
Abstract
Cryptococcus neoformans is an encapsulated, yeast-like fungus that can cause a systemic mycosis, particularly in immunocompromised patients. Disseminated infections typically affect the central nervous system, and osseous lesions are infrequent. Only 5%–10% of disseminated cryptococcosis involves bones. A 69-year-old female presented pain, swelling, and a soft tissue mass in her right lateral hindfoot. Her medical history included a kidney transplant (10 years earlier) secondary to chronic disease due to IgA nephropathy. The patient underwent an excisional biopsy, surgical debridement, and secondarily negative pressure wound therapy to achieve skin closure. Biopsy revealed a rare Cryptococcus neoformans osteomyelitis of the calcaneus. The patient then received IV treatment with liposomal amphotericin B at 3 mg/kg/d for 25 days. In conclusion, we present a case of cryptococcal osteomyelitis which, although not a frequent disease, must be considered as one of the differential diagnoses of osteolytic osseous lesions in patients with chronic osteomyelitis. Cryptococcus neoformans may be a potential cause of below-knee infection, mainly in immunocompromised patients.
Introduction
Cryptococcus neoformans is an encapsulated, yeast-like fungus that can cause systemic mycosis, particularly in immunocompromised patients (ICP).1–3 After inhalation, the organism may remain localized in the lungs or disseminate hematogenously, causing a systemic fungemia with numerous extrapulmonary infection sites. 4 ICP with sarcoidosis, Hodgkin’s disease, leukemia, and AIDS, and those with long-term use of corticosteroids are predisposed to develop cryptococcosis. 5
Disseminated infections typically affect the central nervous system, and osseous lesions are infrequent. Only 5%–10% of disseminated cryptococcosis involve bones. 6 It may affect immunocompetent patients in bone locations such as first metatarsal head, 7 talus, 8 vertebra, 9 iliac bone, 10 femur,11,12 and combination of sites.13–15 Cryptococcosis may lead to significant morbidity and mortality since it may become fatal if not treated adequately. 16 More frequently, other microorganisms may cause calcaneal osteomyelitis (CO). A recent systematic review showed that Staphylococcus aureus was the most common organism involved. 17
To our knowledge, we report the first case of cryptococcal CO in an ICP. The patient was informed that data concerning the case would be submitted for publication, and consent was provided.
Case report
A 69-year-old female presented pain, swelling, and a soft tissue mass in her right lateral hindfoot; this symptom had presented for 2 months. She also had a persistent fever (38°C–39°C) for the previous 3 days, and the signs were not related to any injury or trauma.
Her medical history included a kidney transplant (10 years before) secondary to chronic disease due to IgA nephropathy. Also, she presented several episodes of urinary infection treated with antibiotics and double J catheter placement. Patients have been treated with deltisone (prednisone) (4 mg/day) as a transplant treatment.
On admission to our institution, her body temperature was 37°C, her heart rate was 106/min, and her blood pressure was 133/101 mm Hg. The peripheral blood white cell count was 2800 mm3 (58% neutrophils), and the erythrocyte sedimentation rate (ESR) was 28 m/h. Physical examination revealed a painful soft tissue mass (3 cm × 3 cm approximately) and tenderness in the lateral hindfoot on palpation, with associated pain when weight-bearing. The patient was tested for HIV, and the result was negative.
Radiographs showed a calcaneal tuberosity osteolytic lesion with marginal sclerosis and no associated periosteal reaction (Figure 1). No lesion was found on the chest X-ray. Magnetic resonance imaging (MRI) (T2-weighted) showed a 3.2 cm × 3.0 cm × 2.8 cm infiltrative hyperintense lesion with geographic margins. Posterolateral cortex erosion and significant bone and soft tissue edema were also observed (Figure 2).

(a) Preoperative soft tissue mass on lateral region of right calcaneus. (b) Preoperative lateral radiograph showing a lytic lesion on calcaneal tuberosity without periosteal reaction. No acute fracture was noted.

Sagittal (a) and axial (b) T2-weighted MRI showing a 3.2 cm × 3.0 cm × 2.8 cm infiltrative hyperintense lesion with geographic margins. Erosion of the posterolateral cortex and significant local edema. (c). Sagittal T1-weighted MRI.
Based on clinical examination and IMAGEN study results, excisional biopsy, surgical debridement, and secondarily negative pressure wound therapy (NPWT) were indicated. Intraoperatively, the lesion extended through the soft tissues and the underlying bone. Soft tissue found inside the cavitary was a soft, gray, mucoid, and gelatinous mass associated with purulent secretion (Figure 3). The lesion was removed, and the cystic bone defect was curetted until vital bone was obtained. Due to the soft tissue and bone defect, we used NPWT to achieve neovascularization and granulation.
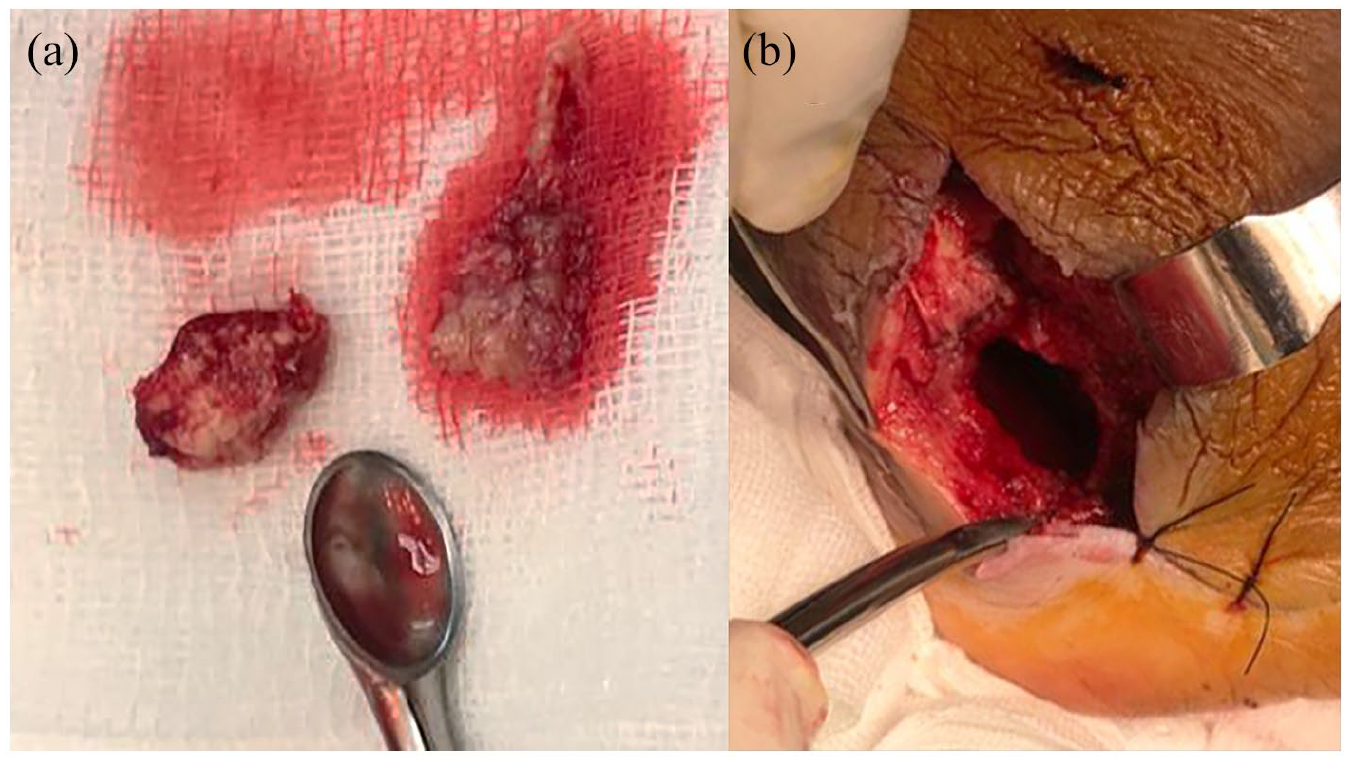
(a) Gross specimens showing a soft, gray, mucoid, and gelatinous mass associated with purulent secretion. (b) Cavitary defect after complete resection of the lesion.
Cryptococcus neoformans was histologically found as spherical or yeast-like organisms within the cytoplasm of macrophages, and no granulomas were seen (Figure 4). The patient received IV treatment with liposomal amphotericin B at 3 mg/kg/d for 25 days, followed by oral 400 mg/d orally for 8 weeks.

(a) The histologic specimens showed the appearance of Cryptococcus neoformans into the cytoplasm of macrophages (arrow), hematoxylin and eosin staining (a) (×400), and periodic acid–Schiff (PAS) staining (inset) (×400) (b).
As a cavitary defect was generated, two-stage wound closure was designed. First, NPWT was used for 8 days to improve wound healing conditions. Although the extent of the defect was near the Achilles tendon insertion, immediate weight-bearing was allowed using a walker boot.
When the NPWT was removed, the skin was closed. The pain had progressively reduced at 2-year follow-up, and the patient was completely recovered and walking normally (Figure 5). MRI showed a slight decrease in the lesion size (Figure 6).

(a) Clinical image showing complete healed lesion. (b) Postoperative lateral radiograph at 1-year follow-up.

Sagittal (a) and axial (b) T2-weighted MRI showing a slight reduction of the hyperintense lesion.
Discussion
Cryptococcal opportunistic infections are quite frequent in ICP; hence, the diagnosis and treatment of osteomyelitis have become more challenging. 18 Sarcoidosis is the most common underlying condition associated with this infection, followed by tuberculosis and long-term use of corticosteroids. 19 The patient presented had been receiving corticosteroids for 10 years following a kidney transplant.
Although lungs and central nervous systems are the most frequently affected,20–22 it may affect other tissues. 23 Only 5%–10% of disseminated cryptococcosis affects bones. 6 Cryptococcal osteomyelitis presumably occurs via hematogenous spread from a pulmonary focus, but direct inoculation through the skin is also possible.20,24 Spine infection is the most commonly reported osteomyelitis site, while other frequent sites are pelvis, femur, and ribs.20,21,23,25,26 We present an ICP with a rare or unique presentation of cryptococcal osteomyelitis on lower limb.
Based on analysis of published studies, the clinical presentation of the patient is invariable. Usually, patients show progressive soft tissue swelling and tenderness associated with systemic manifestations such as fever. 24 Also, most patients typically have normal white cell count and variably elevated ESR. In a recent review, only 7 of 39 cases patients were febrile. Before diagnosis, the median duration of symptoms was 3 months (range = 2 weeks to 33 months), and the leukocyte count was generally normal.20,23 Our patient showed soft tissue swelling and pain, but laboratory parameters were normal.
The radiographic appearance of cryptococcal osteomyelitis is consistently erosive or lytic with little or no periosteal reaction.19,26 While many of these lesions have well-defined geographic borders, this is not a constant finding. 27
Such features are not specific for cryptococcus and may be commonly shared by several conditions, including other infectious etiologies (such as other fungi, Actinomyces, mycobacteria, and Brucella) or neoplastic processes. Reliance on the presence of a periosteal reaction may be confusing. Several reports of patients with cryptococcal osteomyelitis were initially diagnosed as a malignant neoplastic process due to an extensive periosteal reaction.19,28 Also, cortical destruction with an associated purulent soft tissue fluid collection is frequent. 11 This case showed the characteristics mentioned (lytic, no periosteal reaction, and cortical destruction) associated with a purulent soft tissue mass.
Published studies indicate surgical debridement associated with antifungal therapy as a curative treatment for cryptococcal osteomyelitis.23,24 In reported cases, antifungals alone and rarely surgical debridement alone have demonstrated a healing effect.20,29 The primary goals of surgical intervention are to lessen the infectious burden and to avoid adjacent soft tissue involvement. This is achieved by removing the bony sequestrum and carefully debride the surrounding soft tissue affected. This patient was treated with surgical debridement associated with antifungal therapy with the addition of NPWT. NPWT is a widely used technology in acute, 30 chronic and postoperative wounds,31,32 and chronic osteomyelitis.33–35 It provides moist wound conditions, reduces exudate, control wound-bed infection, and stimulates granulation. 36 Secondary wound closure was done after removal of NPWT. Although partial and total calcanectomies or even amputation may be suitable for treating other types of CO, we decided to do a conservative surgical procedure (because of size and low fracture risk) to preserve function. A more radical treatment was deferred if the clinical evolution was not as expected.17,37 Reported lower limb cases and outcomes are summarized in Table 1.
Published reports of osteomyelitis caused by Cryptococcus neoformans on the lower limb.

Given the suspicion for disseminated disease, surgery should always be followed by appropriate chemotherapy. Antifungal chemotherapy usually includes a combination of amphotericin B and 5-flucytosine or fluconazole. 38 Single-agent therapy is generally avoided since secondary drug resistance has been reported. 23 The duration of chemotherapy needed for remission is not well determined and should be based on clinical and radiological improvement.20,23 The patient presented received amphotericin B without presenting adverse effects.
Conclusion
In conclusion, we present a case of cryptococcal osteomyelitis, which, although not a frequent disease, must be considered one of the differential diagnoses of osteolytic osseous lesions in patients with chronic osteomyelitis. It is a rare but treatable disease, particularly in immunocompromised hosts, in whom it may lead to significant morbidity and mortality. We believe that surgical debridement combined with systemic antifungal chemotherapy is the treatment of choice. NPWT is a helpful tool to treat chronic infections with cavitary defects.
Footnotes
Acknowledgements
All authors are equally conceived and designed the study, conducted research, provided research materials and collected and organized data, and analyzed and interpreted data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.