
Abstract
Acute myocarditis is a rare complication of Escherichia coli urinary tract infection and sepsis. We report the case of a previously healthy 55-year-old female who presented to our emergency department with diarrhea and hypotension. The basic metabolic panel results showed an increase in inflammatory markers and an acute kidney injury. Urine and blood cultures grew Escherichia coli. The patient subsequently developed sudden chest pain and shortness of breath, diffuse ST-segment elevation, and cardiac enzymes’ elevation. Coronary angiogram was normal, and transthoracic echocardiogram demonstrated normal ventricular functions. Cardiac magnetic resonance imaging was highly suspicious of myopericarditis. The patient made a full recovery after infection treatment with intravenous antibiotics, aspirin, and colchicine.
Introduction
Bacteremia due to Escherichia coli sepsis is a significant problem in both hospital- and community-acquired infections. 1 E. coli is a common pathogen causing urinary, respiratory, and gastrointestinal tract infections; however, myocarditis is an uncommon complication of E. coli sepsis, with only a few cases reported in the literature.2–4 We present a case of bacterial myocarditis following E. coli urosepsis in a previously healthy patient. A high index of suspicion is needed to diagnose bacterial myopericarditis, with supportive biochemical, electrocardiogram (ECG), and cardiac magnetic resonance imaging (CMRI) findings.
Case presentation
A previously healthy 55-year-old female presented to our emergency department with 2-day history of severe, non-bloody, watery diarrhea associated with crampy abdominal pain. On examination, she was afebrile with a temperature of 36.5°C, heart rate of 95 beats per minute, and respiratory rate of 22 breaths per minute. She was hypotensive with a blood pressure of 86/47 mm Hg. Her abdomen was soft, with generalized tenderness, and cardiovascular and chest examinations were unremarkable. Laboratory values showed leukocytosis with a white blood cell (WBC) of 21.2 × 109/L (4.5–11 × 109/L), neutrophils of 19.44 × 109/L (1.8–7.7 × 109/L), high C-reactive protein of 262.69 mg/L (⩽5 mg/L), elevated creatinine of 256 µmol/L (44–80 µmol/L), urea of 14.50 mmol/L (2.8–8.1 mmol/L), and lactate of 2.65 mmol/L (⩽2.2 mmol/L). ECG done on admission showed normal sinus rhythm. The initial diagnosis was sepsis secondary to severe Clostridium difficile infection. The patient’s blood pressure improved after resuscitation with 2 L of normal saline and was empirically initiated on oral vancomycin 125 mg four times a day and intravenous (IV) metronidazole 500 mg every 8 h. Blood, urine, and stool cultures and stool for C. difficile were collected.
The following morning, the patient spiked a temperature of 38.6°C associated with rigors and shortness of breath with a respiratory rate of 30 breaths per minute and oxygen saturation of 89%. Chest auscultation revealed bilateral crepitations, and the cardiovascular examination was unremarkable with no jugular venous distention. Chest X-ray showed pulmonary edema, ECG showed sinus tachycardia, and brain natriuretic peptide was 6217.0 ng/L (⩽287 ng/L). The patient was placed on Bilevel Positive Airway Pressure (BiPAP) and received one dose of furosemide 80 mg IV due to pulmonary edema and respiratory distress. Blood and urine cultures grew E. coli, and stool culture was negative for C. difficile. Oral vancomycin and IV metronidazole were discontinued, and the patient was started empirically on a renally adjusted dose of ertapenem and received a single dose of amikacin 500 mg. Due to the sudden development of pulmonary edema, a transthoracic echocardiogram was done, which showed normal sizes of the left and right ventricles with normal global systolic and diastolic functions and minimal pericardial effusion.
The patient developed acute central chest pain 2 days post-admission, with diffuse ST-segment elevation (Figure 1), and a troponin T level of 0.791 µg/L (⩽0.014 µg/L), which raised a concern for acute ST-elevation myocardial infarction. The patient received a loading dose of aspirin (300 mg) and ticagrelor (360 mg) and underwent a coronary angiogram, which showed normal coronaries.

A 12-lead ECG showing diffuse ST-segment elevation.
A cardiac magnetic resonance imaging (CMRI) was suggested to rule out myopericarditis but was deferred due to the patient’s acute kidney injury. Over the course of the week, the patient’s condition improved with resolution of fever, dyspnea, and improvement in inflammatory markers and renal function. No inotropes were used as the patient continued to be hemodynamically stable. Antibiotics susceptibility showed pan-sensitive E. coli and ertapenem was de-escalated to augmentin. The patient underwent a CMRI after normalization of her renal functions, which revealed evidence of myocardial edema in the left lateral ventricular wall, presence of subepicardial late gadolinium enhancement (LGE) in the mediolateral left ventricular wall, and presence of pericardial uptake of contrast, which were all highly suggestive of inflammation involving the myocardium and pericardium (Figure 2).
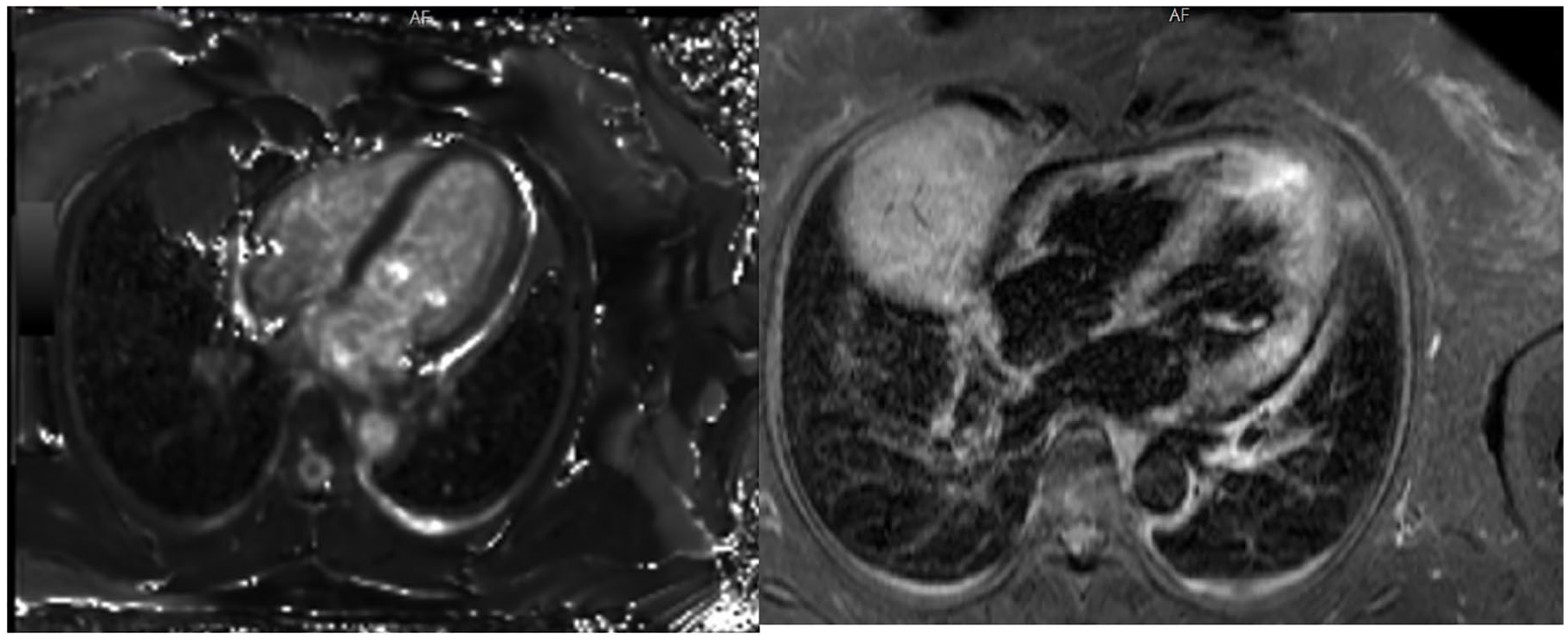
CMRI findings that are highly suggestive of inflammation involving the myocardium and pericardium.
The patient was discharged on the 8th day of admission after making a complete recovery, with a 2-week tapering dose of aspirin and a 3-month prescription for colchicine as a treatment for acute pericarditis. On follow-up 1-week post-discharge, the patient continued to do well with no recurrence of symptoms.
Discussion
Myopericarditis is a rare complication of E. coli urosepsis, with only a few cases reported in the literature.2–4 Infectious myocarditis is most commonly caused by viruses such as enteroviruses, including coxsackie A, coxsackie B, echoviruses, adenoviruses, and parvovirus B19. With the exception of Mycobacterium tuberculosis, bacterial pathogens rarely cause myopericarditis. 5 The exact mechanism by which E. coli can cause myopericarditis is unclear but is likely a combination of direct bacterial invasion due to fimbriae presence, which facilitates adherence and local inflammation, and lipopolysaccharides (LPS), which are found on gram-negative bacteria’s outer membrane, including E. coli. LPS can bind with Toll-like receptor 4 (TLR4) during bacteremia leading to a systemic inflammatory response.6,7
In an experiment done on mice mimicking septic shock, cardiomyocytes, which express TLR4 on their membranes, showed cardiac dysfunction after injection of LPS intraperitoneally. This interaction resulted in the production of proinflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin-1β (IL-1β) that led to local inflammation and contractile dysfunction. 6
Our patient had sepsis secondary to E. coli urinary tract infection and subsequently developed chest pain with ST-elevation on ECG, with normal coronaries and a CMRI suggestive of myopericarditis. The whole picture was suggestive of E. coli myopericarditis. A definitive diagnosis of E. coli myocarditis would require an endomyocardial biopsy to show morphological evidence of inflammation with bacterial invasion and positive tissue culture.3,8 However, its highly invasive nature and low sensitivity render it impractical and of low utility in clinical practice.
Myocarditis can have a wide range of clinical presentations, including chest pain, palpitations, dyspnea, and heart failure symptoms. A constellation of a typical clinical presentation of chest pain, with diffuse ST-segment elevation and PR-segment depression on ECG, elevation in inflammatory markers, and a normal coronary angiogram, often helps in making the diagnosis of myopericarditis. CMRI is a useful noninvasive imaging modality in identifying myocardial and pericardial disease.2,9
There are no specific guidelines for managing bacterial myopericarditis. Management of bacterial myopericarditis requires specific and appropriate management of the bacterial pathogen and sepsis, as well as supportive measures with the use of non-steroidal anti-inflammatory medications to reduce inflammation and control pain. 8
Conclusion
Myocarditis represents a rare complication of E. coli sepsis. Following an acute bacterial infection, symptoms and signs of myocarditis should prompt the physician to investigate for possible bacterial myocarditis. CMRI represents a reliable and noninvasive approach for diagnosis. The mainstay of managing bacterial myocarditis is proper management of the infection, alongside anti-inflammatories for myopericarditis.
Footnotes
Acknowledgements
The authors thank Dr. Jassin Hamed for his clinical assistance in managing the patient. They also thank Heart and Vascular Institute at Sheikh Khalifa Medical City for performing and providing the coronary angiogram images, and Radiology Department at Sheikh Khalifa Medical City for reporting the cardiac magnetic resonance imaging (CMRI) and providing the images.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Institutional Review Board at Sheikh Khalifa Medical City. Reference No. 07.12.2020 [RS-650].
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Patient’s written consent has been obtained before writing and submitting this manuscript.