
Abstract
Neurofibromatosis type 1 is an autosomal dominant disorder with cutaneous features and multiple tumors that involve different organs. Gastrointestinal stromal tumors are non-epithelial tumors associated with neurofibromatosis type 1 and arise from the gastrointestinal tract. Patients with gastrointestinal stromal tumor present most commonly with anemia due to overt or occult bleeding and in rare cases diagnosis might be delayed so patients present with gastrointestinal tract obstruction. Here, we report a rare case of an older patient with neurofibromatosis type 1, who was undiagnosed and presented with acute abdomen due to gastric outlet obstruction. It was caused by progressive gastrointestinal stromal tumor in the antrum of the stomach. Gastrointestinal stromal tumors should be considered in the differential diagnosis of gastric outlet obstruction, especially in patients with neurofibromatosis type 1.
Introduction
Neurofibromatosis type 1 (NF-1), also known as Von Recklinghausen’s disease, is an autosomal dominant syndrome caused by mutations in NF-1 tumor suppressor gene, which predispose to benign and malignant tumors. 1 The most characteristic features are cutaneous manifestations, which include Café-au-lait macules (96.5%), axillary and inguinal freckling (90%), and neurofibromas. 2 Many tumors are associated with NF-1, such as pilocytic astrocytoma, gastrointestinal stromal tumors (GISTs), pheochromocytoma, and juvenile myelomonocytic leukemia. GISTs might be developed in up to 25% of patients with NF-1, they mainly arise from small intestine (70%) than stomach, and the most common sign is anemia due to overt or occult bleeding.3,4 According to many published cases, gastrointestinal bleeding was the most common symptom and rarely due to obstruction of the gastric outlet. Here, we report an unusual case of an adult man, who was diagnosed with NF-1 following gastric obstruction.
Case report
A 65-year-old man presented to our clinic with acute onset of non-bilious and non-bloody vomiting. The patient also came with weight loss, anorexia, and postprandial epigastric pain which developed gradually from 6 months. He smokes 45 packs a year. He has no significant medical or surgical history. The vital signs were normal. The physical examination showed a moderate epigastric tenderness. Laboratory evaluation revealed a moderate anemia with hemoglobin of 10.5 g/dL and MCV 76 fL; the other tests were normal. Ultrasonography showed a large residue in the stomach with thickness in stomach wall. Gastroduodenoscopy was performed, and the findings are shown in Figure 1. It inaccurately interpreted as a stricture in the antrum, which caused gastric outlet obstruction. Abdominal computed tomography (CT) was initially negative, with no significant changes in the abdominal viscera (Figure 2). The macroscopic examination of a mucosal biopsy showed inflammatory changes. The clinical features and radiological and histopathological findings were most consistent with ulcer stricture. A balloon dilatation was performed. After the procedure, the patient was in a stable condition and the symptoms were resolved. However, as soon as the patient was fed, the complaint relapsed. The patient underwent a barium swallow study to evaluate the results of the previous dilation; the barium swallow showed an obstruction in the duodenum (Figure 3). A detailed physical re-examination was performed and we noticed multiple café-au-lait spots distributed on his trunk and multiple cutaneous neurofibromas over the face and neck (Figure 4(a) and (b)). These cutaneous manifestations are consistent with NF-1 based on the National Institutes of Health (NIH) criteria, 5 which include the presence of two or more of the signs, and according to these criteria, our diagnosis of NF-1 was confirmed.
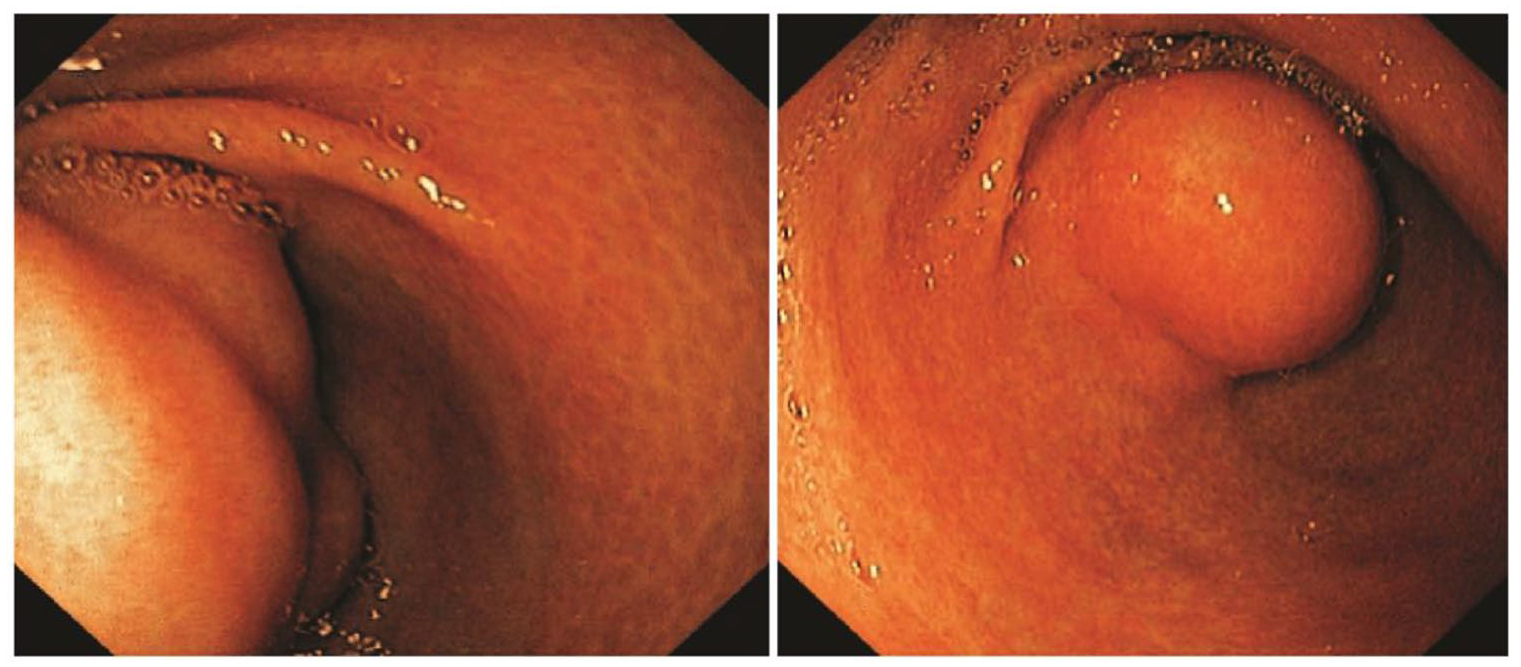
Esophagogastroduodenoscopy (EGD) showed narrowing in the outlet of the stomach.
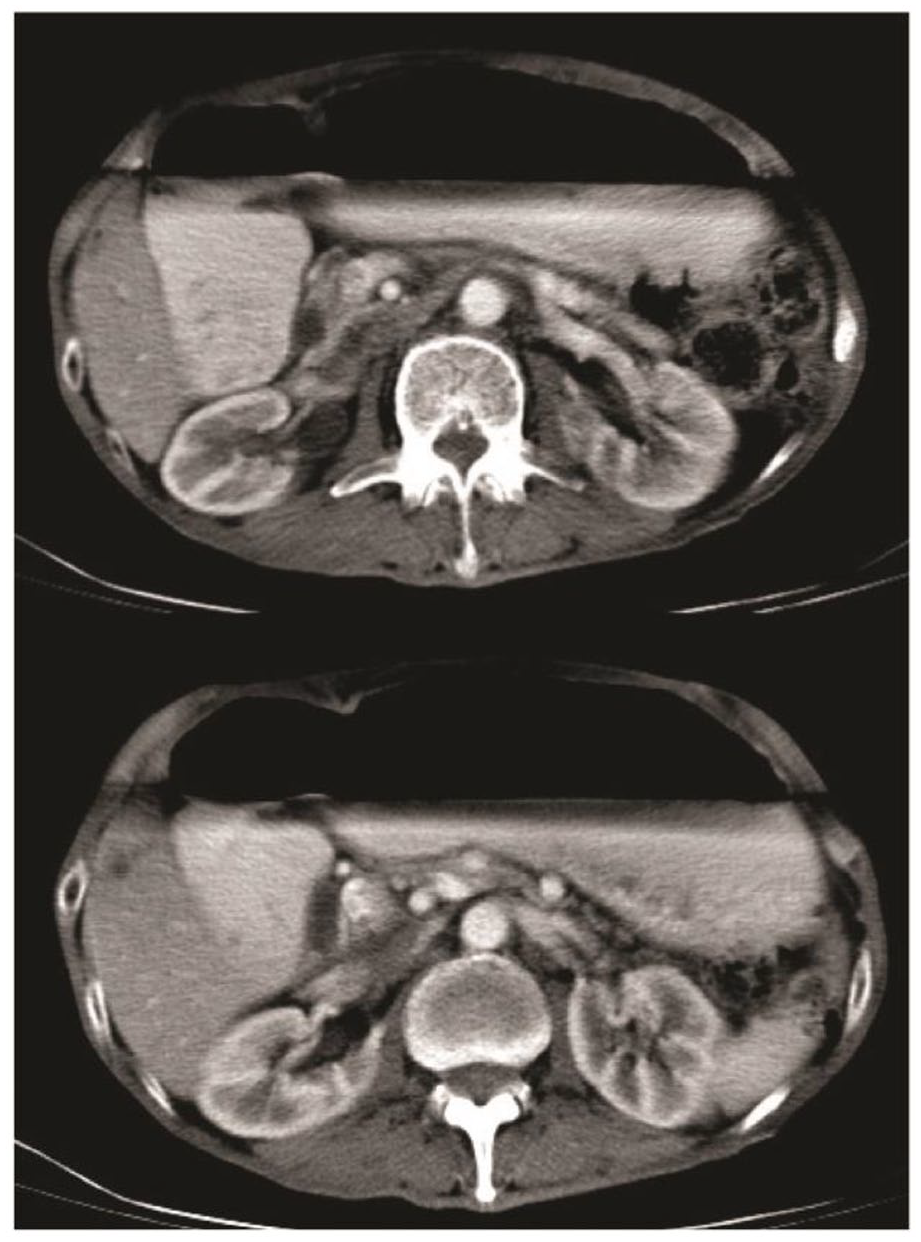
Axial section abdominal CT shows gastric dilatation with residue.
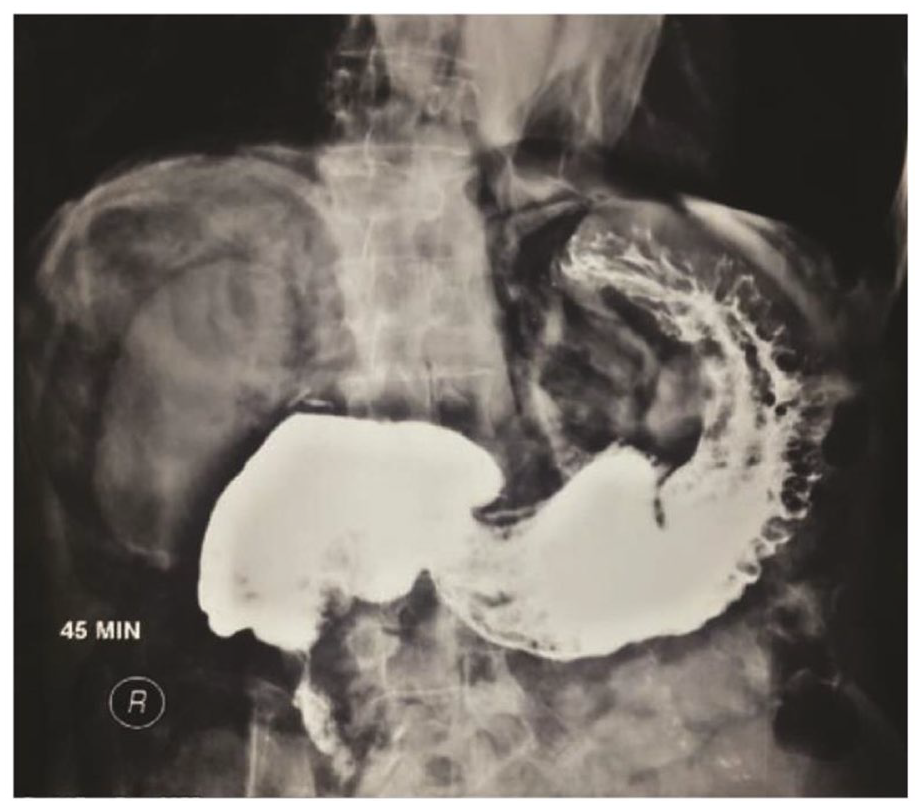
The barium swallow study at the 45th min shows slow movement of barium from the stomach through the pylorus to the duodenum.
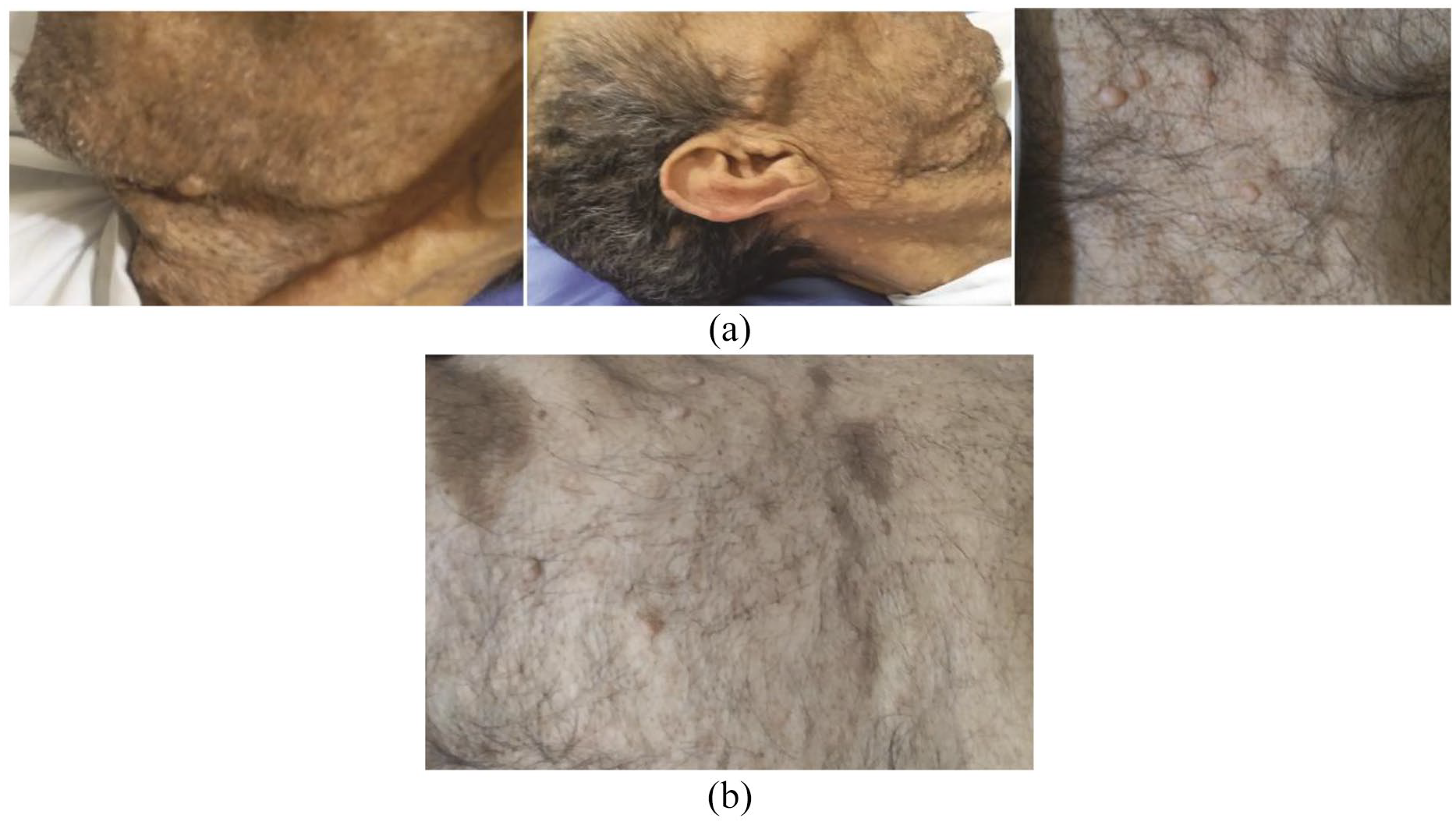
(a) Photographs of the patient showing cutaneous and subcutaneous neurofibromas. (b) Multiple Café-au-lait macules. Characteristic features include even pigmentation and smooth, well-defined borders.
Because of the strong association between NF-1 and GISTs, the possibility of GISTs incidence was considered, so the patient underwent an exploratory laparotomy, which detected multiple tumors arising from the stomach and small intestine. It was resected and sent for pathological study that showed spindle-shaped tumor cells arranged in fascicles and bundles occupying the submucosa and muscularis propria, which suggested a spindle cell neoplasm, most likely GISTs (Figure 5). Confirmation of the diagnosis of GISTs requires an immunohistochemical test, but this test has not been available to the patient due to its high cost and few laboratories to perform. Therefore, physicians replaced it with pathological evidence compatible with clinical information to make the final diagnosis.
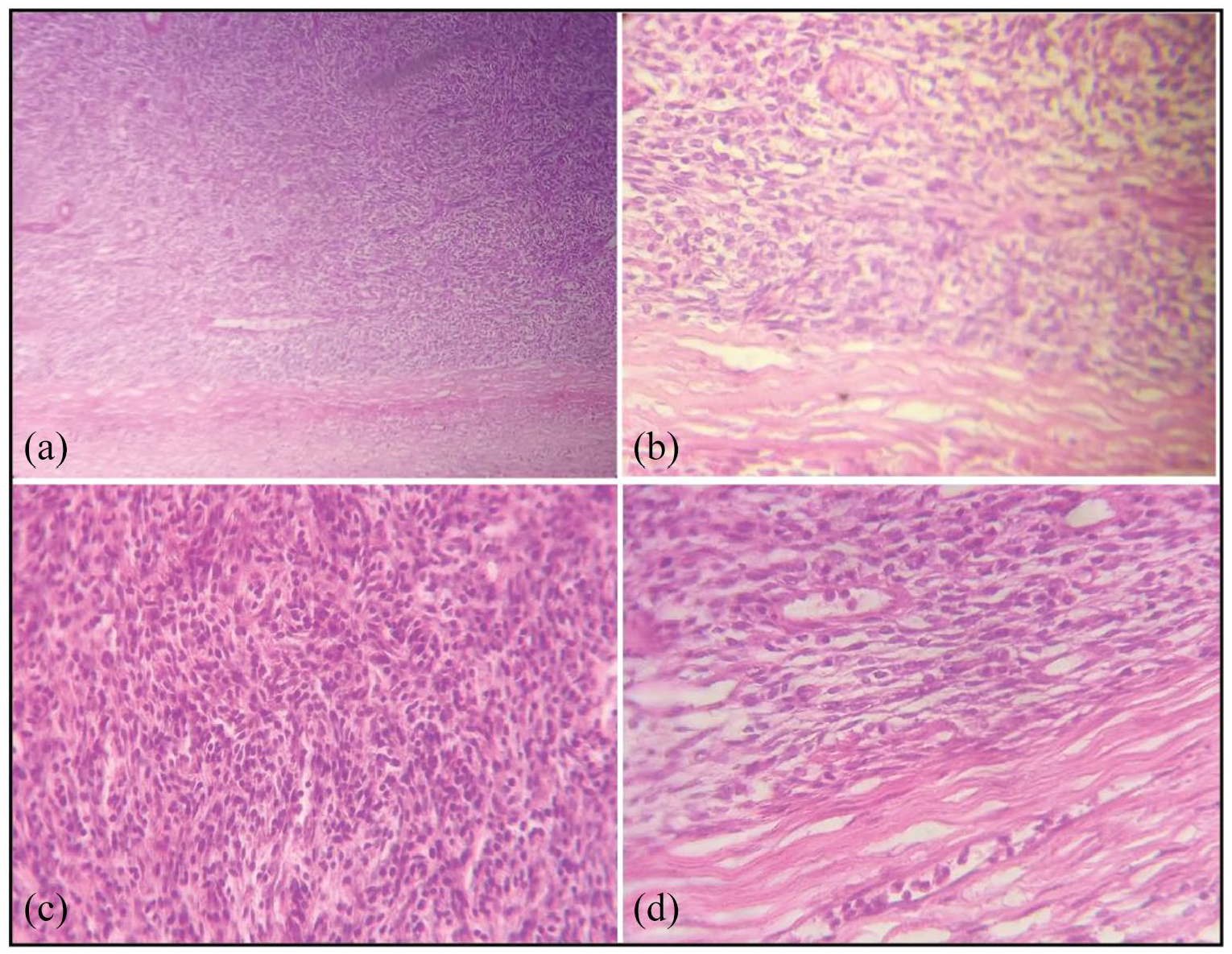
Spindle-shaped tumor cells arranged in fascicles and bundles occupying the submucosa and muscular layer: (a) H&E, ×40 magnification; (b) H&E, ×200 magnification; (c) H&E, ×200 magnification; and (d) H&E, ×200 magnification.
Discussion
This case demonstrates an unusual situation of a patient with NF-1. NF-1 is a common disorder associated with high risk of benign and malignant tumors occurrence; it was first described in the 13th century. In the 19th century, von Recklinghausen described “neurofibromas” and the other features of NF-1. Therefore, NF-1 was called von Recklinghausen’s disease till the end of the 19th century.1,2 The diagnosis of NF-1 is based on the presence of the characteristic clinical features. It has been described by the NIH. 5
The clinical manifestations of NF-1 develop over time; approximately 50% of sporadic NF-1 patients (i.e. de novo mutations) have clinical criteria for diagnosis in the first year of life and nearly are obvious by 8 years of age. 5 GISTs are rare mesenchymal neoplasms of the gastrointestinal tract. They arise from the stomach and small intestine wall as subepithelial neoplasms. 4 The association between GISTs and NF-1 is well described and it is not uncommon. GISTs arise from stomach most commonly, but in the presence of NF-1, the most common site is small intestine.3,4,6 The progress of GISTs is slow and the symptoms depend on tumor site; most patients with GISTs are asymptomatic. Overt or occult GI bleeding is the most common symptom of the gastric GIST; however, some tumors may grow large enough, causing an acute abdomen in very rare cases.4,6 By reporting the second case in published literature, we want to alert physicians to consider NF-1 as a differential diagnosis for patients with gastric obstruction.
Conclusion
The possible incidence of NF-1 in patients with GIST should be considered more and vice versa. In atypical cases, careful clinical examination may provide much more valuable information than radiographic methods and should not be underestimated even if the diagnosis is clear.
Footnotes
Acknowledgements
We sincerely thank Dr Simon Yousef, Department of Pathology, Hama National Hospital, Hama, Syria, for his great help.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval.
Informed consent
Oral consent was taken from the patient, but after the patient died, his son was the legally authorized to give the written informed consent, so it was obtained from the patient’s son for all information including images and the other medical details to be published in our article.