
Abstract
Kaposi’s sarcoma is the most common AIDS-associated malignancy. Kaposi’s sarcoma in the oral cavity and oropharynx present as a macular, papular, or nodular lesion on the palate, gingiva, or tongue which may look pink, reddish, or purplish. Kaposi’s sarcoma of the tonsils is relatively less common compared with other sites in the oral cavity and oropharynx. We report a case of Kaposi’s sarcoma of tonsil with profuse bleeding requiring emergency tracheostomy to protect the airway followed by tonsillectomy to control the bleeding. Our initial diagnosis was hemangioma or a pyogenic granuloma. The patient tested positive for a retroviral infection and the histopathology report was compatible with Kaposi’s sarcoma. Antiretroviral therapy and radiotherapy were given after stabilizing the patient. Kaposi’s sarcoma of tonsils is relatively uncommon and it is unusual to cause profuse bleeding. Various treatment options are available but there are no standard treatment protocols. Treatments options depend on the site, size, stage, and immune status of the patient.
Introduction
Kaposi’s sarcoma was first described by Hungarian Dermatologist Moriz Kaposi in 1872. 1 It is a mesenchymal tumour that involves blood vessels and lymphatic tissues and is of multifactorial origin. 2 Viral oncogenes by human herpes virus-8 and cytokine-induced growth together with the immunocompromised state are some important conditions to develop this tumour. 2 Neo-angiogenesis, proliferation of spindle cells, inflammation, and oedema are characteristics of Kaposi’s sarcoma.1,3 As there is a lack of conventional clinical features of malignancy, it is classified as intermediate neoplasm and still there is a debate whether it is a reactive proliferation, true malignancy, or both. 3 Four major types of Kaposi’s sarcoma have been described: Classic, African endemic, immunosuppression or transplant-associated, and AIDS-associated. 3 AIDS-associated Kaposi’s sarcoma can involve any part of the skin on the body, most commonly on the lower limbs but it can also affect aerodigestive tract mucous membrane. 4
Kaposi’s sarcoma is the most common AIDS-associated malignancy, and the oral cavity is the initial site of manifestation in more than 20% of patients with AIDS-associated Kaposi’s sarcoma.1,5 Patients with AIDS have 20,000 times more risk of developing Kaposi’s sarcoma than the general population. 2 The most frequently involved sites in the oral cavity are palate, gingiva, and tongue, but any mucosal surface may be involved less frequently.1,5 Oral Kaposi’s sarcoma may be pink or purple and can be macular, papular, or nodular. 3 Incidence of Kaposi’s sarcoma has been reduced by 30%–50% after the introduction of highly active antiretroviral treatment (HAART) for HIV patients, but it still remains a common malignant disease in HIV patients. 5
Case history
A 26-year-old female foreign worker presented to ear, nose, and throat clinic with a history of foreign body sensation in the throat for 2 months. She had discomfort on swallowing but had no pain. For a few weeks, she noticed blood-stained saliva on and off which resolved by itself.
On examination, she looked emaciated and was febrile. There was a purplish mass of about 1.5 × 1.0 cm arising from the inferior pole of the left tonsil going towards the tongue base. The right tonsil looked normal. There were no other lesions in the oral cavity, pharynx, or larynx. Multiple sub-centimetre cervical lymph nodes were palpable on both sides of the neck. We did not find any skin lesions on her face, limbs, or body. Our differential diagnoses were hemangioma, pyogenic granuloma, and lymphoma. She was admitted to the hospital for further investigations. After the admission, she started to have profuse bleeding spontaneously from the left tonsillar mass, which could not be controlled by ice water gurgle or local pressure with gauze packs. She was rushed to the operating theatre for an emergency tracheostomy to protect the airway. After the airway was secured with a tracheostomy, we did a bilateral tonsillectomy to control bleeding and for pathological evaluation. The left tonsillar mass was friable, which came out in piecemeal, and continued to bleed a lot during the surgery. She received three pints of pack cells post-operatively as the haemoglobin has dropped to 6.0 g/dL. Blood report showed a white blood count of 7.6 × 109/L, neutrophil 37%, lymphocyte 49%, monocyte 12%, atypical lymphocyte 2%, platelets 84 × 109/L, and erythrocyte sedimentation rate was 140 mm in the first hour. She tested positive for both HIV and hepatitis B virus infections which were not known before. Histopathology examination of the lesion noted the proliferation of spindle-shaped cells with blood-filled spaces in between compatible with Kaposi’s sarcoma (Figure 1(a) and (b)). CD34 staining highlighted the spindle cells (Figure 2(a) and (b)). Computed tomography of the chest was normal, and bronchoscopy and lavage were negative for Kaposi’s sarcoma. Trephine biopsy of bone marrow was done to exclude the involvement of bone marrow which was also negative for Kaposi sarcoma. The tracheostomy tube was weaned off in a week and the patient was stable after 2 weeks of hospital stay. Our patient was started on HAART therapy (tenofovir, lamivudine, and efavirenz); and after the dental evaluation, she was given radiotherapy of 30 Gy in 10 fractions. Following the treatment, our patient clinically improved and her CD4 count improved from 286/μL on admission to 497/μL on discharge. She left for her country for the continuation of the treatment and we could not follow up.

(a) H & E x 40: Low power view showing proliferation of spindle-shaped cells forming small blood-filled vascular channels. (b) H & E x 100: Proliferation of the spindle-shaped cells with blood-filled spaces in between.
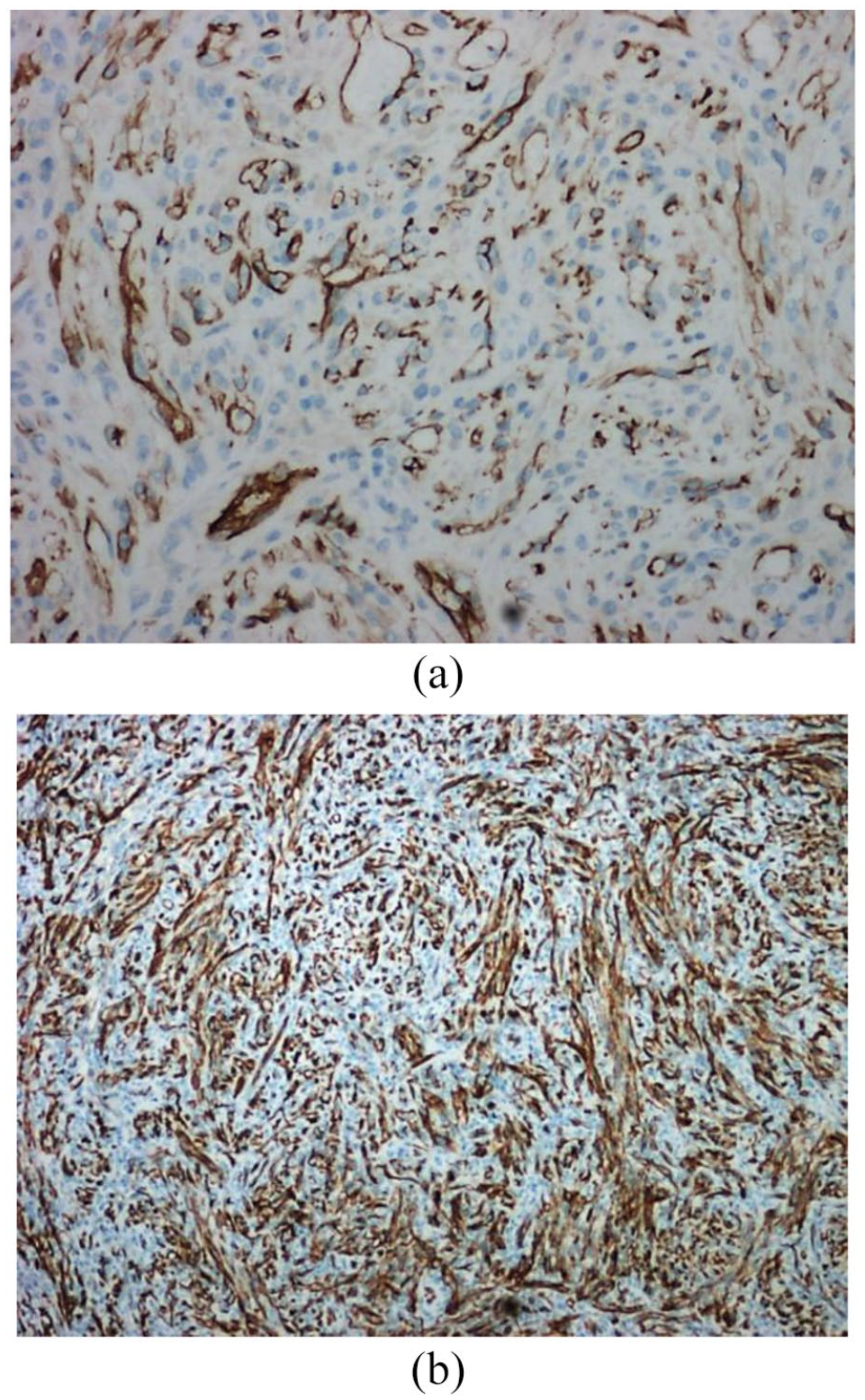
(a) CD34 highlights some of the spindle-shaped cells and Blood-filled spaces lined by endothelial cells. (b) CD34 highlights the spindle cells.
Discussion
Kaposi’s sarcoma is the most prevalent malignancy in patients with AIDS 6 and represents the first manifestation of AIDS in 30–40% of patients. 7 Twenty percent of the people infected with HIV develop oral Kaposi’s sarcoma mostly in their fourth and fifth decades of life. 8 Kaposi’s sarcoma is also reported in HIV-negative patients9–12 although it is uncommon. The incidence of Kaposi sarcoma in the general population is 1 in 100,000 compared with about 1 in 20 in HIV-infected individuals. 13 AIDS-associated Kaposi’s sarcoma is the most aggressive form, skin being the most typical site of occurrence. 1 Involvement of the oral cavity and oropharynx can occur without skin involvement as in our case. Kaposi’s sarcoma is often progressive in AIDS patients and likely to involve multiple organ systems. 14
Depending on the site and size of the lesion, patients with Kaposi’s sarcoma of the oral cavity and pharynx may present with difficulty in swallowing,12,15 abnormal sensation in the throat, 15 or present with a mass 1 which are generally painless.2,3,7,8,16–18 Some cases may present with blood-stained saliva or some bleeding;4,8,17 however, profuse bleeding requiring tonsillectomy and tracheostomy has not been reported to our knowledge. The lesions which may look pink,2,3 purplish1,15,17,18 or reddish 15 may be macular, 3 papular,3,18 nodular3,8,10,15,18 or pedunculated.19,20
Numerous treatment methods have been developed like radiotherapy, laser, intralesional chemotherapy, cryotherapy (liquid nitrogen), surgical excision, and systemic chemotherapy. 2 Selection of treatment options depends on the extent and rate of tumour growth, disease stage, lesion distribution and evolution pattern, symptoms, immune status, and concurrent complications of HIV infection as there are no standard therapy protocols. 13 In cases with fewer than five lesions and when the immune deficit is moderate, local treatment such as external radiotherapy, cryotherapy, laser, surgery, and in situ chemotherapy may be given. 7 Local treatments may be considered first as systemic chemotherapeutic agents may cause myelosuppression and radiotherapy causes severe mucositis. 6 Surgical excision of the lesion and intralesional chemotherapy may be useful to reduce symptoms if systemic chemotherapy does not reduce the size of the lesion. 15 In HIV-negative Kaposi’s sarcoma, only surgical excision of the lesion has prevented recurrence.9,12 Newer treatment option with diode laser has been described recently to be successful without recurrence at 6 months. 18 Our case was managed with bilateral tonsillectomy followed by HAART and radiotherapy to prevent recurrence as the tongue base was involved. Systemic chemotherapy was not given as there was no evidence of systemic involvement at that time although gastroscopy and colonoscopy should have been done.
HAART therapy and improvement of immune function have been shown to cause regression of the lesion of AIDS-associated Kaposi’s sarcoma. 16 However, Kaposi’s sarcoma still represents the second most frequent tumour in HIV-infected patients. 13
Conclusion
Kaposi’s sarcoma of the tonsils is less common compared with other sites in the oral cavity and oropharynx. It may cause uncontrollable and profuse bleeding which may require emergency tracheostomy and tonsillectomy to protect the airway and control the bleeding. We recommend taking a biopsy of a Kaposi’s sarcoma suspected lesion in a controlled setting.
Footnotes
Acknowledgements
We thank the patient for consenting to share her clinical history and the reviewers of this article for their valued recommendations.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest concerning this case report, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.