
Abstract
A 79-year-old woman was admitted to our hospital for ischemic necrosis of the right first toe. During having normal lipid profiles, such as low-density lipoprotein cholesterol and triglyceride, plasma levels of lipoprotein(a) (Lp(a)] were abnormally high (141 mg/dL). She had a history of heart failure (HF) due to aortic valve stenosis (AS) and drug-eluting coronary stenting due to angina pectoris. To avoid worsening of HF and limb ischemia during minor amputation, she underwent balloon aortic valvuloplasty and endovascular therapy. She was also placed on proprotein convertase subtilisin/kexin type 9 inhibitors (140 mg of evolocumab) every 2 weeks, which decreased her plasma Lp(a) levels to 105 mg/dL (26% decrease) at discharge. Elevated plasma Lp(a) levels could strongly affect the development of AS and progression of systemic atherosclerosis. The screening and treatment of increased plasma Lp(a) are imperative for patients with AS having peripheral arterial disease.
Keywords
Introduction
An increase in plasma lipoprotein(a) (Lp(a)) levels has been identified as a risk factor for atherosclerotic cardiovascular disease (ASCVD), including coronary artery disease (CAD) and peripheral artery disease (PAD),1 –4 independent of low-density lipoprotein cholesterol (LDL-C) levels. 4 Increased plasma Lp(a) levels have also been closely associated with the development of aortic valve stenosis (AS) 5 and increased risk of AS in patients with PAD. 6 We herein describe a patient with hyperLp(a)emia who had CAD with AS and PAD. To prevent worsening heart failure (HF) and promote adequate wound healing after amputation surgery, we performed balloon aortic valvuloplasty (BAV) for AS and endovascular treatment (EVT) for recanalization of chronic total occlusion (CTO) in the superficial femoral artery (SFA). Moreover, the patient was placed on proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors to decrease the plasma Lp(a) and LDL-C levels.
Case description
Our patient was a 79-year-old non-smoking Japanese woman who presented with necrosis of the right first toe with intractable pain at rest (Figure 1(a)). She was admitted to our hospital for further evaluation and treatment of critical limb ischemia (CLI). Identified cardiovascular risk factors included hypertension, diabetes mellitus (DM), and dyslipidemia, for which she had been medicating for 8 years (10 mg/day of amlodipine for hypertension, 20 mg/day of teneligliptin for DM, and 4 mg/day of pitavastatin for dyslipidemia). Her blood pressure (120–130/50–60 mmHg) and glycated hemoglobin A1c (HbA1c) levels (6.0%–6.4%) were relatively well controlled over the last 3 years. On admission, her blood pressure and HbA1c levels were 131/54 mmHg and 6.2%, respectively. Lipid markers showed an LDL-C, high-density lipoprotein cholesterol, and triglycerides levels of 106.3, 52.7, and 147 mg/dL, respectively. Although LDL-C levels were over 100 mg/dL upon admission, they were controlled between 80 and 90 mg/dL through statins before admission. Furthermore, her lipid profile was comprehensively examined given her family history of premature CAD, with her mother having an acute myocardial infarction in her 40s. Plasma Lp(a) levels, which were measured using the latex-enhanced immunoturbidity method (SRL Inc., Tokyo, Japan), were markedly elevated at 141 mg/dL (normal range, < 30 mg/dL). She had a medical history of a hospitalization for HF associated with a moderate AS, with a calculated aortic valve (AV) area of 1.34 cm2 and mean aortic valve pressure gradient of 30 mmHg. She also had a history of treatment for unstable angina pectoris with percutaneous coronary intervention, for which a drug-eluting stent was implanted in the left main trunk to the left anterior descending coronary artery and in the proximal right coronary artery. On admission, her food had a clinical stage of Fontaine IV and Rutherford 5 in the right side; Fontaine I and Rutherford 0 in the left side. 7 The ankle-brachial pressure index (ABI) was 0.35 in the right side and 0.92 in the left side. 7 Computed tomographic angiography revealed that her right SFA was totally occluded with severely calcified plaques and no patent vessels below- the knee (Figure 1(c)). Based on the aforementioned findings, primary minor amputation to relieve her rest pain and revascularization of the right extremity was considered to promote postoperative wound healing. Transthoracic echocardiography (TTE) on admission showed a peak aortic jet velocity of 5.7 m/s, mean aortic pressure gradient of 65 mmHg, and calculated AV area of 1.10 cm2, which suggested AS progression. Given the likelihood that severe AS was an important trigger for HF, BAV was planned for first-line treatment of AS, followed by revascularization via EVT for the right SFA.
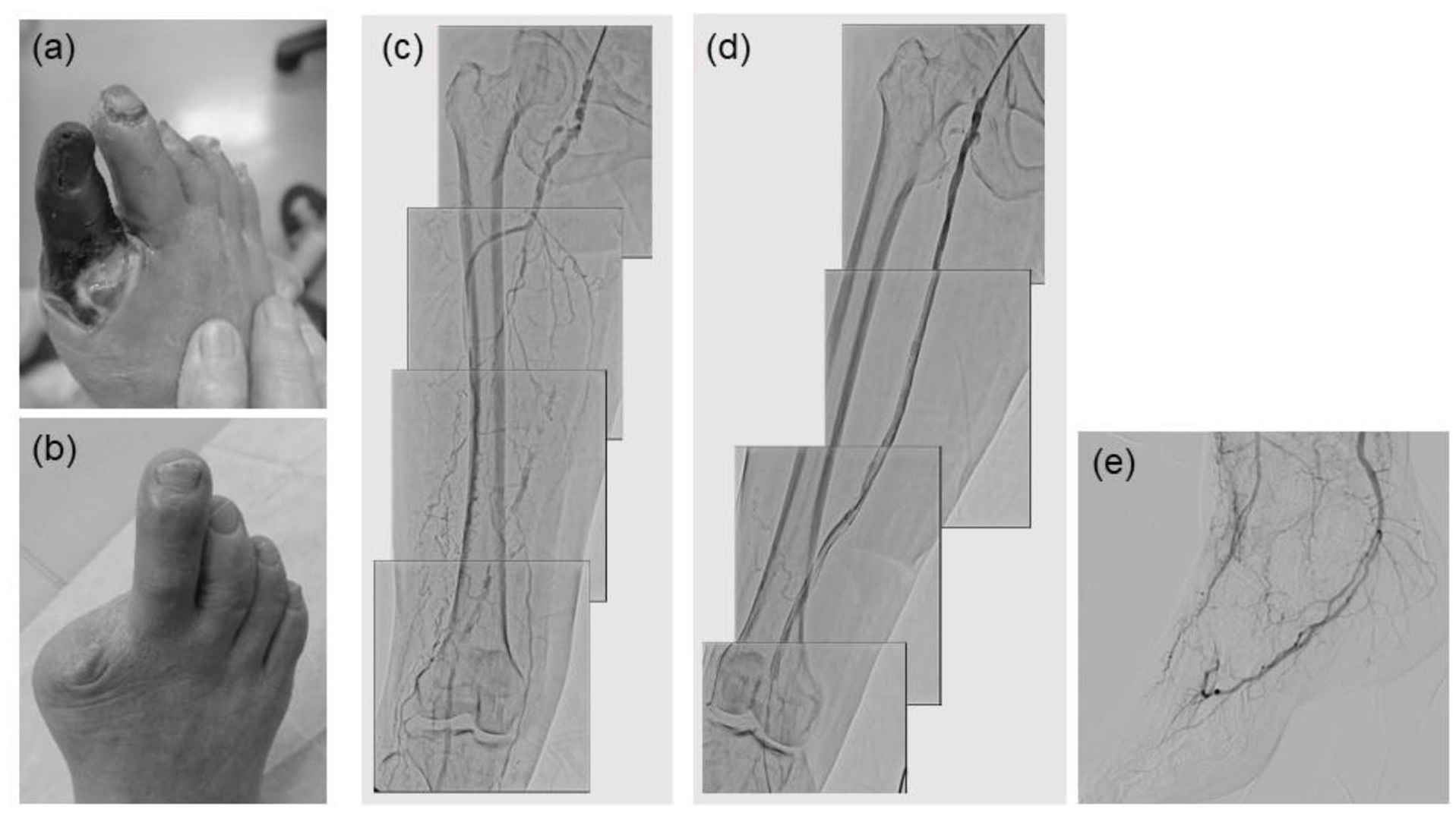
Necrosis of the right first toe (a: on admission; b: 3 months after amputation). Angiography of the right superficial femoral artery before (c) and after endovascular treatment (EVT) (d). Angiographic image showing favorable blood flow in the dorsal and plantar arteries after EVT (e).
On the fourth day of admission, BAV was performed via the femoral artery using the retrograde approach. The AV was crossed with a 0.035-inch supper stiff guide wire via the retrograde approach using a 4-Fr diagnostic catheter. An 18 mm INOUE balloon (Toray Industries, Inc., Tokyo, Japan) was then advanced over the wire and positioned across the AV. We initially inflated the INOUE balloon to a diameter of 18 mm and then incrementally increased it by 1 mm until 20 mm (Figure 2(b)). Inflations were repeated five times for each size. The right ventricle was placed at 180 bpm to stabilize the balloon position during inflation. A subsequent hemodynamic study showed that the mean trans-aortic pressure gradient improved from 46 (Figure 2(a)) to 26 mmHg (Figure 2(c)) (43% decrease) and the AV area from 0.80 to 1.13 cm2 (41% increase). Cardiac output also increased from 3.97 to 4.31 L/m after the final balloon dilatation. On follow-up TTE study, mild aortic regurgitation had not worsened. On the eighth day of admission, EVT was performed using the crossover technique from the contralateral side. A 6-Fr 45 cm Destination Peripheral Guiding Sheath (Terumo Corp., Tokyo, Japan) was inserted in retrograde fashion into the left common femoral artery (CFA) after successful right CFA puncture. A 0.014-inch guide wire was used to cross the peripheral CTO lesion in the right SFA using the conventional technique. EVT was performed using a 5.0 × 60 mm Sterling balloon (Boston Scientific Corp., MA, USA) and a 5.0 × 300 mm Ultraverse RX balloon (C. R. Bard, Inc., NJ, USA) with several overlapping inflations. Subsequently, stenting was performed using 6.0 × 120, 6.0 × 120, and 6.0 × 80 mm Eluvia drug-eluting stents (Boston Scientific Corp., MA, USA). Thereafter, post-dilatation was performed using a 5.0 × 300 mm Ultraverse RX balloon. No residual stenosis and dissection in the CTO lesion after stenting were observed. The final angiography showed complete revascularization from the SFA to the dorsal and plantar arteries (Figure 1(d) and (e)). The right ABI improved to 0.80, whereas the skin perfusion pressures in the dorsal and plantar region were 67 and 75 mmHg, respectively. On the 12th day of admission, she underwent right first toe amputation.

Simultaneous pressure tracings from the left ventricle and aorta. Pressure tracing before balloon aortic valvuloplasty (BAV) showing a maximum pressure gradient of 46 mmHg and aortic valve area of 0.80 cm2 (a). Balloon inflation with an 18- to 20 mm INOUE balloon catheter under rapid right ventricle pacing (b). Pressure tracing after BAV showing a maximum pressure gradient of 26 mmHg and aortic valve area of 1.13 cm2 (c).
She was given PCSK9 inhibitors (140 mg of evolocumab) every 2 weeks just after admission, which decreased her plasma LDL-C and Lp(a) levels from 106.3 and 141 mg/dL at admission to 54.7 and 105 mg/dL at discharge (49% and 26% decrease), respectively (Figure 3). After adjusting her plasma LDL-C levels using Dahlen’s modification, 8 a decrease from 66.6 mg/dL at admission to 16.6 mg/dL at discharge was noted (75% decrease).

Changes in plasma lipoprotein(a) (Lp(a)) and low-density lipoprotein cholesterol (LDL-C) levels before and after proprotein convertase subtilisin/kexin type 9 administration.
The patient was discharged from our hospital on the 21st day of admission, and successful wound healing after the amputation was achieved without superficial or deep incisional surgical infection 3 month later (Figure 1(b)). She also remained free from HF symptoms for 3 months since the BAV procedure.
Discussion
This case report details our experience with a patient having CAD with elevated plasma Lp(a) who underwent catheter interventions for AS and PAD. After administering PCSK9 inhibitors aimed at lowering Lp(a) levels, a change in plasma Lp(a) and LDL-C levels was observed.
The patient had compensated HF with preserved ejection fraction due to AS, with TTE revealing gradual AS progression after the initial hospitalization for HF. Traditional surgical AV replacement (SAVR) or transcatheter AV implantation (TAVI) needed for release of AS was considered for this patient. However, given that the preoperative inflammation response to CLI could potentially increase the risk of infection (e.g. infective endocarditis) after SAVR or TAVI, we instead opted for BAV. Despite its high efficacy and acceptable levels of perioperative complications in patients with severe AS, 9 BAV provides only transient effects and serves as a bridging therapy to SAVR or TAVI,10,11 which should be performed no later than 6 to 11 months after BAV. 9
Studies have identified elevated plasma Lp(a) levels as an independent risk factor for the development of atherosclerosis and a strong predictor of future cardiovascular events.1 –5 Moreover, epidemiologic have shown a 13% and 10% increased risk for coronary heart disease and ischemic stroke for each 3.5-fold increase in plasma Lp(a) levels, respectively, 12 as well as a 37% increased risk for PAD for every 2.7- fold increase in the same. 4 Among healthy individuals, elevated plasma Lp(a) levels had also been associated with increased risk for AS, with levels > 90 mg/dL predicting a 3.0-fold increased risk. 13 Despite robust evidence showing that PAD frequently coexists with CAD, PAD has been closely associated with AS. Aronow et al. 14 reported that older patients with AS had a higher prevalence of symptomatic PAD compared to those without AS. Furthermore, Hojo et al. 6 reported that elevated plasma Lp(a) levels were associated with an increased risk of AS in patients with PAD. The aforementioned studies, as well the present case report, suggest the importance of screening for AV and plasma Lp(a) levels in patients with PAD.
Plasma Lp(a) levels can almost entirely by attributed to genetics given their strong association with genetic diversity of the apo(a) gene locus and Lp(a) polymorphisms with different molecular weights. With regard to phenotype, one study showed that smaller weights were associated with higher levels of Lp(a). 1 Although no genetic testing was performed in the current case, genome testing with mutation analyses would allow for a better understanding on the risk of ASCVD progression. Plasma Lp(a) levels over 30 mg/dL have been considered pro-atherosclerotic and are found in approximately 20% of the population. 15 In Japan, a population-based cohort study showed that Lp(a) levels ranged widely from 5 to 2150 mg/dL and were 80, 150, and 270 mg/dL at the 25th, 50th, and 75th percentile, respectively. 16 Although the Lp(a) values of the present case were not unusual, the aforementioned studies suggest that Lp(a) measurement is imperative in the management of patients with ASCVD. Moreover, the 2018 AHA/ACC guidelines recommended the same for patients with family history of premature ASCVD or personal history of ASCVD. 17
Lp(a) has been considered as one of the residual risk factors after statin therapy. 18 Although several therapies, such as antisense oligonucleotide-targeting hepatic apo(a) messenger RNA, are currently being developed clinically for patients with elevated Lp(a), 19 an effective and safe Lp(a)-lowering therapy has yet to be established. The FOURIER trial demonstrated that evolocumab, a monoclonal antibody to PCSK9 inhibitor strongly and sustainably reduced plasma Lp(a) levels. 20 Nonetheless, the mechanisms by which anti-PCSK9 antibody with evolocumab decreases plasma Lp(a) levels remain unclear. Furthermore, whether a large reduction in plasma Lp(a) levels could achieve a clinically meaningful reduction in cardiovascular events or slow progression of AS remains unclear to date. However, Lp(a)-lowering therapy should be considered in addition to current medical therapies even in patients with elevated plasma Lp(a).
Conclusion
This case report details our experience with a patient having CAD with elevated plasma Lp(a) levels who underwent catheter interventions for AS and PAD. Notably, after administering PCSK9 inhibitors as Lp(a)-lowering therapy, changes in plasma Lp(a) and LDL-C levels were observed. Given that hyperlipoprotein(a)emia strongly affects the development of AS and progression of systemic atherosclerosis, screening and treatment of AS and PAD, including CAD are imperative.
Footnotes
Author contributions
A.N. and H.E. conceived and designed the study. A.N., K.S., and M.K. collected data. A.N. wrote the paper. All authors read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent has been obtained from the patient(s) for their anonymized information to be published in this article.