
Abstract
Pleomorphic adenoma is a common, benign neoplasm typically located in the major salivary glands. The external auditory canal is an atypical location for a pleomorphic adenoma to originate. Wide surgical excision is essential in cases of pleomorphic adenoma due to its tendency to recur and change into malignancy. We report a case of pleomorphic adenoma emerging in the external auditory canal, which is an atypical location for it to originate. A 23-year-old male presented with swelling and decreased hearing in the left ear for 2 months. On examination, there was a smooth, pink, firm swelling in the cartilaginous part of external auditory canal. Pure tone audiogram and computed tomography of temporal bone were performed. The patient underwent excision biopsy and the diagnosis of pleomorphic adenoma was confirmed after histopathology. Long-term follow-up is recommended as pleomorphic adenoma has the potentiality to recur or transform into malignancy.
Introduction
Pleomorphic adenoma is a benign neoplasm commonly arising from the major salivary glands. Occasionally, it originates from the minor salivary glands within the palate, buccal mucosa, or the lips. 1 Pleomorphic adenoma in the external auditory canal is extremely rare and was first reported by Mark and Rothberg in 1951. 2
The external auditory canal consists of sebaceous glands and the modified apocrine glands termed as ceruminous glands. The glandular tumors of external ear have been classified by Wetli et al. into four categories, namely, ceruminous adenoma, pleomorphic adenoma, adenoid cystic carcinoma, and ceruminous adenocarcinoma. 3
Due to the peculiarities of pleomorphic adenoma, such as recurrence and malignant transformation, 1 clinician should consider it in the differential diagnosis in cases of swelling in the external auditory canal. We report a case of pleomorphic adenoma in the external auditory canal, which is an atypical location for it to originate.
Case report
A 23-year-old male patient presented to the Department of Otorhinolaryngology of our hospital with swelling in left ear and decreased hearing on the same side for 2 months. On examination, there was a pink, smooth, firm mass in the cartilaginous part of external auditory canal. The tympanic membrane could not be visualized due to the mass. There was no parotid swelling and cervical lymph nodes were impalpable.
Pure tone audiometry was performed and there was 28 decibel mild conductive hearing loss on the left ear. The high-resolution computed tomography (HRCT) of the temporal bone showed a 1 cm smooth growth arising from the anterior wall of cartilaginous part of left external auditory canal without any bony erosion and the middle ear was normal (Figure 1). Under local anesthesia, excision biopsy of the lesion was performed using endaural approach. Peroperatively, there was a 1.5 × 1 × 1 cm, well-defined, smooth, whitish, firm mass attached to the anterior canal wall which was easily dissected from the underlying cartilage and overlying skin.

High-resolution computed tomography of temporal bone with an arrow indicating to a smooth soft tissue density arising from anterior wall of cartilaginous external auditory canal.
The postoperative biopsy report showed epithelial and stromal elements. The epithelial components were arranged in tubular structures and sheets, with outer layer of myoepithelial cells. The stroma showed chondromyxoid materials (Figure 2). There was no malignant change and the pathological diagnosis of pleomorphic adenoma of the external auditory canal was confirmed.
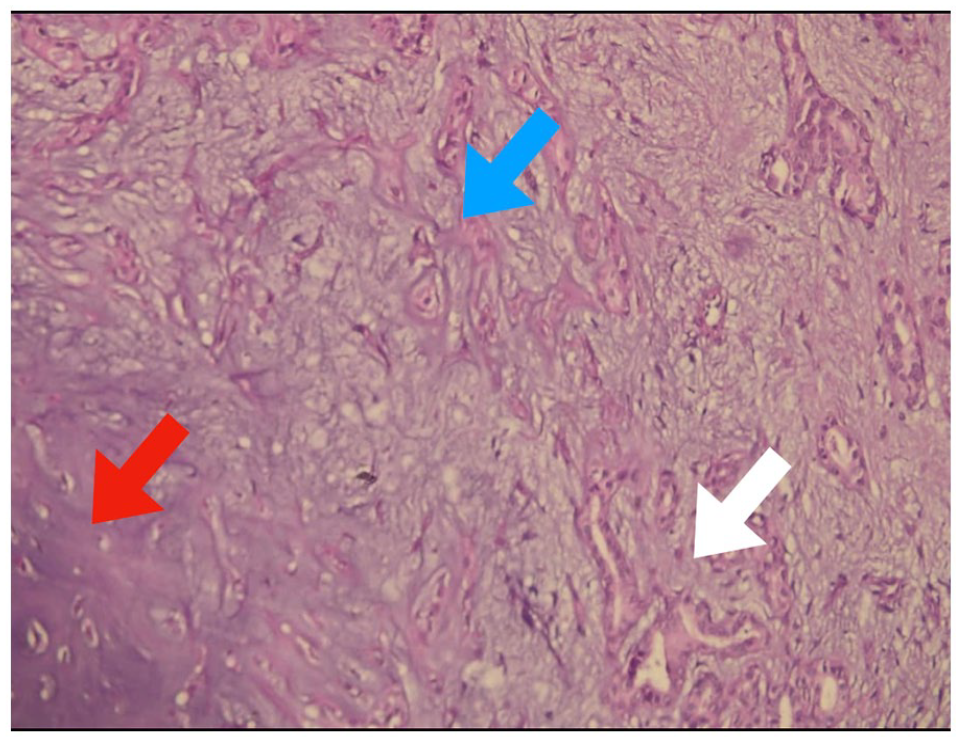
Epithelial and myoepithelial cells arranged in tubules within chondromyxoid stroma.
The patient was disease free at 1-year follow-up with normal hearing and advised to review regularly.
Discussion
Pleomorphic adenoma in the external auditory canal is a very rare entity and its origin is debatable. 4 In the past, it was believed to originate either from the ectopic salivary tissues or from direct extension of tumors of the parotid glands. However, the current literatures support that pleomorphic adenoma originates from the ceruminous glands.4,5 Collins and Yu studied the histochemical, immunohistochemical, and electron microscopic pictures of pleomorphic adenoma of the external auditory canal and concluded its origin likely to be from the ceruminous glands. 5
The World Health Organization has classified ceruminous neoplasms of the external auditory canal as benign neoplasms constituting ceruminous adenoma, ceruminous pleomorphic adenoma and ceruminous syringocystadenoma papilliferum, and malignant neoplasms constituting ceruminous adenocarcinoma, ceruminous adenoid cystic carcinoma, and ceruminous mucoepidermoid carcinoma. 6 Pleomorphic adenoma is characterized by subepithelial proliferation of glandular structures and myoepithelial cells adjacent to mucoid, myxoid, or chondromyxoid stroma. 7
The mean age for presentation of pleomorphic adenoma is fifth decade; however, it may range from 12 to 85 years. 8 There is no any gender predisposition. The clinical symptoms could be nonspecific such as aural fullness or sense of occlusion, hearing loss, otalgia, growth in the ear canal (usually noticed by others), and otorrhoea. The commonest site of origin of the tumor is posterior or posterosuperior canal wall; 4 however, in this case, the tumor arose from the anterior canal wall.
Fine needle aspiration cytology (FNAC) from the swelling may be performed to distinguish between benign and malignant neoplasms. 9 Computed tomography (CT) scan and magnetic resonance imaging (MRI) would be helpful to formulate the diagnosis and decide the surgical approach. In CT scan, pleomorphic adenoma would be visualized as a well-defined smooth mass without bony erosion. In MRI, the tumor would usually be hypointense on T1-weighted image and hyperintense on T2-weighted image. 10
The definitive treatment of pleomorphic adenoma of external auditory canal is wide surgical excision with safe margins. 8 Most cases are approached through postauricular or endaural incision. At times, endoscopic surgical resection may be performed. 11 Adequate surgery and long-term follow-up is mandatory because of its potentiality to recur and convert into malignancy. Botha and Khan reported the first malignant relapse of pleomorphic adenoma with satellite nodules 3 years after the first excision. 12 The chance of tumor recurrence increases if the margin is inadequate or if the tumor ruptures during surgery.
Conclusion
Pleomorphic adenoma is an extremely rare benign tumor of the external auditory canal arising from the ceruminous glands. Unlike other benign tumors, it has peculiarity to recur and convert into malignancy. Therefore, wide surgical excision and long-term follow-up is crucial for proper patient management.
Footnotes
Acknowledgements
The authors acknowledge the immense help and support received from the Department of Otorhinolaryngology and Pathology, Tribhuvan University Teaching Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.