
Abstract
With an increased interest in youth sports, the burden of overhead throwing elbow injuries accompanying early single-sport focus has steadily risen. During the overhead throwing motion, valgus torque can reach and surpass Newton meters (N m) during the late cocking and early acceleration phases, which exceeds the tensile strength (22.7–33 N m) of the ulnar collateral ligament. While the ulnar collateral ligament serves as the primary valgus stabilizer between and degrees of elbow flexion, other structures about the elbow must contribute to stability during throwing. Depending on an athlete’s stage of skeletal maturity, certain patterns of injury are observed with mechanical failures resulting from increased medial laxity, lateral-sided compression, and posterior extension shearing forces. Together, these injury patterns represent a wide range of conditions that arise from valgus extension overload. The purpose of this article is to review common pathologies observed in the adolescent overhead throwing athlete in the context of functional anatomy, osseous development, and throwing mechanics. Operative and non-operative management and their associated outcomes will be discussed for these injuries.
Introduction
With over an estimated 8.6 million participants in youth baseball alone, increased participation in youth sports has been accompanied by a corresponding increase in the number of elbow injuries in young athletes. 1 Overhead-throwing athletes, specifically single-sport focused baseball pitchers, have been disproportionately affected with a greater number of athletes experiencing injury to the elbow.2,3 While mounting evidence suggests that skeletally immature athletes who engage in single-sport specialization are subject to detrimental effects with regard to performance, short- and long-term injury risks, and joint health, the emphasis placed on early single-sport specialization to succeed at the highest level of competition has been called into question.4,5 In addition, Fleisig and Andrews noted a 22-fold increase in ulnar collateral ligament (UCL) tears at their institution from 1994 to 2010, with many of these injuries occurring in high school athletes. 2 In early studies, symptomatic elbow pain has been reported in 17%–20% of Little League players with more recent evidence suggesting higher incidence of elbow pain in youth players, ranging from 26% to 52%.6–9 At the collegiate level, 9.3% of game injuries and 10.8% of practice injuries are elbow related, and 70.9% of which are related to throwing. 10 In a smaller study, 12% of injuries at the collegiate level account for over 4% of lost game time and is a concern for athletes at higher tiers of competitive sport. 11 Thus, the significance of identifying these injuries and understanding the implications of these conditions in the context of the functional anatomy of the elbow is of importance.
In the overhead throwing motion, the rotating humerus generates significant valgus torque across the elbow which is countered by rapid elbow extension. While the UCL functions as the primary restraint to valgus stress between 30° and 120° of elbow flexion, early cadaveric studies demonstrated that the UCL can withstand a maximal torque of 32.1 ± 9.6 N m.12–17 This implies that other structures surrounding the elbow must contribute to stability during throwing as valgus torque can reach and surpass 64 N m during the late cocking and early acceleration phases.12,13 Medial structures are at risk of failure in tension. 18 Along with increased medial laxity, lateral-sided compression injuries and posterior shear-stress injuries can develop, which represent a constellation of conditions that result from a single pathophysiological mechanism: valgus extension overload.18,19 Presentation of these injuries is largely impacted by an individual athlete’s physiological stage of skeletal maturity with mechanical failures occurring at the weakest link in the chain.14,20,21
Injury to the elbow is examined through an understanding of common medial, lateral, and posterior pathologies. Common medial pathologies such as traction apophysitis of the medial epicondyle, known as Little Leaguer’s elbow, affects approximately 26%–28% of youth baseball pitchers with acute tension failure at the medial apophysis resulting in avulsion of the medial epicondyle.14,18–20 While repetitive overhead activity can lead to osteochondritis dissecans (OCD) of the capitellum on the lateral side, painful persistent olecranon physes and stress fractures have also been reported at all levels of sport, as have olecranon osteophytes and symptomatic intra-articular loose bodies in the posterior compartment.18,19 As the burden of these injuries increase, it is important for orthopedic surgeons to understand the functional anatomy of the elbow, biomechanical forces of overhead throwing, and the surgical techniques available in order to counsel patients and make informed, evidence-based decisions.
This article serves to review the anatomy, biomechanics, pathophysiology, and treatment options for common injuries to the adolescent elbow in overhead athletes. These conditions will be examined in the context of the osseoligamentous development of the elbow, which undergoes significant transformation through adolescence into skeletal maturity. The relevant anatomy will also be described within the context of the biomechanics of throwing, in order to illustrate which conditions may occur based on the physiologic stage of development. Key physical examination and diagnostic findings, as well as approaches to treatment and outcomes reported in the literature will also be discussed. Two of the authors (A.M.L. and P.D.R.) conducted searches of MEDLINE, Embase, and CENTRAL (Cochrane Central Register of Controlled Trials), using the terms “adolescent,” “elbow,” “overhead athlete,” “thrower,” “ulnar collateral ligament NOT thumb,” and “valgus extension overload,” in various combinations with the Boolean operators “AND” and “OR.” A final search was performed on 1 June 2020.
Relevant anatomy
The elbow is a complex joint that allows flexion-extension through the ulnohumeral articulation and pronation-supination through the radiocapitellar articulation. When athletes throw repeatedly at high velocity, repetitive stress can lead to a wide range of overuse injuries, including most commonly that of the UCL.14,22 The UCL is located medially on the elbow and consists of three bundles: anterior, posterior, and transverse (Figure 1).23–27 The anterior bundle serves as the primary restraint to valgus stress during the overhead throwing motion and inserts on a broad footprint on the sublime tubercle of the ulna (Figure 1).14,28 It is further subdivided into anterior and posterior bands, with the anterior band of the anterior bundle maintaining an isometric strain pattern throughout 30°–120°.14,30 The posterior bundle provides secondary restraint to valgus force over 120° and forms the floor of the cubital tunnel, which serves as a conduit for the ulnar nerve as it passes posteriorly to the medial epicondyle. 31 While both the anterior and posterior bundles span the elbow joint, the transverse bundle of the UCL is functionally insignificant with no attachments to the humerus and provides little to no contribution to valgus stability.24–27,32
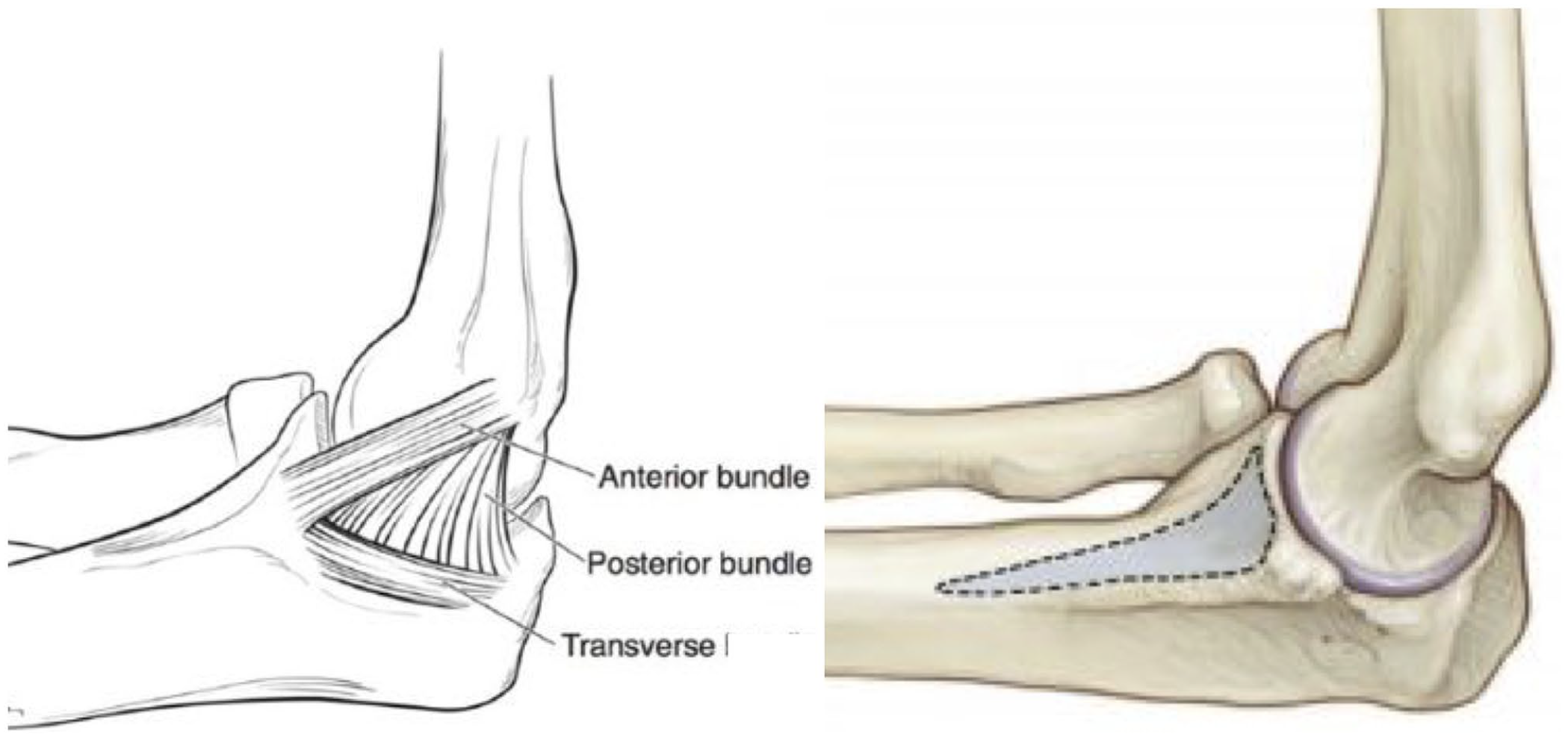
Anatomy of the ulnar collateral ligament (UCL).
The flexor–pronator mass (FPM) muscles also originate from the medial epicondyle of the humerus from two common heads and serve as important secondary stabilizers to the UCL.33,34 The pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), and flexor digitorum superficialis (FDS) originate anterior to the UCL origin, while a portion of the FDS and the flexor carpi ulnaris (FCU) originate posteriorly, providing dynamic restraint to valgus load.33,34 Additional secondary osseous stabilizers include the radiocapitellar articulation laterally and the olecranon and olecranon fossa posteriorly.35,36 The bony congruity of the olecranon and olecranon fossa serve as the primary restraint to valgus stress with the elbow flexed less than 20° and functions to engage fossa around 20° flexion. 37 Failure of these structures to provide valgus stability may lead to repetitive insults at the elbow and subsequently result in injury.
Osseous development
A number of various injury patterns may develop in the adolescent thrower’s elbow depending on an athlete’s stage of osseous development. The elbow develops from six ossification centers, each of which mature and fuse at different rates: the capitellum, the radial head, medial epicondyle, trochlea, olecranon, and the lateral epicondyle. The medial epicondyle apophysis persists the longest in most cases.18–20,38 Although an open physis may remain open up to 20 years of age, the medial epicondyle ossification center fuses around 17 years of age in males (14 years in females), with closure of the medial epicondyle apophysis representing skeletal maturity of the elbow.18,39 In comparison, the olecranon physis closes just before the medial epicondyle around 16 years in males (14 years in females) and is composed of 2 components: a smaller anterior nucleus at the tip of the olecranon and a larger more posterior nucleus that forms the majority of the articular surface.39,40 Laterally, the capitellum typically ossifies around 15 years in males and 13 years in females, while the radial head ossifies around 16 years in males and 14 years in females. 39
Throwing mechanics and pathomechanics
An appreciation of the phases of throwing and the related forces that occur across the elbow is essential to understand how different structures become injured through overuse or poor mechanics. Although the phases of the overhead throwing motion are divided into six phases: windup, early cocking, late cocking, acceleration, deceleration, and follow-through; the late cocking/early acceleration, acceleration, and deceleration phases represent key moments during throwing that are associated with injury (Figure 2).12,13,41 Notably, the late cocking and early acceleration phases of throwing correspond with maximum shoulder external rotation, which generates a large valgus moment across the elbow, resulting in increased tension medially and compression laterally.12,13 During this phase, the medial elbow can experience up to 64 N m torque, exceeding the tensile strength of the UCL, which has been found to be around 22.7–33 N m in cadaveric studies.12–17 In adolescent throwers, the torque generated is typically less—closer to 18–28 N m.16,43 In this population, relative increased laxity demonstrated at the medial UCL and weakness in tension of the apophyseal cartilage are contributing factors to stability with the FPM muscles playing an important role in dynamic stabilization of the elbow.20,31,44–48

Throwing mechanics and pathomechanics diagram.
Timing of acceleration is also significant as this phase occurs between maximum shoulder external rotation and ball release. While rapid extension and pronation result in this phase, shear force of 300 N is produced across the elbow with 500 N of compression across the radiocapitellar joint, which are transmitted through the posterior compartment as the olecranon engages fossa around 20°.12,13 During deceleration, a centripetal force occurs around the elbow, as well as a peak force equal to roughly 90% of body weight that is generated by the flexor-pronators, triceps, and anconeus to counter distraction following ball release to terminal extension.12,13 Collectively, the medial tension, lateral compression, and posterior shear forces generated during overhead throwing are known as valgus extension overload.
Differential diagnosis of elbow pain in the adolescent overhead thrower
When assessing a painful or injured elbow in an adolescent overhead throwing athlete, medial, posterior, and lateral pathologies should be considered, regardless of the primary location of pain, as multiple conditions are often present in the same injured elbow. Moreover, the location of the complaint may not always reveal the location of the pathology. For instance, some athletes with posterior impingement complain of medial pain. 49 In this regard, the differential diagnosis for elbow injuries is wide and a number of conditions should be considered given the varying injury patterns that result from the repetitive stress of the overhead throwing motion and pathologic biomechanics. Lateral pathologies include the presence of radiocapitellar plica that tend to occur in association with OCD lesions that arise from lateral radiocapitellar compression loading forces at the capitellum/radial head. Posterior conditions include persistent olecranon physis and olecranon stress fractures that result from posterior shearing forces when the arm is brought into rapid extension and the follow-through phases of throwing. Posteromedial impingement/symptomatic olecranon osteophytes is also a concern posteriorly with the caveat that presentation is rare prior to exiting adolescence. Medial elbow pathology commonly results with failures in tension, as the medial collateral ligament (MCL) can become attenuated with repetitive strain. Conditions associated on the medial aspect of the elbow include medial epicondylitis, medial epicondyle avulsion fracture, UCL injury, and flexor–pronator injury. In addition, ulnar neuritis is a common condition associated with medial elbow pathology. Loose bodies can occur anywhere in the elbow joint, but most commonly affect the posterior and radiocapitellar compartments with fragmentation.
Lateral elbow pathology
When evaluating for lateral elbow pathology, the key anatomic structures to consider are the capitellum and radial head, which are vulnerable to repetitive compression loading.
Panner’s disease
In younger athletes, the capitellar cartilage of the developing elbow is particularly susceptible to injury through repeated microtrauma, as the capitellar epiphysis blood supply is derived from two to three nutrient vessels functioning as end-arteries that do not communicate with the intramedullary system, which contributes to an age-related injury pattern, as healing potential is limited by tenuous vasculature. 50 In athletes less than the age of 10 years, capitellar osteochondrosis, or “Panner’s Disease,” can develop, which is a distinct entity from OCD. 51 Vague activity-related pain and stiffness are usually the presenting symptom with radiographs showing global fragmentation of the capitellar epiphysis. In most cases, spontaneous regeneration and resolution occur with rest and no surgical intervention is warranted.
OCD
OCDs tend to develop in older athletes than those in whom Panner’s disease occurs—typically between 12 and 17 years of age. 51 OCDs present with insidious onset of poorly localizing functional lateral elbow pain that occurs during throwing and quickly resolves with rest.52,53 Athletes may also complain of mechanical symptoms such as locking or catching in later stages, due to loose body formation in the joint. Examination may reveal lateral tenderness over the capitellum, small effusion, and a 15°–20° flexion contracture in affected athletes. Reproducible symptoms with the active radiocapitellar compression test, which places the affected elbow in extension and elicits lateral compartment pain with forearm pronation and supination, may also be significant (Figure 3). 54 Prompt identification of these findings, especially in the primary care setting, can facilitate appropriate imaging, medical assessment, and surgical intervention in these patients. 55

Radiocapitellar compression test.
In radiographic staging for OCD, Stage 1 refers to a localized flattening and/or radiolucency, Stage 2 refers to a non-displaced fragment, and Stage 3 refers to a displaced fragment; however, X-rays may be falsely normal or understate the degree of injury.56–58 Magnetic resonance imaging (MRI) provides a better characterization of the injury, and will also provide an assessment of other soft tissue structures, such as the UCL or a possible plica. 59 The MRI staging of capitellar OCDs is shown in Figure 4. Indicators of an unstable lesion which will likely require surgery include a high-intensity signal line below the lesion on T2-weighted MRI sequence, a closed capitellar growth plate, range of motion (ROM) restricted >20°, and/or visible fragmentation on ultrasound.53,57

MRI staging of capitellar osteochondritis dissecans.
Non-operative management for OCD consists of 6 months of elbow rest without throwing, non-steroidal anti-inflammatory drugs (NSAIDs), and a hinged elbow brace. 53 Although progressive strengthening and a repeat MRI after 3–6 months for re-evaluation can be considered in some cases, the vast majority of players return to play (RTP) with resolution of pain and demonstrate excellent outcomes when stable OCD lesions are managed conservatively.53,56,60,61 Non-operative management is indicated for small, stable lesions, patients with an open capitellar physis, and those in whom elbow motion is well preserved. 53 Indications for surgery include unstable lesions, mechanical symptoms, symptomatic loose bodies, and failure of conservative management.53,58,62,63 While surgical treatment options are dictated by arthroscopic staging, various surgical modalities to address OCD lesions of the capitellum in the overhead athlete, specifically, minimally invasive arthroscopic-assisted surgery, represent current trends of OCD treatment. Depending on the individual case, cartilage reparative techniques—from debridement and microfracture to fixation, as well as cartilage restoration using osteochondral auto and allograft transplantation can be used to relieve symptoms, return athletes to their sport, and preserve future function of the elbow. 63
Cartilage reparation techniques such as arthroscopic debridement, drilling, abrasion chondroplasty, microfracture, and fixation are viable options for select Capitellar OCD lesions. Drilling is most commonly performed when the subchondral bone fails to heal, but the overlying cartilage is intact. 63 Using Kirschner wires to drill multiple small holes in the subchondral bone, pathways for new blood vessels are created to nourish the affected area and encourage a healing response. 64 In cases where the cartilage is compromised, debridement is often considered, which involves the removal of unstable cartilage and bone via a curette or shaver. 65 Microfracture involves the use of an arthroscopic awl, which is impacted below the level of the subchondral bone and advanced to the minimal depth that allows marrow contents to egress into the lesion. 66 For simple Stage 1 lesions that fail conservative management, drilling or simple debridement is often considered. In the case of Stage 2 or 3 lesions that are less than or equal to 1 cm in diameter and show an intact lateral buttress of capitellar cartilage, microfracture is typically indicated. 66 In comparison, fixation has been achieved in an open or arthroscopic fashion and is considered for lesions that demonstrate displacement of chondral fragments, but that are still intact and robust.63,67 This technique attempts to repair the articular surface using native hyaline tissue with the use of sutures, pins, darts, small anchors, or bone-peg grafts.52,67,68–72
As arthroscopy of the elbow has evolved, it has become the mainstay treatment for OCD and has yielded good short-term outcomes. Rahusen et al. 73 found that 12 of 15 (80%) patients with unstable lesions returned to sports after arthroscopic debridement and abrasion chondroplasty with no reported complications. Clinical outcomes after arthroscopic debridement demonstrated good results, with pain relief during activities of daily living and sport. Although ROM did not improve significantly, the function of the elbow, as reflected by the Modified Andrews Elbow Scoring System (MAESS score), improved from poor to excellent post-operatively. 73 In a study performed by Jones et al., 18 of 21 (86%) patients who underwent arthroscopic management of OCD of the capitellum returned to participate in their sport at their pre-injury level. On average, patients gained 17° of extension and 10° of flexion compared with their pre-operative ROMs. When patients were asked to rate their elbow function using the Single Assessment Numerical Evaluation (SANE) score, the average rating was 87%. 74 Lewine et al. 64 reported outcomes of 21 patients following arthroscopic drilling or microfracture of grade IV capitellar OCD lesions. Although there were no complications in the 21 index procedures, four patients with recurrent loose bodies underwent revision surgery. ROM improved as mean elbow flexion contracture decreased from 15.3° to 3.19° post-operatively and mean elbow flexion increased from 128.3° to 137.1°. Overall, over 86% of patients returned to any sport, while 67% were able to return to their primary sport with reported Timmerman–Andrews (TA) scores improved by a median of 30. 64
In order to preserve native hyaline cartilage and minimize long-term degenerative changes, several studies have depended on the long-used method of fragment fixation, which has produced reliable results and high rates of union.52,71,75 Maruyama et al. 68 observed good clinical outcomes at 2-year follow-up for athletes who underwent bone-peg grafting for grade II lesions, while Uchida et al. reported comparatively good results at 3 years when performing arthroscopic fragment fixation using absorbable thread pins on grade III lesions. 69 In addition, Hennrikus et al. 76 reported good to excellent functional outcomes in the majority of patients undergoing internal fixation of unstable in situ OCD lesions of the capitellum particularly in younger patients with lesions less than 13 mm in sagittal width. While higher levels of evidence are still needed to further investigate optimal surgical treatments of unstable OCD lesions, a systematic review performed by Lu et al. 67 suggested that arthroscopic techniques may be a better option over open procedures with regard to fragment fixation by any method.
Although good short-term outcomes have been obtained with arthroscopic interventions, other treatment modalities have been developed in an effort to improve long-term function. While current marrow stimulation techniques promote the formation of fibrocartilage, Caldwell et al. 77 described a novel arthroscopic approach of debridement and drilling that is augmented with a micronized allogeneic cartilage scaffold to stimulate the formation of more durable hyaline-like cartilage. The addition of a micronized allogeneic cartilage scaffold has been shown to yield higher rates of hyaline cartilage formation in animal studies when compared with microfracture alone, which suggests a viable option for future treatments of unstable OCD lesions.78,79
While treatment modalities such as drilling, debridement, microfracture, and fragment fixation are still largely considered the standard of care for unstable OCD lesions, encouraging evidence suggests that osteochondral autograft transplantation (OAT) and costal osteochondral transplantation procedures can be successful in treating advanced OCD lesions of the capitellum and returning athletes to high-level competition. Compared to other methods, OAT has the distinct advantage of using a patient’s native subchondral bone and articular cartilage to provide mechanical support and an articular surface for the defect.80–82 In a systematic review that specifically looked at RTP after OAT, the authors found over 94% of all patients returned to competitive play without restrictions with a mean of 5.6 months. 83 While Kirsch et al. 83 involved several studies of multiple lesion characteristics and varying surgical techniques and protocols, it demonstrates the current evidence to suggest the efficacy of OATs as a viable treatment modality for unstable OCD lesions (Figure 5). In addition, Nishinaka et al. 85 observed satisfactory results when advanced extensive lesions affecting the lateral wall were treated with costal osteochondral autograft. In this study, 21 out of 22 patients achieved rapid functional improvement and returned to their former sports activity levels with four patients requiring additional minor surgical procedures including screw removal, loose body removal, and debridement. Outcomes for both reparative and restorative techniques for OCD are summarized in Tables 1–3.

Osteochondral autograft transfer (OAT).
Return to play for osteochondritis dissecans (OCD) lesions surgically managed by debridement/abrasion chondroplasty/microfracture.

N: sample size; NR: not reported; ASMI: American Sports Medicine Institute Classification System for Grading OCD Lesions; ICRS: International Cartilage Repair Society Classification System for Grading OCD Lesions; TA score: Timmerman and Andrews Elbow score; MAESS: Modified Andrews Elbow Scoring System; SANE: Single Assessment Numeric Evaluation; DASH: Disabilities of the Arm, Shoulder, and Hand Score; MEPI: Mayo Elbow Performance Index; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room.
Return to play for osteochondritis dissecans (OCD) lesions surgically managed by fragment fixation (any method).

N: sample size; NR: not reported; Minami: Classification System for Capitellar OCD (X-ray); ICRS: International Cartilage Repair Society Classification system for Grading OCD Lesions; TA score: Timmerman and Andrews Elbow score; MEPI: Mayo Elbow Performance Index; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room.
Return to play for osteochondritis dissecans (OCD) lesions surgically managed by OATs/costal osteochondral transplantation procedures.

N: sample size; NR: not reported; ASMI: American Sports Medicine Institute Grading System for OCD Lesions; Nelson: Classification System for Capitellar OCD (MRI); ICRS: International Cartilage Repair Society Grading System for OCD Lesions; JOA Elbow score: Japanese Orthopedic Association Elbow Score; TA score: Timmerman and Andrews Elbow score; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room.
Radiocapitellar plica
Symptomatic radiocapitellar plica can develop when repetitive impingement occurs on a congenitally originated fold. This condition is often associated with capitellar OCD in athletes and presents with lateral clicking, catching, and snapping, as well as a painful click on terminal extension and supination of the forearm. On examination, tenderness over the anconeus soft spot, effusion, and snapping reproduced by the flexion–pronation test by flexing the pronated elbow can be appreciated (Figure 6).101,102 While plain radiographs typically reveal no specific findings, MRI may demonstrate thickened synovial folds ⩾3 mm and hypertrophic folds with irregular or nodular appearance (Figure 7).101,102 Non-operative management typically consists of physical therapy, NSAIDs, activity modification, and intra-articular steroid injections. 101 Patients who fail conservative measures can be treated operatively with arthroscopic resection (Figure 8). 101

The procedure of the posterolateral radiocapitellar plica test.

MRI of radiocapitellar plica (yellow arrow).
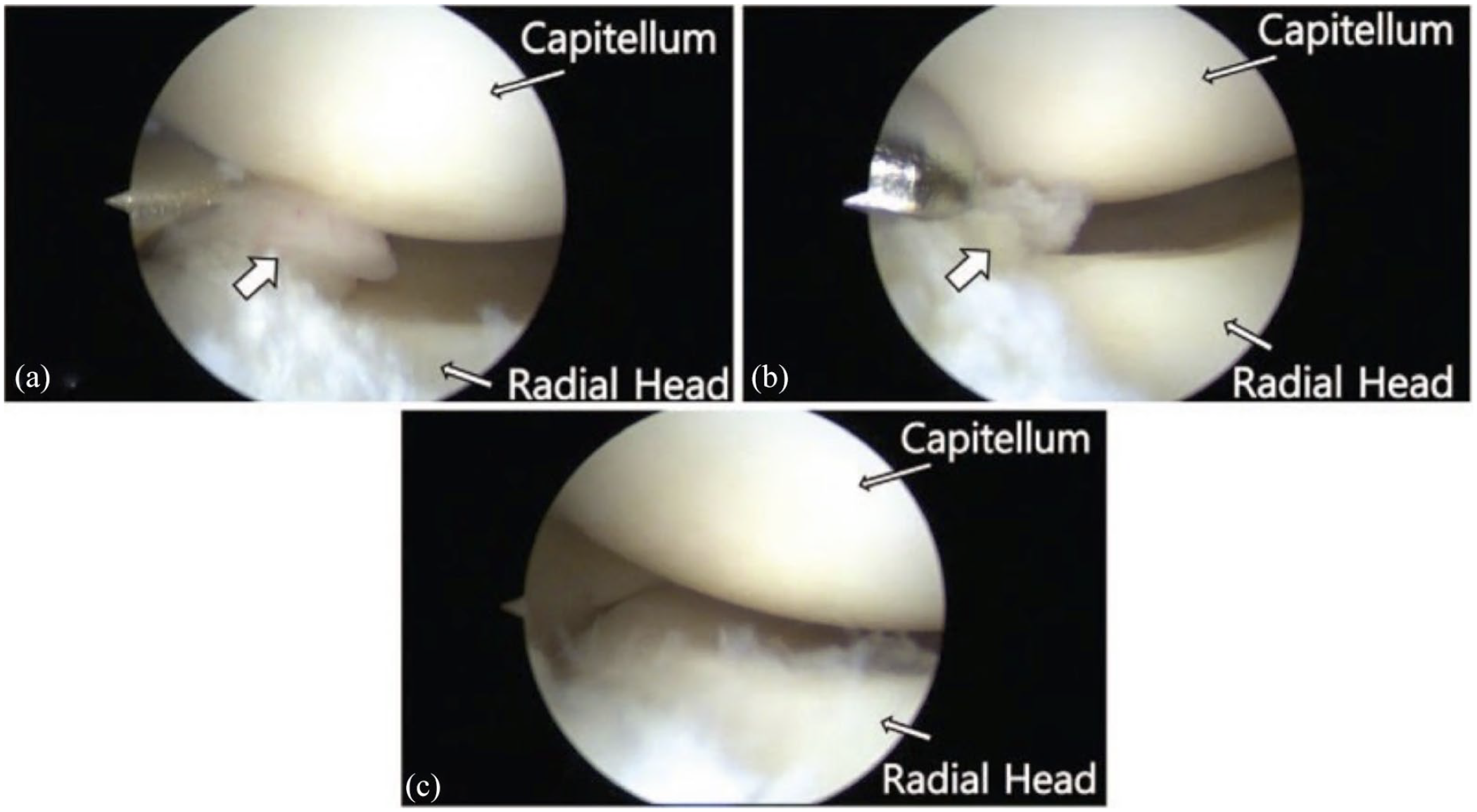
Arthroscopic images of impingement by the posterolateral plica on the radiocapitellar joint (a) thickened and inflamed synovial plica (arrow), (b) arthroscopic debridement of the plica, and (c) radiocapitellar joint after arthroscopic excision.
Posterior elbow pathology
Posterior elbow pathology is related to shear stress across the posterior olecranon as it engages the trochlea and provides increasing restraint to valgus with increasing extension. This contributes to the development of posteromedial osteophytes, olecranon stress fractures, and can also be associated with loose body formation in the context of repetitive microtrauma from the posteromedial olecranon impacting the trochlea. The actual injury pattern is largely a function of patient age and skeletal maturity.
Posteromedial impingement and olecranon osteophytes
Athletes presenting with posteromedial olecranon impingement and olecranon osteophytes usually complain of posteromedial elbow pain during the extension or follow-through phase of throwing, which is often associated with a gradual loss of control, causing throws to miss high.49,105 This condition first described by Wilson et al. in 1983 is the most common elbow injury in adult professional baseball players and usually occurs following maturation through adolescence as valgus extension forces predominate around 18.6 years of age.106–110 Mechanical symptoms such as locking, catching, and/or crepitus that can localize to the posterior elbow are common; however, the presence of severe pain may suggest osteophyte fracture.110,111 On examination, special maneuvers directed at eliciting symptoms of posteromedial impingement include the extension impingement test and the arm bar test. In the extension impingement test, the examiner begins with the elbow slightly flexed and the forearm supinated. The examiner then rapidly extends the elbow while applying a valgus force (Figure 9). If there is worsening of symptoms with applied valgus force, this finding suggests posteromedial osteophytes.49,54 The arm bar test is performed with the patient’s arm in 90° forward flexion and full internal rotation at the shoulder with the elbow extended, while the examiner applies gentle downward hyperextension force on the olecranon (Figure 10). 54 Reproduction of pain and symptoms with these maneuvers is suggestive of posteromedial impingement and olecranon osteophyte formation.54,112 In addition, posteromedial pain and crepitus may be present during the moving valgus stress test. 54
Extension impingement test.
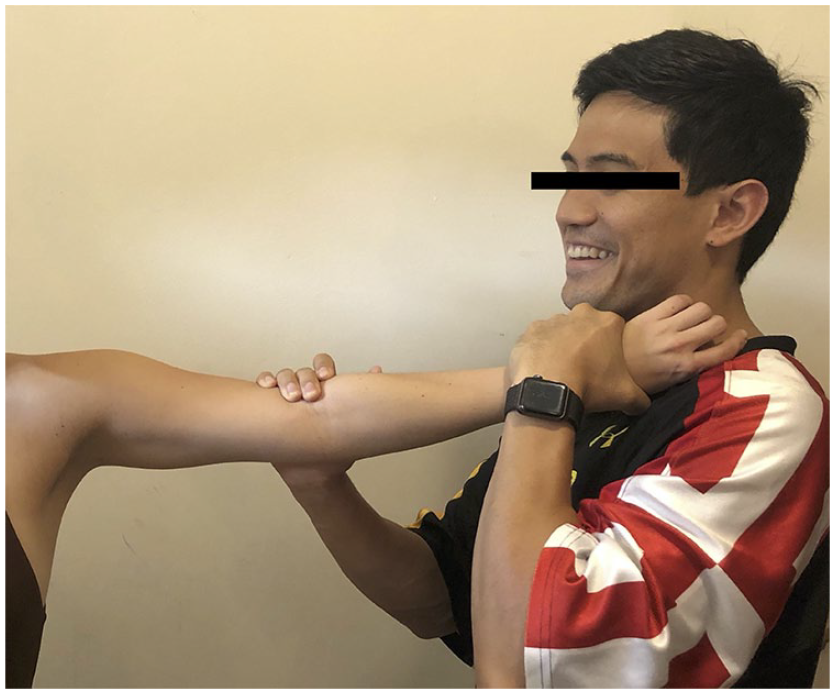
Arm bar test.
On imaging, a posterior osteophyte may be seen on lateral X-ray, while a posteromedial osteophyte may be seen on flexed axial projection. Small osteophytes, however, are best seen on computed tomography (CT; Figure 11).106,111,113–115 The size of the osteophyte does not necessarily correspond with the degree of symptoms, as even very small osteophytes can cause extreme pain and limitation when fractured.
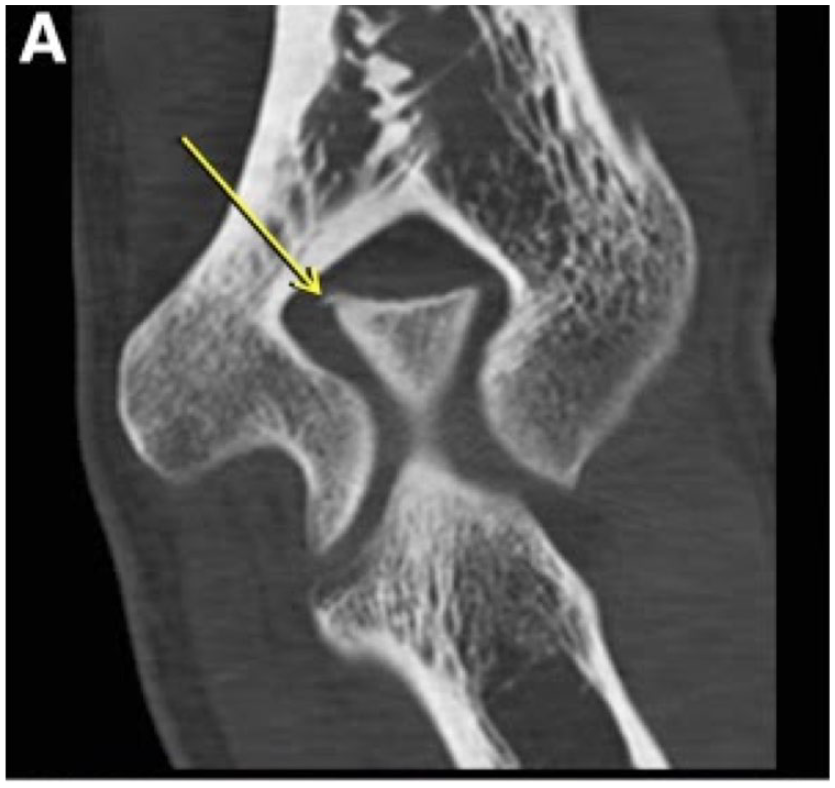
Computed tomography (CT) of small posteromedial osteophyte.
Non-operative management usually involves a combination of rest, throwing restrictions for 2–6 weeks, dynamic stabilization, and eccentric strengthening of flexor-pronators, and is warranted as first-line treatment for most athletes.106–109,115 Surgical management involves osteophyte resection, which can be performed as an open procedure or arthroscopically. When the offending osteophyte is quite small, pre-operative CT can help guide the surgeon to the correct location.49,106–109,115
Elbow arthroscopy has been shown to be a safe and reliable treatment for posteromedial impingement and olecranon osteophytes. Early studies cautioned that operative management targeted at treating secondary effects of UCL insufficiency, such as posteromedial impingement, often led to unsatisfactory results without addressing the underlying UCL. 108 In addition, Reddy et al. 107 reported a larger series in which 187 arthroscopies were reviewed. In this study, the average modified Figgie score increased from 31.2 points to 46.9 post-operatively in professional athletes with 47 out of 55 players (85%) returning to play at the same level or higher. Across several other studies, elbow arthroscopy has yielded excellent RTP and low rates of complications.49,109,116 Outcomes for arthroscopic resection of olecranon osteophytes are described in Table 4.
Outcomes for arthroscopic resection of olecranon osteophytes.

N: sample size; NR: not reported; Modified Figgie score: Outcome Measure to Evaluate Elbow Function; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room; UNT: ulnar nerve transposition; UCL: ulnar collateral ligament; ORIF: open reduction and internal fixation.
Olecranon stress fractures and persistent olecranon physis
Olecranon stress fractures and persistent olecranon physis can lead to loss of extension strength and ROM, as well as posterior elbow pain, especially during terminal elbow extension and follow-through. In addition to pain reproduced on resisted elbow extension, patients may also have a positive arm bar test and tenderness in the region of physis.
Five patterns for olecranon stress fracture have been identified based on a combination of X-ray, CT, and MRI findings: (1) physeal, (2) transitional, (3) classic, (4) sclerotic, and (5) distal. 110 Younger athletes tend to develop the physeal type injury, while the transitional type occurs in the intermittent age range. In contrast, older athletes with skeletally mature olecranons tend to develop the classic type.
Triceps traction and extension forces typically predominate at an average of 14.1 years of age, which can lead to a transverse pattern of injury and the formation of posterior tip osteophytes. 110 By comparison, valgus extension forces predominate around 18.6 years of age, which allow for the development of an oblique pattern of injury and may present with posteromedial osteophytes and/or an oblique stress fracture following the transitional phase. 110 Physeal type stress fractures can be further divided into four stages based on imaging (Figure 12). 110
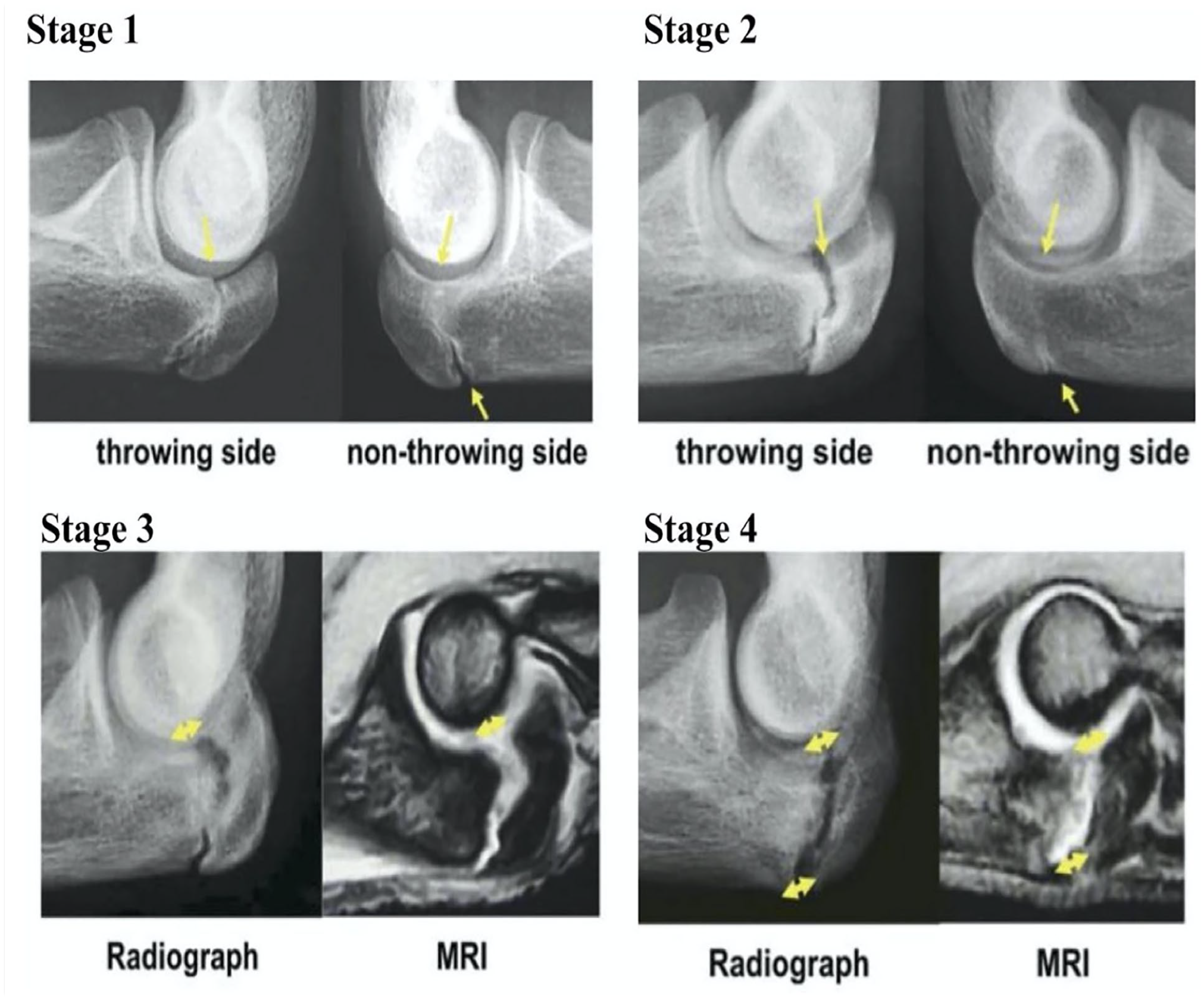
Four stages of physeal type stress fracture based on imaging.
A trial of non-operative management for 3–4 months is warranted in most cases, although schlerotic types may be more likely to fail non-operative management. Contralateral elbow radiographs to determine evidence of persistent physis, delayed closure, and widening are diagnostic. Non-operative management (rest, cessation of throwing, NSAIDs) is initially indicated for most cases.110,117 When surgical intervention is warranted, internal fixation, typically with a cannulated screw or intramedullary screw, affords reliable results with resolution of symptoms and high rates of RTP within less than a year.40,110,116,118–123 Although less common, tension band constructs have also been implemented, but have been associated with a higher rate of symptomatic hardware and subsequent hardware removal. 124 Outcomes for operative management of olecranon stress fractures are summarized in Table 5.
Outcomes for operative management of olecranon stress fractures.

N: sample size; NR: not reported; TB: tension band; DASH: Disabilities of the Arm, Shoulder, and Hand Score; MEPI: Mayo Elbow Performance Index; ASES score: The American Shoulder and Elbow Surgeons Score; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room; ORIF: open reduction and internal fixation.
Medial elbow pathology
During the overhead throwing motion, the medial epicondylar apophysis represents the weakest link in the kinetic chain with injury resulting from failures in tension. Structurally, the FPM muscles and the UCL have a shared origin at the medial epicondylar apophysis with greater contributions of pulling forces from the FPM in younger athletes. 21
Depending on an athlete’s age and the maturity of the medial epicondylar apophysis, patterns of injury may vary. For instance, failure of the weak apophyseal cartilage may result in avulsion fractures in younger athletes, while UCL tears tend to occur after physeal closure.14,18–20 While studies have demonstrated the tensile strength of the UCL to be 22.7–33 N m in cadavers,14,16,17,34 maximum valgus torque in adolescent athletes reaches 18–28 N m16,43 and can exceed 120 N m in professional athletes. 128 These findings highlight the greater role of the FPM20,31,44–46 to facilitate offset discrepancies and serve as a dynamic stabilizer in the context of relative laxity of the UCL in younger athletes.47,48
In most cases, athletes who suffer a medial epicondylar fracture usually present with a history of medial elbow pain during the acceleration (85%) and deceleration (25%) phases, a sudden pain or “pop” while throwing, and/or decreased control or difficulty throwing hard or far distances. 58 Examination will usually reveal point tenderness to bony palpation of the medial epicondyle, medial swelling with a possible effusion, and valgus instability. 58 Typically, a fractured medial epicondyle is diagnosed on plain radiographs, but the true displacement may be underestimated if relying exclusively on anterior–posterior (AP) and lateral projections.58,129,130 Other views, such as the internal oblique and distal humerus axial views, can be useful in this regard; however, three-dimensional CT is the most accurate method to assess true displacement.129,130 In terms of conservative management, long-arm casting for 4 weeks followed by strengthening and progressive return to sport (RTS) is indicated if a patient suffers a fracture with minimal displacement (<5 mm) and exhibits no laxity/instability on physical exam.129,131,132 In contrast, operative fixation of medial epicondyle fractures is generally recommended for fragment displacement over 5 mm and significant laxity or instability, as well as evidence of fragment incarceration in the elbow joint.129,131,132 To assist with reduction during open reduction and internal fixation (ORIF), the wrist is fully flexed, the forearm is supinated, the elbow flexed to 90°, and Esmarch is applied distally to proximally. 129 These maneuvers allow the fragments to be milked proximally and restore the defect to its anatomic position.
The optimal treatment for medial epicondylar fractures remains unclear; however, successful RTP can be achieved using published treatment algorithms. In a study of eight skeletally immature baseball players, five of eight players had 5 mm or less of displacement and were selected for non-operative treatment, while three of eight players had more than 5 mm of displacement and underwent ORIF. All eight players returned to play in less than a year with an average time of 7.6 months. 131 Similarly, Lawrence et al. 132 demonstrated excellent outcomes in 14 pediatric overhead athletes who suffered medial epicondyle fractures. Eight patients were treated operatively and six patients were managed non-operatively. Excellent DASH (Disabilities of the Arm, Shoulder, and Hand) scores were achieved in both groups and all overhead athletes were able to return to their sport at the next appropriate level. 132 Despite the conflicting literature in regard to the optimal treatment of medial epicondyle fractures, other studies have found no statistically significant difference in outcomes or complications between operative and non-operatively treated moderately displaced medial epicondyle fractures in adolescent upper-extremity athletes. 133 Outcomes for operative versus non-operative management for medial epicondyle fractures are summarized in Table 6.
Outcomes for operative versus non-operative management for medial epicondyle fractures.

N: sample size; NR: not reported; DASH: Disabilities of the Arm, Shoulder, and Hand Score; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room.
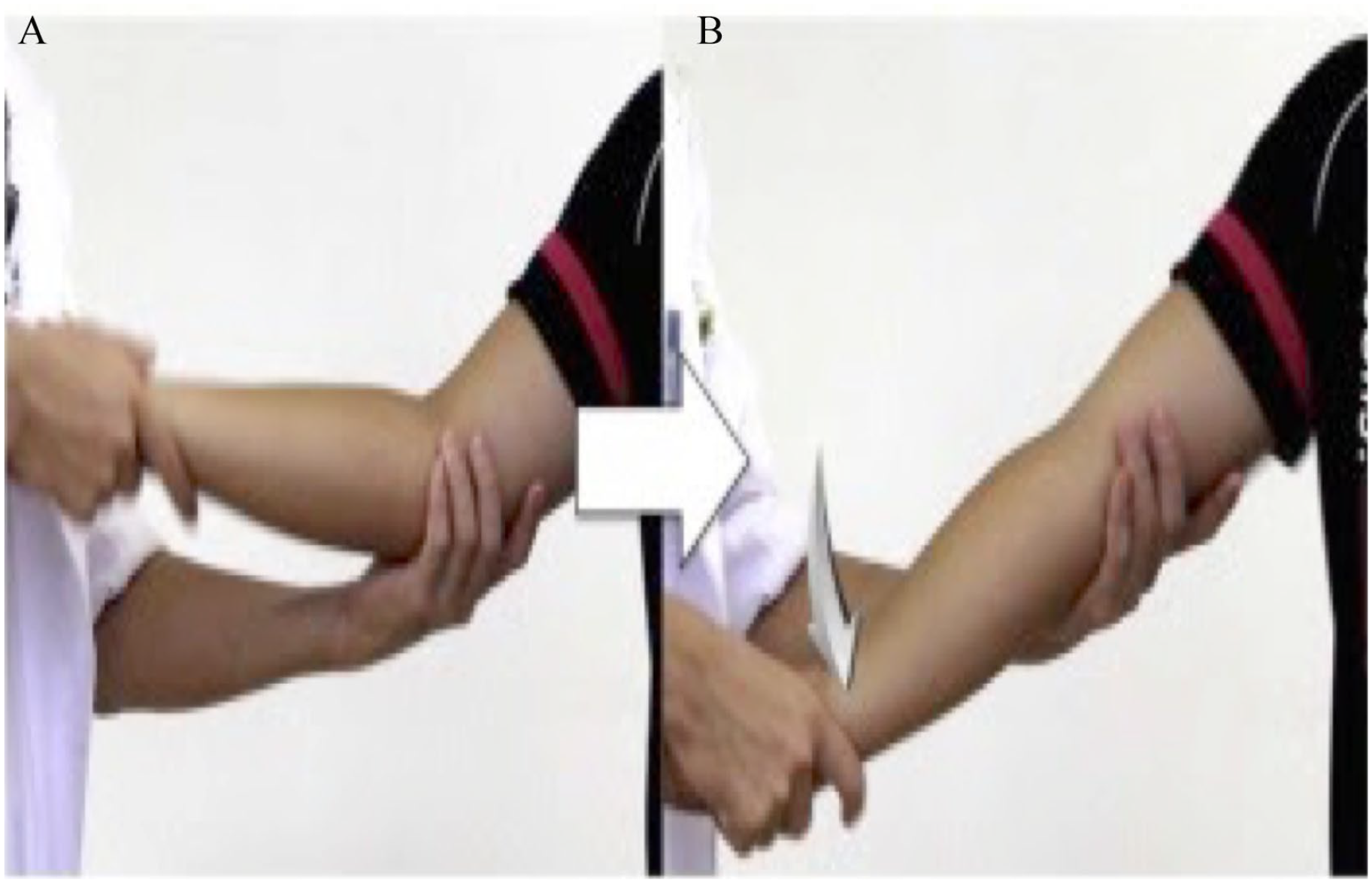
An acute UCL rupture presents with a sudden pain or pop during one throwing motion, which leaves the athlete debilitated and unable to continue throwing. This injury is relatively more common in younger athletes and may be associated with possible ulnar paresthesias.14,44 In addition, UCL rupture can result from chronic injury with pain during the acceleration phase, which is associated with loss of ball control, reduced velocity, and/or increased fatigability. 105 On examination, special maneuvers including the valgus stress test, the milking maneuver, and the moving valgus stress test can be performed to assess the elbow. 54 The classic valgus stress test assesses the anterior band of the UCL anterior bundle by stabilizing the humerus at 30° of elbow flexion to unlock the bony restraint of the olecranon from the fossa and applying a valgus stress. 134 The milking maneuver assesses the posterior band of the UCL anterior bundle by flexing the elbow 90°, grabbing the affected thumb with the opposite hand passed under the affected arm, and pulling to stress the medial elbow (Figure 13).135,136

Milking maneuver.
The moving valgus stress test can also be performed, which has the highest sensitivity (100%) and specificity (73%) for UCL injury (Figure 14). 137 In the moving valgus test, the shoulder is placed in abduction and external rotation while the examiner holds the thumb with one hand and supports the elbow with the other. The elbow is gently flexed and extended while applying a valgus stress, with a positive test eliciting pain at the arc of motion between 80° and 120°. 138

Moving valgus stress test (a) examiner places valgus stress with elbow at 90° of flexion and (b) elbow is quickly extended to approximately 30° with continuous valgus stress.
On imaging, X-rays should confirm a skeletally mature medial elbow, as cartilaginous apophysis fails before the UCL. MRI or CT arthrogram may also reveal lateral bony edema, as well as a “T sign” (Figure 15), which represents partial tearing off the ulnar insertion. 139 While MRI remains the gold standard, the accuracy of MRI in the evaluation of subtle UCL injuries and the utility of arthrography and contrast remain controversial.114,139–142

Coronal image of “T sign” representing UCL rupture. Patient consent was obtained for permission to use this image.
For partial UCL tears, non-operative management is attempted, which typically consists of rest from throwing, a hinged elbow brace restricting full extension, NSAIDs, and physical therapy with graduated throwing once pain free. 117 Rehabilitation of the elbow, whether following immediate injury or post-surgical, generally follows a progressive and sequential order, consisting of a 3-month course divided into four phases: (1) immediate motion, (2) intermediate, (3) advanced strengthening, and (4) return to activity. 117 In the immediate motion phase of rehabilitation, ROM is initially permitted in a non-painful arc of motion, usually from 10° to 100°, to decrease inflammation and align collagen tissue. In addition, a brace is prescribed to restrict motion; isometric exercises are performed to prevent atrophy; and NSAIDs are prescribed to control pain and inflammation. In the intermediate phase, ROM is gradually increased by 5°–10° per week as tolerated with the goal of advancing to the strengthening phase, where isotonic strengthening and plyometric exercises are slowly initiated. These exercises eventually progress to an interval return to throwing, as the athlete regains full ROM, adequate elbow strength, and dynamic stability for RTS. 117 Operative management is usually considered if symptoms continue to persist.
Although studies suggest over 42% of UCL ruptures reach full recovery without surgical intervention, it is still unclear how to predict these outcomes in certain athletes. With regard to reconstruction, multiple techniques including interference screws are used today, in addition to the most commonly performed modified Jobe (figure-of-8) and docking techniques. Although the modified Jobe has long been considered the gold standard in reconstruction, multiple systematic reviews have suggested that the docking technique is associated with fewer complications and higher RTP rates.143–146 Looney et al., 147 however, observed that a number of these systematic reviews often included studies in which the classic Jobe technique was utilized. In Dr Jobe’s original description in 1974, the FPM was detached to access the medial elbow, and a submuscular ulnar nerve transposition was routinely performed to protect the ulnar nerve, as the humeral tunnels were directed posteriorly toward the cubital tunnel. 148 Since then, three significant modifications have been made to the original technique including (1) the development of approaches that preserve the FPM and decrease morbidity associated with detachment; (2) submuscular ulnar nerve transposition was abandoned in favor of subcutaneous transposition; and (3) the humeral tunnels were directed anteriorly, to prevent iatrogenic injury to the ulnar nerve.108,147,149,150 Together, these changes are commonly referred to as the modified Jobe technique. These discrepancies are important to consider, as Looney et al. 147 found that there is no significant difference in outcomes between the docking and figure-of-8 techniques with regard to the Conway Scale rating or RTP time, when modern muscle sparing techniques are utilized and submuscular ulnar nerve transposition is avoided.
Although reconstruction has been the mainstay of surgical management of UCL injuries, renewed interest in repair techniques despite initial poor reported outcomes have resurfaced given a stronger understanding of the indications and limitations associated with the procedure. In addition, excellent clinical outcomes have been observed with the advent of implementing internal brace with repair of the UCL. Typically, the best candidates for the procedure are younger patients with an acute UCL tear as this population tends to lack the degenerative component seen in older athletes. While no clinical studies have been conducted comparing the outcomes of repair with internal brace versus reconstruction in adolescent athletes, Bodendorfer et al. 151 observed no significant differences in valgus gapping under cyclic fatigue testing when specimen repair with an internal brace construct was compared to specimen treated with docking reconstruction, or when either was compared to elbows with intact ligaments. Jones et al. 152 reported similar results when comparing specimen repaired with internal brace with specimen reconstructed with the modified Jobe technique. Recently, Wilson et al. 153 reported one case of a collegiate football athlete who suffered a complete tear of the UCL and was treated with primary UCL repair with internal brace and achieved excellent recovery with RTS at 3 months. This case also demonstrated excellent elbow function and RTP at the same level 5 years later. 153 While the evidence regarding clinical outcomes is sparse, repair techniques with internal brace are promising and continue to gain popularity. 154 Study outcomes of reconstruction and repair techniques for UCL rupture are summarized in Tables 7–9.
Outcomes for UCL reconstruction with modified Jobe technique.

N: sample size; NR: not reported; DASH: Disabilities of the Arm, Shoulder, and Hand; KJOC: Kerlan–Jobe Orthopedic Clinic Shoulder and Elbow score; TA score: Timmerman and Andrews Elbow score; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room.
Outcomes for UCL reconstruction with docking technique.

N: sample size; NR: not reported; KJOC: Kerlan–Jobe Orthopedic Clinic Shoulder and Elbow score; TA score: Timmerman and Andrews Elbow score; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room; UNT: ulnar nerve transposition.
Outcomes for UCL repair techniques.

N: sample size; NR: not reported; KJOC: Kerlan–Jobe Orthopedic Clinic Shoulder and Elbow score; RTP: return to play; RTP SL/H: return to play at the same level or higher; RTP time: return to play time (reported in months); RTOR: return to operating room; UNT: ulnar nerve transposition.
Other notable conditions including ulnar neuritis, or cubital tunnel syndrome, medial epicondyle apophysis, and flexor–pronator strain or rupture are important to consider when evaluating adolescent overhead throwing athletes for medial pathology. In cubital tunnel syndrome, a chronic traction injury results from elongation of medial structures, which is present in 40% of cases of UCL injury along with symptomatic subluxation.14,45 A positive Tinel’s test over the cubital tunnel and/or palpable subluxation is usually appropriate for diagnosis, with treatment involving transposition, especially at the time of UCL surgery if pre-operative symptoms are present.170,171 In comparison, flexor–pronator strain is uncommon in younger athletes and presents with pain exacerbated at the muscular origin of the medial epicondyle on resisted wrist flexion.14,45 Finally, chronic overuse syndrome from repetitive traction to the medial apophysis can develop.14,45 X-rays may reveal slight widening of apophysis and/or fragmentation of the ossification center, which represent accelerated growth and gradual deformity with chronicity that is easily detected on MRI. 14 Treatment consists of rest with position change for 4–6 weeks, usually followed by a strengthening program. 54
Conclusion
Increased single-sport specialization by younger athletes may be leading to a rise in elbow injuries. With an increased prevalence of injuries, a comprehensive understanding of the diagnosis and management of common elbow injuries in the context of functional anatomy and varying states of skeletal maturity is of increased importance. While the UCL is the primary valgus stabilizer in the elbow between 30° and 120° of flexion, other structures, such as the FPM, the radiocapitellar articulation, and the olecranon, all contribute to the ability to withstand the significant and abrupt valgus force that is placed on the medial elbow during the late cocking and early acceleration phases of the throwing motion.
Depending on an athlete’s stage of skeletal maturity, a wide range of injuries that arise from failures in medial tension, lateral-sided compression loading, and posterior extension shear-stress can develop in adolescent throwers. When considering lateral pathology of the elbow, conditions such as Panner’s disease, OCD, and radiocapitellar plica can develop. Excellent outcomes with non-operative and surgical management of these conditions have been reported, along with the emergence of varied techniques and novel approaches for improved long-term function. In the posterior compartment, posteromedial impingement and olecranon osteophytes, olecranon stress fractures, and persistent olecranon physis or loose bodies may also pose a concern. While there is an increased burden of olecranon stress fractures and persistent olecranon physis in younger athletes, both conservative and operative management with internal fixation has resulted in excellent clinical outcomes with high RTP rates when appropriately indicated. Generally, symptomatic hardware and recurrence are common complications with some studies reporting cases of infection and ulnar nerve impingement. Depending on an athlete’s phase of osseous development, failure in medial tension at the elbow can also manifest. While weakness in apophyseal cartilage may lead to medial epicondyle avulsion fractures, UCL tears can develop in athletes that have reached skeletal maturity. Although there is evidence to suggest good clinical outcomes with non-operative management, no consensus has been made to anticipate which individuals will see spontaneous recovery from their injuries.
The main limitations to this review relate to the sample sizes and study designs of the included studies. While an exhaustive review was performed to evaluate the outcomes following surgical management of OCD lesions using varied techniques, arthroscopic resection of olecranon osteophytes, internal fixation of olecranon stress fractures, operative versus non-operative management of medial epicondyle fractures, and the surgical management of UCL rupture using reconstruction versus repair techniques, the assessment of RTP are limited given the variability of surgical technique employed across several studies, non-standardized post-operative rehabilitation protocols, and varying outcome measures. Furthermore, the majority of the studies included baseball players, which may limit the generalizability of these results to other athletes, such as javelin throwers or football players, who may experience varied loading to the elbow given different modes of competitive play. In addition, discrepancies in surgical management, such as varied operative technique and approach, as well as non-standardized post-surgical rehabilitation may have influenced outcome measures and RTP rates. Given the significant heterogeneity and small samples across several studies, there is a high risk of available bias regarding the overall evidence from this review. Higher levels of evidence are required to determine a true estimate of RTP for the management of these injury patterns.
Overall, with sound clinical judgment and operative technique, excellent clinical outcomes with high RTP rates can be obtained in the setting of elbow injury in the adolescent throwing athlete. Future directions for research should consider the need to define treatment algorithms, improve clinical outcomes, and contribute to a limited pool of data that compares the efficacy of varied surgical techniques and approaches.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.