
Abstract
Objectives:
Primary retroperitoneal mature cystic teratomas are exceedingly uncommon in males aged 50 years and above, and only seven cases have been reported in the literature so far. They usually occur in infants less than 6 months and young females. The aim of this article is to present a rare case of a 51-year-old male with a primary retroperitoneal mature cystic teratoma located in the right infrarenal area adherent to the psoas muscle and to discuss a historical literature review.
Methods:
An incidental hypoechoic, solid appearing 8.2 × 7.6 × 7.8 cm3 mass arising off the inferior pole of the right kidney was found on abdominal ultrasound during evaluation for a history of alcoholism. Computerized tomography (CT) scan revealed small calcifications in the lower part of the cystic mass. Laparotomy with excision of the retroperitoneal mass was performed.
Results:
On gross examination, the specimen consisted of a cyst filled with pale yellow greasy material with entrapped hair. Histopathologic examination revealed a dermoid cyst with focal chronic inflammation, dystrophic calcification, and foreign-body giant cell reaction.
Conclusions:
Retroperitoneal mature cystic teratoma in an older male is extremely rare. Primary gonadal teratoma with retroperitoneal metastasis should be excluded first. Evaluation of age and location of tumor are critical for its prognosis. Complete excision of tumor is necessary to evaluate whether there are immature and solid elements which need long-term follow up due to the increased risk of malignancy.
Introduction
Mature cystic teratomas, also known as dermoid cysts, are neoplasms composed of tissues from at least two of the three germ layers.1,2 They are most commonly located in the gonads and infrequently in extragonadal sites such as the retroperitoneum in less than 4% of the cases. 3 Metastasis of gonadal malignancies to the retroperitoneum comprise most of the retroperitoneal neoplasms; however, primary retroperitoneal neoplasms comprise only 0.1%–0.3% of all the tumors and 1%–11% of those are teratomas.4–6 In children, the most common retroperitoneal tumors are neuroblastoma and Wilms’ tumor. 7 Primary retroperitoneal teratomas (RT) are characterized by absence of attachment to other organs such as kidneys, adrenal glands, and pancreas. 8 Cases are reported usually early in infancy or in young females. The most common site is sacrococcygeal area in infants and left suprarenal region in adults.9–14 The aim of this article is to present a rare case of a large retroperitoneal mature cystic teratoma located on the right infrarenal region in a 51-year-old male and to present a historical literature review.
Case study
A 51-year-old Caucasian male was found to have an incidental hypoechoic, solid appearing 8.2 × 7.6 × 7.8 cm 3 mass arising off the inferior pole of the right kidney on abdominal ultrasound during evaluation for a history of alcoholism (Figure 1). The review of systems was unremarkable. The patient had a past medical history of alcoholism, diabetes mellitus type 2, hypertension, and gastroesophageal reflux disease. The medication list included hydrochlorothiazide, glargine, ranitidine, sitagliptin, and metformin. The patient had no known allergies. Past surgical history included repair of a torn left rotator cuff. The social history was significant for cigarette smoking. He had quit drinking alcohol 6 years ago. Abdominal exam revealed 10 cm × 10 cm palpable mass occupying the right lower quadrant. It was non-tender, firm with smooth surface, and a well-defined margin. The mass was fixed and did not move with respiration. The rest of the physical examination was unremarkable. The scrotum was well developed with bilateral unremarkable testis. The blood tests were all unremarkable except for elevated liver function tests.

Sagittal image of abdominal ultrasound showing right infrarenal hypoechoic mass.
A computerized tomography (CT) scan of the abdomen and pelvis with contrast revealed a large cystic mass lying inferior to the lower part of the right kidney measuring about 8.6 × 8.3 cm2 in diameter (Figures 2 and 3). The mass did not appear to arise from the right kidney. The mass was adherent to the right iliopsoas muscle. No abnormal enhancement was identified. Small calcifications were seen in the lower part of the cystic mass. There was no retroperitoneal lymphadenopathy, ascites, or intestinal mechanical obstruction. Fatty infiltration of the liver was also seen. A CT-guided aspiration and biopsy of the cystic mass were then attempted; however, the specimen collected was unsatisfactory (Figure 4).

Axial image of contrast enhanced computed tomography of abdomen and pelvis showing a large cystic mass inferior to the right kidney with small calcifications.

Coronal image of contrast enhanced computed tomography of abdomen and pelvis showing the cystic mass adherent to the psoas muscle.

CT-guided biopsy of the mass.
Laparotomy with excision of the retroperitoneal mass was performed. On gross examination, the specimen consisted of a cyst measuring 13.5 × 5.5 cm2. The cyst wall was up to 0.3 cm thick. The cyst was filled with pale yellow greasy material with entrapped hair (Figure 5).

(a) Specimen received in formalin with pale yellow greasy material floating; (b) cyst wall containing the sebaceous material; (c) aggregates of the sebaceous material; and (d) few strands of entrapped hair from the cyst contents.
Histopathologic examination revealed a dermoid cyst with focal chronic inflammation, dystrophic calcification, and foreign-body giant cell reaction. The cyst wall was focally lined by keratinizing stratified squamous epithelium with partial disruption and dystrophic calcification. The cyst wall comprised dense fibrous tissue abutting striated muscle. The cyst contents comprised acellular keratinous material along with fragments of hair shafts (Figures 6–8). No other lines of differentiation or immature/undifferentiated elements were present. Written informed consent was obtained from the patient for publication. Our institution does not require ethical approval for reporting individual cases.
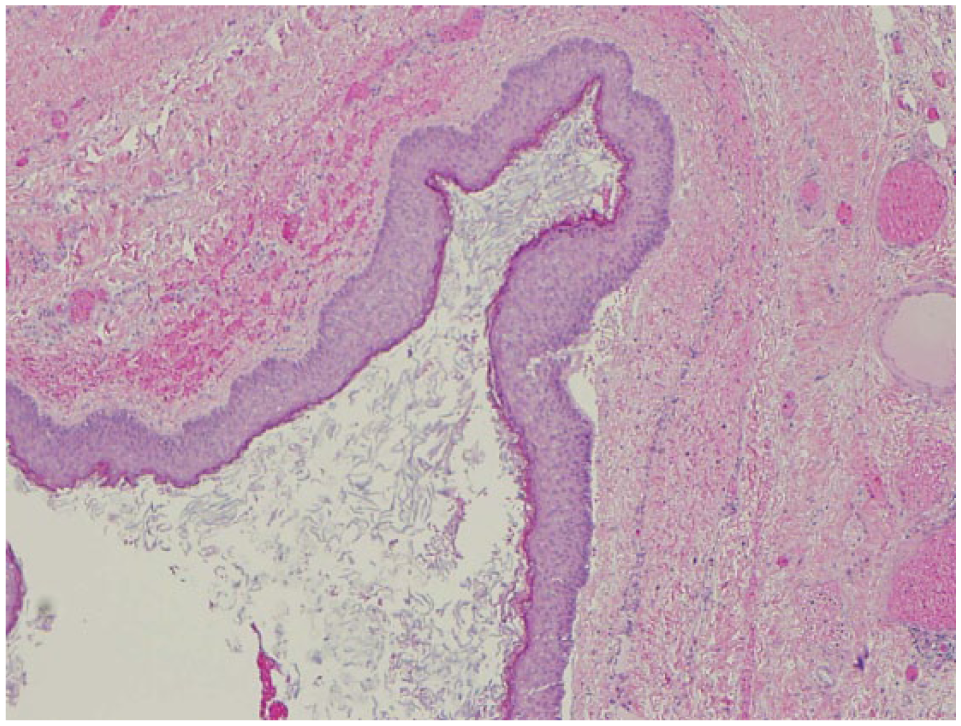
Cyst wall lined by stratified squamous epithelium.
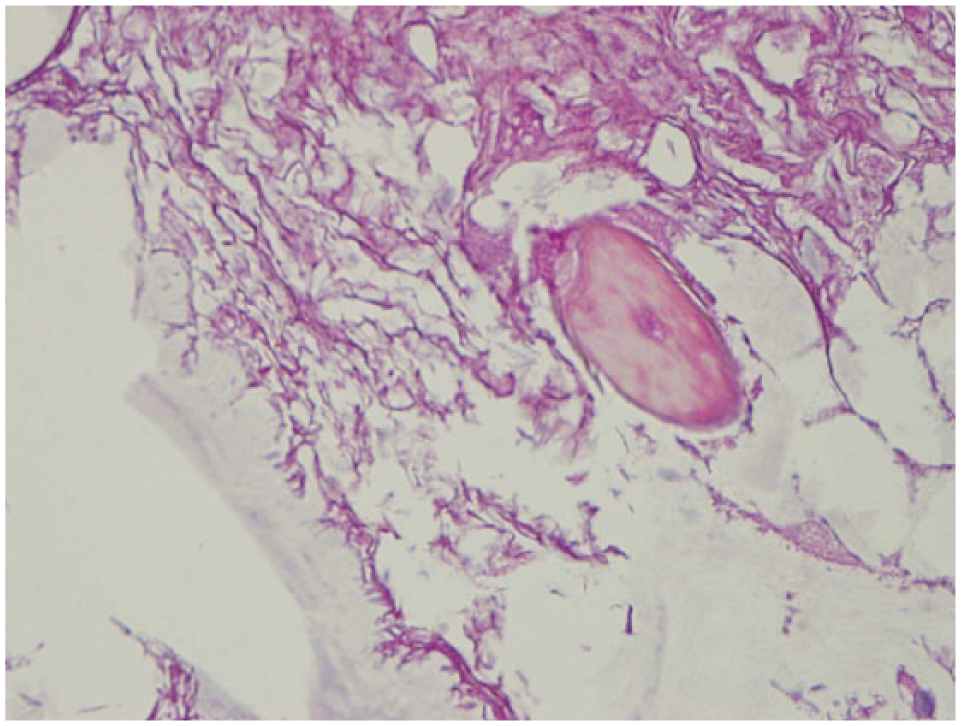
Cyst contents showing acellular keratinous material and a hair shaft.

Fibrous cyst wall with focal calcification.
Discussion
RT were first described by Morgagni 15 in 1769. In 1937, urography was first used to diagnose RT.16,17 In 1968, 127 cases of RT from around the world were recorded by Arnheim, 7 Palumbo et al., 6 and Engel et al. 14
The oldest person with RT recorded was an 82-year-old female who presented with change in bowel habits, left abdominal pain, and weight loss for 2 months. 18 In earlier times, before the widespread use of imaging modalities, the patients usually presented with abdominal enlargement or pain due to huge size of the mass with or without obstructive symptoms. 19 In 1987, the first CT scan appearance of RT was presented, and with the advent of magnetic resonance imaging (MRI), many more cases are now discovered incidentally.20,21 This has led to further characterization of the RT through imaging modalities.2,4,10,21
The differential diagnosis of a primary retroperitoneal mass could be divided between solid and cystic. Cystic retroperitoneal masses can be either neoplastic or non-neoplastic. Mature teratomas, mucinous cystadenomas, and cystic mesotheliomas encompass the neoplastic cystic masses, while lymphangiomas, müllerian cysts, epidermoid cysts, pancreatic pseudocysts, lymphoceles, urinomas, and hematomas comprise the non-neoplastic cystic masses.22,23 Beside teratomas, fat-containing primary retroperitoneal masses include lipoma, well-differentiated liposarcoma, and dedifferentiated liposarcoma.22,24–26 However, primary retroperitoneal masses with calcification include malignant fibrous histiocytoma, dedifferentiated liposarcoma, paraganglioma, and ganglioneuroma.27–29 Immature teratomas usually present as solid masses containing undifferentiated tissues but may also include fat and calcification. 30 In a review of 90 primary retroperitoneal neoplasms, Lane et al. 31 found 59 malignant and 31 benign masses, one of which was a cystic teratoma.
There are various theories regarding the origin of primary RT. They were once thought to arise from the earliest segmentation of the fertilized ovum. This theory is also known as the Blastomere Theory. 32 Another theory is that extragonadal teratomas come from incomplete conjoined twins. Instead of even division of the blastula to allow the separation of a twin, an incomplete division occurs, and only a small proportion of cells is separated forming the teratoma. 33 The most widely accepted theory is that they are vestiges of the wolffian and müllerian ducts or that they arise from pronephric or mesonephric tubules as it correlates with their midline and paramedian location. 34
Extragonadal teratomas can be located in decreasing order of frequency, in the anterior mediastinum, retroperitoneum, presacrum, coccygeal region, intracranium, neck, and abdomen. 14 Infrarenal locations of RT are uncommon compared with the commonly cited suprarenal location.34–36 In a review of 57 cases by Palumbo et al., 6 only 6 have been reported to be located below the kidneys with 4 on the left and 2 on the right side. An unusual retroperitoneal dumbbell-shaped cystic teratoma was reported in a 24-year-old female in Taiwan in 2004 which extended to the intraspinal region. 37
The location of the teratoma would coincide with the symptoms of compression of the adjacent structures such as vomiting, constipation, lumbar back pain, abdominal distention, and edema. Systemic symptoms may also be present such as fever, chills, night sweats, and weight loss.34,38–41 RT may present with chemical peritonitis from rupture of the cyst. 42 Retroperitoneal cystic teratoma can also get infected, and a case presenting as a subhepatic abscess has been reported in a postpartum woman. 43 Unusual presentations include ocular myasthenia gravis and hypertension which both resolved after excision of the cystic mass.44,45
The size of RT in adults is variable and can reach as large as 41 cm. RT have been reported to weigh as much as 31.6 kg and contain 3 L of cystic fluid.34,41,45
The occurrence of a primary RT beyond 50 years and in a male is extremely uncommon. As of the authors’ knowledge, only seven cases have been reported since 1769.6,14,46–49 The most recent report was on a 54-year-old male with a left suprarenal mass presenting as left upper quadrant abdominal and flank pain. 50
Teratomas are part of the family of non-seminomatous germ cell tumors. Totipotent cells differentiate into ectoderm, mesoderm, and endoderm components of the teratoma. They can be classified according to the number of layers present (mono-, bi-, or tridermal), epithelial lining (epidermoid, dermoid, or teratoid), degree of maturity of tissues (mature or immature), presence of malignant tissues, and content of tumor (cystic, solid components, or mixed).51,52
Risk of malignancy of these neoplasms ranges from 6.8% to 36.3% and increases with age, male sex, and presence of immature tissues and solid components.6,7,14,52,53 The earliest case of malignant transformation in a RT was reported in 1969 where an adenocarcinoma was arising from bronchial epithelium.36,54 Other documented cases of malignant transformation include neuroendocrine carcinoma (48 females), squamous cell carcinoma (65 females), and papillary renal cell-like carcinoma (36 males).55–57
In the 1990s, serum markers such as alpha-fetoprotein, carcinoembryonic antigen, lactate dehydrogenase, beta-human chorionic gonadotropin, CA 19-9, and CA 125 were detected from RT, but these were more associated with malignancies arising from the teratoma. 4 Elevated alpha-fetoprotein levels were found in 50% of immature teratomas and 6% in mature teratomas. 58 These serum markers are not specific to teratomas as they can be found in other diseases. These markers are evaluated pre-operatively to exclude other germ cell tumors and are followed up post-operatively to detect recurrence of the RT. 34 If the RT involves the adrenal gland, plasma catecholamines, renin, aldosterone, adrenocorticotrophic hormone, and cortisol levels may also be evaluated. 59
Since the cyst of our patient was found incidentally through imaging, the differential diagnosis of retroperitoneal cystic masses included a long list of neoplastic and non-neoplastic lesions. 60 The challenge in such cases is to differentiate the different cystic masses, despite the many overlapping features because management differs for each. Plain abdominal radiographs are part of the initial evaluation which will show calcifications but the findings are non-specific. 61 Ultrasound may show echogenic spots with acoustic shadows or dermoid plugs (Rokitansky body) but has limited sensitivity which makes CT scan the more appropriate imaging. CT scan findings indicative of primary RT include well-circumscribed fluid component, hypoattenuating fat, and calcifications which were found in our patient.2,10,62,63 Although MRI was not part of the evaluation in this patient, MRI may have a role of demonstrating invasion of the adjacent organs and delineating cyst contents such as fat which is highly suggestive of teratoma. CT-guided biopsy may be helpful in the diagnosis of such cases; however, it may not sample all the areas with the possibility of missing on the immature and malignant tissues that may be present.21,63
Complete excision of the mass was the primary method of management of these neoplasms with involved significant morbidity and mortality.6,7,14 However, in 1995, the first laparoscopic removal of a benign retroperitoneal teratoma was reported. 64
Few cases have been reported from 1880s where the cyst was first evacuated leaving the cyst wall in place with good post-operative outcomes. Other historical methods of RT management include marsupialization where the cyst was first emptied and then the cyst wall was everted and sutured on the skin. 11 Laparoscopic surgery is the preferred approach, especially when the cyst is well circumscribed on imaging.34,64 Surgical resection through laparotomy was done in our case due to the massive cyst size and the 3%–6% rate of malignant transformation in older males.61–63,65,66
Adjuvant chemotherapy and radiotherapy are necessary when RT harbors malignancy, especially germ cell carcinomas. Malignant teratomas behave like advanced testicular germ cell tumors, thus platinum-based chemotherapy is used. Teratomas with malignancies are highly resistant to chemotherapy and radiotherapy with an overall response rate of 61%.34,67–70
Since there are fewer reports of RT, there is little data for assessment of prognosis which depends on the type of tissues that the teratoma contains. With complete excision of the benign cyst, prognosis is excellent. However, if left untreated, mortality and morbidity are much higher due to obstruction of nearby viscera or metastasis from malignancies arising from the RT.7,11,34 Continued long-term post-operative follow up is recommended to detect early recurrence.
Conclusion
Retroperitoneal mature cystic teratoma in an older male is extremely rare. Primary gonadal teratoma with retroperitoneal metastasis should be excluded first. Evaluation of age and location of tumor are critical for its prognosis. Complete excision of tumor is necessary to evaluate whether there are immature and solid elements which need long-term follow up due to the increased risk of malignancy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.