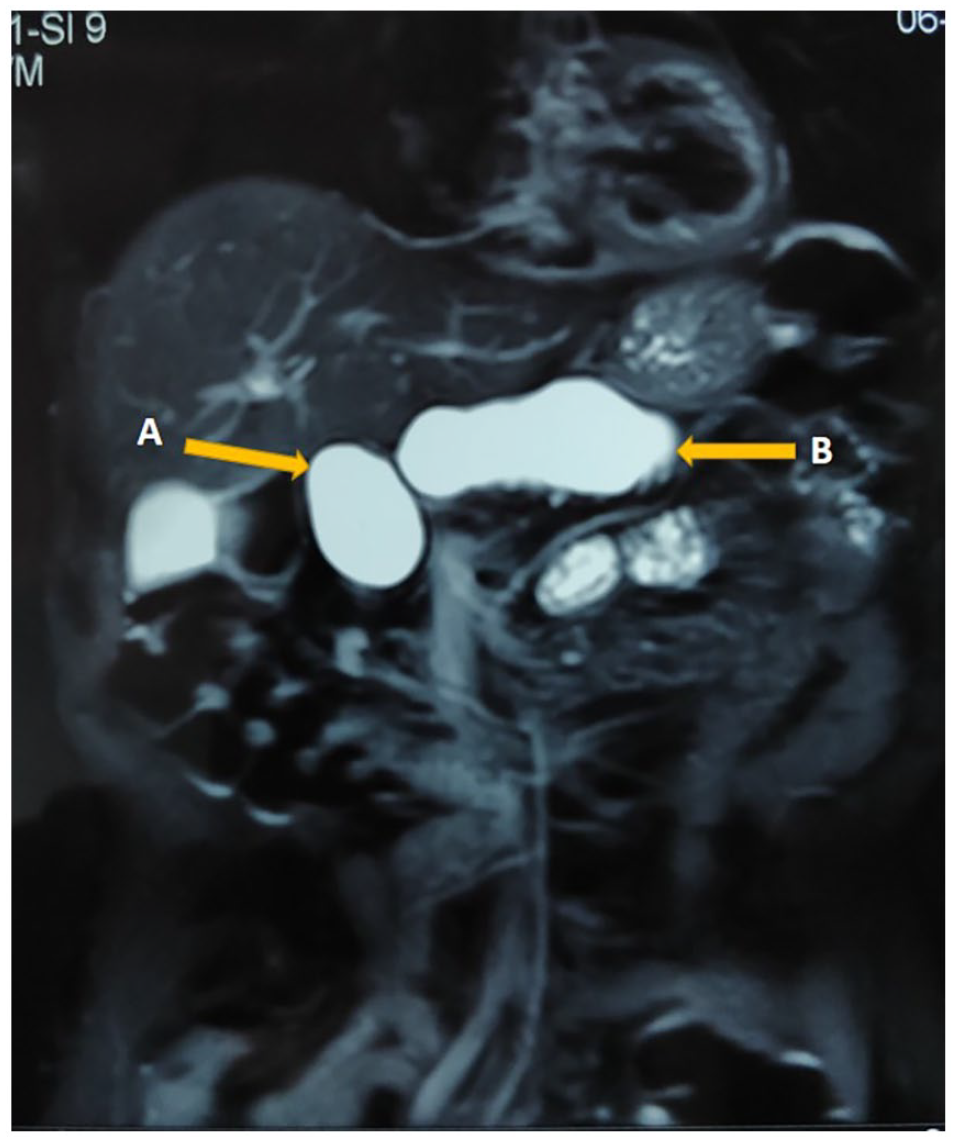
Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) also confirmed a well-defined cystic lesion with no solid component in the uncinate process and the head of the pancreas measuring 5 × 3 cm with gross tortuous dilatation of the PD (2.2 cm) (Figures 2–4). The pancreatic parenchyma appeared atrophic. The extra and intrahepatic bile ducts were normal.

MRCP showing a well-defined cystic mass lesion in the uncinated process and the head of the pancreas (arrow A) with a gross tortuous dilatation of the pancreatic duct (arrow B). Common bile duct was normal in calibre with smooth outline and the intrahepatic ducts were also normal in calibre.
Coronal section of MRI showing a well-defined cystic mass lesion in the uncinated process and the head of the pancreas (arrow A) causing gross tortuous dilatation of the pancreatic duct (arrow B).

Cross-sectional view of the MRI showing a well-defined cystic mass lesion in the uncinated process and the head of the pancreas (arrow A) causing gross tortuous dilatation of the pancreatic duct (arrow B).
Endosonography (EUS) showed a grossly dilated PD (>2.0 cm) along its entire length from the neck to the tail (Figure 5). The cystic dilatation of the head was in continuity with the main PD, with the parenchyma mainly seen at the tail of the pancreas. The ampulla of Vater was normal on side-viewing endoscopy. The aspirate from the PD was non-viscous, clear and colourless. Cytology of the aspirate showed no pus cells, lymphocytes or red cells. Fluid amylase was 1778 U/L and carcinoembryonic antigen (CEA) was 6.1 µg/L. These findings were consistent with normal pancreatic exocrine enzymes with no evidence suggestive of other cystic neoplasms such as IPMN.

Endoscopic ultrasound image showing a grossly dilated pancreatic duct (20 mm in diameter) throughout its entire length (from head to tail). No separate cystic lesion in the head of the pancreas was identified.
She was started on pancreatic enzyme supplementation. and followed up for 4 years. Though her persistent dyspepsia persisted, the symptoms of exocrine deficiency improved with enzyme supplementation.
Discussion
A spectrum of inflammatory and neoplastic conditions of the gastrointestinal tract and hepatobiliary system have been associated with NF1. 9 However, to our knowledge, the association between NF1 and idiopathic gross main pancreatic duct dilatation has not been previously reported.
PD dilatation mostly occurs in association with chronic pancreatitis, pancreatic carcinoma and IPMN, 1 although in some cases the cause is unknown. 1 The PD dilatation demonstrated in this patient with NF1 was unique for several reasons. The duct dilatation was diffuse, extending from the head to the tail of the pancreas, and massive, with a diameter of more than 2 cm in its entire length. Furthermore, no demonstrable cause of proximal PD obstruction such as a calculus, stricture or neoplasm was observed. The possibility of a neurofibromatosis-related soft tissue lesion such as a ganglioneuroma, neurofibroma or schwannoma of the pancreas causing duct dilatation was considered but excluded using multimodal imaging. The considerably thinned out pancreatic parenchyma was likely responsible for exocrine dysfunction although the presence of some parenchyma in the tail probably resulted in preservation of endocrine function.
Although the CT and MRCP were suggestive of a discrete cyst in the head of the pancreas, EUS clarified that it was indeed part of the ectatic duct. The absence of a separate discrete cyst and the analysis of the aspirate excluded the likelihood of a cystic neoplasm of the pancreas. In addition, the non-viscous, clear aspirate from the duct with low CEA levels and normal cytology were not in favour of cystic neoplasms such as mucinous cystadenomas (MCA) or IPMN. This highlights the value of EUS as a diagnostic tool when used in conjunction with cross-sectional imaging in the assessment of pancreatic lesions. 10
More importantly, the patient’s history dates back to 10 years (including follow-up), making malignancy highly unlikely. Specific tumour markers were not examined because of the absence of clinico-radiological findings in favour of a pancreatic adenocarcinoma and the necessity to be selective in sourcing costly assays in our resource-limited circumstances. Furthermore, except for exocrine failure, clinical and radiological manifestations on cross-sectional imaging were unlike that observed in chronic pancreatitis as the PD dilatation was gross and there was no calcification. With the background of NF1, congenital duct ectasia of unknown aetiology was our hypothesis and led us to report this case.
Conclusion
The association of NF1 with idiopathic gross pancreatic duct dilatation has not been previously reported. Clinical presentation in conjunction with multimodal imaging and biochemical and cytological fluid analysis did not reveal the aetiology of the ectatic duct system and attenuated glandular tissue in this patient, which is most likely congenital.
Footnotes
Acknowledgements
The authors wish to thank Mr Pragatheeshkumar Sriskantharajah for editing the images.
Author contributions
UJ, OB and PKW contributed to collection of information and writing of the manuscript. NF and SS contributed to writing and final approval of the manuscript. All authors have read and approved the final manuscript.
Availability of data and material
All data used to support the findings of this study are included within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval and consent to participate
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for anonymised information and accompanying images to be published in this article.