
Abstract
Background:
Endomyocardial biopsy is considered as the gold standard in patients with suspected myocarditis. We aimed to evaluate the impact of bioptic findings on prediction of successful return to work.
Methods:
In 1153 patients (48.9 ± 12.4 years, 66.2% male), who were hospitalized due to symptoms of left heart failure between 2005 and 2012, an endomyocardial biopsy was performed. Routine clinical and laboratory data, sociodemographic parameters, and noninvasive and invasive cardiac variables including endomyocardial biopsy were registered. Data were linked with return to work data from the German statutory pension insurance program and analyzed by Cox regression.
Results:
A total of 220 patients had a complete data set of hospital and insurance information. Three quarters of patients were virus-positive (54.2% parvovirus B19, other or mixed infection 16.7%). Mean invasive left ventricular ejection fraction was 47.1% ± 18.6% (left ventricular ejection fraction <45% in 46.3%). Return to work was achieved after a mean interval of 168.8 ± 347.7 days in 220 patients (after 6, 12, and 24 months in 61.3%, 72.2%, and 76.4%). In multivariate regression analysis, only age (per 10 years, hazard ratio, 1.27; 95% confidence interval, 1.10–1.46; p = 0.001) and left ventricular ejection fraction (per 5% increase, hazard ratio, 1.07; 95% confidence interval, 1.03–1.12; p = 0.002) were associated with increased, elevated work intensity (heavy vs light, congestive heart failure, 0.58; 95% confidence interval, 0.34–0.99; p < 0.049) with decreased probability of return to work. None of the endomyocardial biopsy–derived parameters was significantly associated with return to work in the total group as well as in the subgroup of patients with biopsy-proven myocarditis.
Conclusion:
Added to established predictors, bioptic data demonstrated no additional impact for return to work probability. Thus, socio-medical evaluation of patients with suspected myocarditis furthermore remains an individually oriented process based primarily on clinical and functional parameters.
Introduction
Systolic heart failure in young patients is predominantly caused by viral myocarditis. Myocarditis is characterized by a broad clinical spectrum and variable acute presentation from fulminant myocarditis with cardiogenic shock to oligosymptomatic abortive forms. 1 Due to silent courses, the prevalence remains unclear, and postmortem data of sudden cardiac death patients demonstrated a viral myocarditis in 8.6%–12%.2,3 While viral myocarditis is the most common genesis, there are various other pathogenetic causes. 4
A reliable classification of myocarditis can be performed by endomyocardial biopsy (EMB) with histological, immuno-histochemical, and molecular genetic examination. 5 Beside cardiac magnetic resonance imaging, EMB has been considered the gold standard technique for diagnosis of myocarditis. EMB data are essential tools for selecting treatment strategies including conventional heart failure medication as well as specific antiviral and immunomodulating therapy (immunoadsorption therapy, immunoglobulins, interferon-β (IFN-β)).6,7 In experienced centers, the complication rate of EMB is low with 0.12%. 8
Although there are numerous evidence-based recommendations for athletes with cardiomyopathies and myocarditis,9–11 data regarding return to work (RTW) and recommendations for leisure time activity in non-athletes are rare. 12 Recent statement papers do not affect the social-medical aspect of occupational reintegration.13,14 Routinely physicians judge according to the acute clinical presentation, remaining left ventricular function after clinical recovery, and rhythm stability; nevertheless, these decisions are not based on evidence.
We aimed to investigate whether EMB data added to conventional clinical parameters have an independent predictive impact on RTW probability as a risk stratification tool. Thus, an accurate identification of vulnerable patients and their socio-medical management including appropriately tailor reintegration strategies based on objective pathogenetic conditions could be performed.
Methods
In 1153 patients (48.9 ± 12.4 years, 66.2% male) at working age (below 65 years) who were hospitalized between 2005 and 2012 in the Department of Cardiology and Pneumology, Medical Clinic II, Charité University of Berlin due to symptoms of heart failure, an EMB was performed. All patients were included in the data base of the Collaborative Research Centre Transregio 19 (CRC TR 19) “Inflammatory Cardiomyopathy—Molecular Pathogenesis and Therapy.” Routine clinical and laboratory data and sociodemographic parameters as well as medication and comorbidities were documented. In all patients, a two-dimensional transthoracic echocardiogram including tissue Doppler ultrasound was performed. If possible, patients underwent exercise function testing (6 minute walk test). In all patients, a right and left cardiac catheterization including coronary angiography and EMB following a standardized protocol was performed. Baseline values are presented in Table 1.
Baseline parameters of patients with EMB and available data of pension insurance.

EMB: endomyocardial biopsy; BMI: body mass index; HLP: hyperlipoproteinemia; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease; Mca: acute myocarditis; MCc: chronic myocarditis; DCM: dilative cardiomyopathy.
All included patients were contacted by letter and asked for permission for data query from the German statutory pension insurance program. Data on employment status were retrieved from the four leading nationwide pension providers. The queries included work intensity (activity description), unemployment days after inpatient stay and, if applicable, retirement parameters covering a follow-up of 24 months. We calculated time to RTW in absolute values and in dependence of physical workload.
Out of the 1153 patients, 564 (48.9%) answered and 87 (7.5%) rejected the inquiry. A total of 391 patients gave a positive consent for data query and had a complete data set of hospital and insurance information. Out of them, several essential socio-medical data (including parameters of work intensity) were missing in 171 patients, thus a final complete data set could be used for analysis of 220 patients (see Figure 1).

Inclusion flow chart.
Institutional review board (IRB) approval was obtained via the Human Research Ethics Committee of University of Potsdam, Germany (No. 44/2013; 18 March 2014).
Statistics
Continuous variables are expressed as means ± standard deviation (SD) and categorical variables as frequencies and percentages. Univariate analyses were performed using log-rank tests/Kaplan–Meier plots to compare and visualize cumulative incidences for time to RTW. EMB data and clinical records were linked with RTW data and analyzed for prognostic ability by Cox regression. Candidate variables for a multiple logistic regression model were found by stepwise forward selection based on maximum likelihood criteria. Selected variables were kept in the model even if they lost significance.
Effects with a p value of less than 0.05 (two-sided) were considered significant. Calculations were carried out using SPSS 22.0 (IBM, Chicago, IL, USA) and STATA 14.2 (StataCorp LP, College Station, TX, USA).
Results
Clinical data
Signs of systemic infection prior to heart failure symptoms were given in 53.3%. Main initial symptoms were breathlessness and angina. Mean left ventricular ejection fraction (LVEF) was 47.1% ± 18.6% (LVEF <45% in 46.3%) (Table 2). A coronary artery disease could be diagnosed in 3.2% of the patients. Left ventricle was bordered dilated as well as left atrium. Mean echocardiographic LVEF was reduced to 47.1% and only few patients (3.7%) had a moderate to severe diastolic dysfunction (E/E′ > 12). A left bundle branch block was documented in 15.4%. Left ventricular end-diastolic pressure was slightly increased, while pulmonary artery pressure was normal.
Clinical, laboratory, and bioptic findings.

ECG: electrocardiogram; LBBB: left bundle branch block; LA: left atrium; LVEDD: left ventricular end-diastolic diameter; LVEDP: left ventricular end-diastolic pressure; LVEF: left ventricular ejection fraction; TAPSE: tricuspid annular plane systolic excursion; RAP: right atrial pressure; PAP: pulmonary artery pressure; 6 MWT: 6-minute walking test; CK: creatine kinase; CRP: C-reactive protein; Mca: acute myocarditis; MC: chronic myocarditis; DCM: dilative cardiomyopathy; MC-BL: borderline myocarditis; MCNo: no myocarditis; PVB: parvovirus B19; ACE-I: ACE inhibitors; ARB: angiotensin receptor antagonists; MRA: mineralocorticoid receptor blockers; ASA: acetyl salicylic acid; CCB: calcium channel blockers; CK-MB: creatine kinase muscle-brain type.
EMB data
An acute myocarditis was clinically suspected in 10.5%, whereas a proven active myocarditis according to the Dallas Classification was diagnosed by EMB in only 1.8%. Borderline myocarditis was detected in 24.5% and dilated cardiomyopathy in 22.3% of the patients (suspected in 21.4%). In 51.4% of the patients, no myocarditic pathologies were objected. In all, 29.2% of the patients had no viral infection in the EMB, nearly three quarters of patients were virus-positive with a predominance of parvovirus B19 (54.2%). Other viruses or mixed infection were found in 16.7%. Immunohistological parameters including quantification of CD 3, CD45RO classes, perforin-positive cytotoxic cells, and Mac-1 positive macrophages are presented in Table 2.
Predictive parameters for RTW
In 56.2%, the work intensity was described as light, in 15.7% as light to moderate, in 16.3% as moderate, and in 11.8% as severe. RTW was achieved after a mean interval of 168.8 ± 347.7 days. After 6, 12, and 24 months, 61.3%, 72.2%, and 76.4%, respectively, of the patients were reintegrated into the workflow. Time to first day of employment after EMB was independent on work intensity (Figure 2).
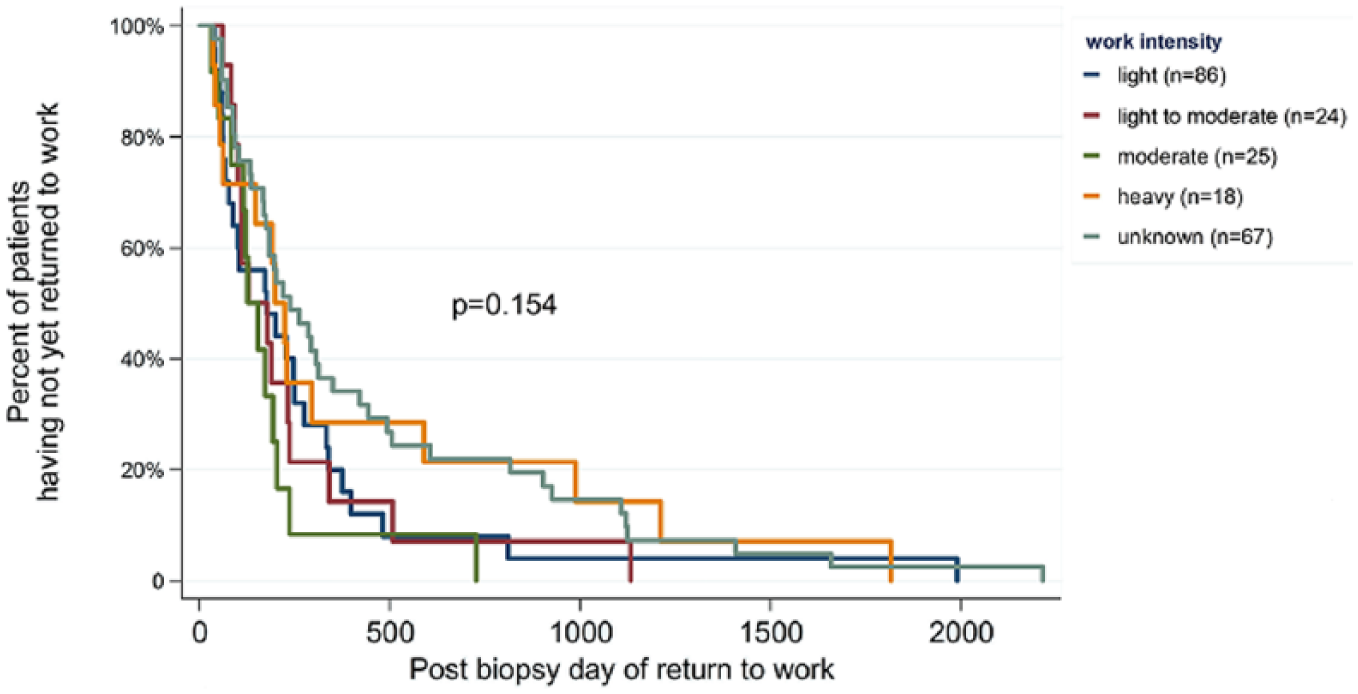
Time to RTW by previous work intensity.
None of the EMB-derived parameters was significantly associated with RTW, very early in the stepwise forward selection all invasive variables lost their significance. In the multivariate regression analysis including patients with suspected as well as with proven myocarditis, only age (per 10 years, hazard ratio (HR), 1.27; 95% confidence interval (CI), 1.10–1.46; p = 0.001) and LVEF (per 5% increase, HR, 1.07; 95% CI, 1.03–1.12; p = 0.002) were associated with increased probability of RTW. In contrary, elevated work intensity (heavy vs light, HR, 0.58; 95% CI, 0.34–0.99; p < 0.049) was associated with a decreased reintegration rate (Figure 3).
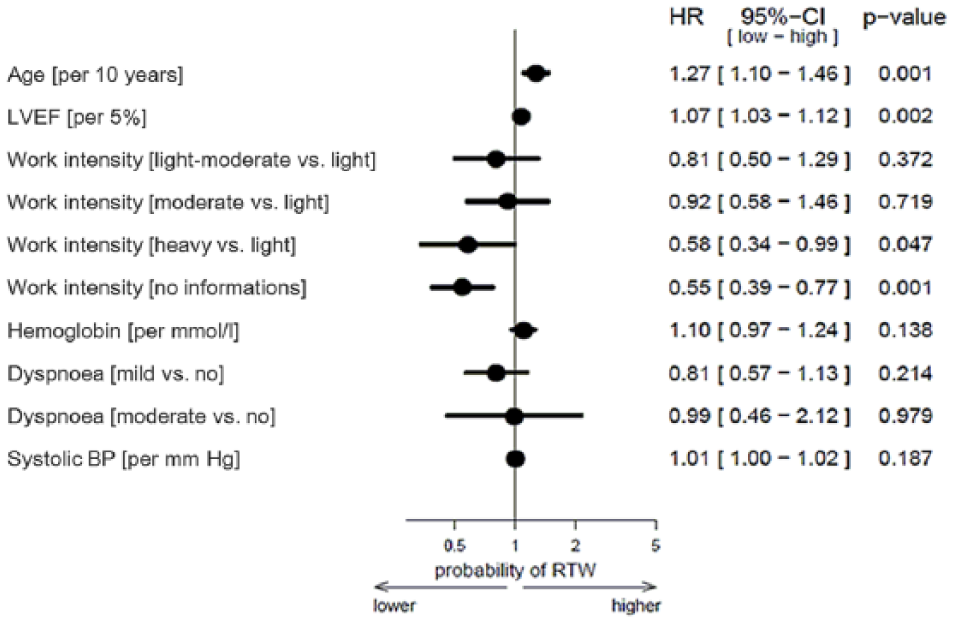
Cox regression of suggested predictors for successful RTW for patients with suspected myocarditis.
Analyzing only patients with biopsy-proven myocarditis (n = 107), again age (per 10 years, HR, 1.36; 95% CI, 1.09–1.70; p = 0.006) and LVEF (per 5% increase, HR, 1.09; 95% CI, 1.02–1.17; p = 0.002) were associated with increased probability of RTW. Clinical symptoms at the first presentation, particularly weakness (HR, 3.38; 95% CI, 1.69−6.78; p = 0.001), angina (HR, 1.89; 95% CI, 1.03–3.46; p = 0.040), and rhythm disorders (HR, 2.46; 95% CI, 1.27–4.76; p = 0.008), were predictive for a successful reintegration (Figure 4).

Cox regression of suggested predictors for successful RTW for patients with proven myocarditis.
Discussion
Our study has three important findings. First, all data derived from EMB are not predictive for the probability of RTW in multivariate analysis. Second, conventional prognostic parameters including age, left ventricular function, intensity of professional workload, and parameters at the first clinical presentation are the most important factors in this population. Finally, after a follow-up of 2 years, only three quarters of the young patients are successfully reintegrated into the working process.
EMB offers the opportunity to confirm a clinically suspected diagnosis of myocarditis in patients with heart failure of unknown origin. Histological and immuno-histochemical analysis supports the differentiation between acute myocarditis, borderline or chronic myocarditis, or postinflammatory dilated cardiomyopathy. Quantification of T-cell markers CD3 and CD45RO, Mac-1 positive macrophages, as well as perforin-expressing cytotoxic cells are helpful instruments to estimate the malignancy and enable prognostic assessment. 15 Although sensitivity of EMB is limited due to sampling error, multiple bioptic probes of right and left ventricular myocardium enable a reliable diagnosis of underlying damage pattern. In earlier CMR imaging studies of biopsy-proven viral myocarditis, the presence of late gadolinium enhancement (LGE) yielded the highest HR for all-cause and cardiac mortality. 16
Nevertheless, advantages of EMB for clinical and therapeutic decisions are not accompanied by additional benefits for socio-medical evaluation. After adding to conventional parameters, none of the EMB-derived parameters was significantly associated with RTW. Particularly, parameters suspecting an adverse clinical course including high level of CD3 positive T-cells (>10) and Perforin expression (>5) as well as Mac-1 positive cells (>45) had no impact on prediction of RTW, thus demonstrating a gap between clinical and socio-medical prognostic parameters. Similarly, we do not found any correlation between RTW data and invasive parameters including left ventricular, right atrial and pulmonary pressure, or echocardiographic parameters except LVEF.
Large predictive value in multivariate analysis showed a higher age (for 10 years HR, 1.27; 95% CI, 1.10–1.46). While traditionally a higher age is associated with a reduced RTW rate in other cardiac populations, 17 there is still a complete lack of data regarding post-myocarditic patients. It could be assumed that patients at higher age have a higher motivation to RTW than younger patients. Furthermore, it might be possible that younger patients have not yet returned to the work process as part of a retraining program (duration over 3 years). This differentiation cannot be given by the data of the pension insurance. In contrast, as expected, higher LVEF predicted a significant better professional reintegration (for 5%, HR, 1.07; 95% CI, 1.03–1.12). A normal left ventricular systolic function constitutes one of the most important prognostic parameters in various cardiac entities including dilated and ischemic cardiomyopathy 18 and biopsy-proven myocarditis. 19
In acute coronary syndrome (ACS) patients, RTW rate is determined by medical parameters such as left ventricular function, residual ischemia and rhythm stability, as well as by occupational requirement profile such as the blue- or white-collar work, night shifts, and the way capacity.20,21 In the present investigation, work intensity was inversely associated with the probability of RTW. A large part of patients after myocarditis suffer from weakness, angina, and arrhythmias still for months after index event. Although there is often no correlate in cardiopulmonary exercise testing, the subjectively perceived performance can be restricted subjective representing the limiting factor for RTW particularly in physically demanding professions. 22
Focusing of those part of the patients with biopsy-proven myocarditis, again neither EMB data nor therapeutic strategies offer a prognostic impact on the end-point of RTW. This knowledge underlines that particularly clinical (LVEF, symptoms at first presentation) and demographic (age) parameters are the key factors for socio-medical decisions in this heart failure population.
Reemployment rate of 76.4% after 24 months was low in this patient group, thus almost every fourth patients failed to return to normal working life. This is of particular importance because all patients were in a workable age at the start or the middle of the professional employment life span. Disease-related unemployment in young patients pushes deprivation, poverty, and further progression of functional impairment. 23 Underlying reasons for failing reintegration are not documented in this investigation. Cardiologic parameters including persistent angina in parvovirus B19-infections, persistent systolic and diastolic dysfunction, or general performance limitation might be partially responsible. Nevertheless, it can be assumed that in accordance with ACS populations the most important factors of non-RTW are of psychosocial origin including uncertainty, lack of knowledge, and anxiety. Further analyses are needed to objectify individual reasons to reduce the financial and psychosocial consequences of unemployment and early retirement.
Until now, there are only few observational, non-randomized data regarding the effectivity of RTW in post-myocarditic patients. 24 This refers to the effectiveness of cardiac rehabilitation after myocarditis as well. In Germany, due to the statutory jurisdiction that concedes the right to participate in a cardiac rehabilitation (CR) program for every patient, randomization is restricted due to legal and ethical boundaries and the effect of CR on RTW cannot be evaluated independently. While extensive publications deal with aspects of sports eligibility decisions in competitive or leisure time athletes suffering from myocarditis, limited and partly outdated data give recommendations for cardiac rehabilitation.25–27 Striking is the complete absence of suggestions for reemployment strategies. In the 2013 position statement from the ESC Working Group on Myocardial and Pericardial Diseases, 13 the problem of professional reintegration is not mentioned, as well as in the American College of Cardiology Foundation/American Heart Association (ACCF/ACC) guidelines for the management of heart failure. 28 Increased efforts focusing on this subject could be helpful to create evidence-based recommendations for this vulnerable population. Patients with reintegration risk factors described here should be placed in the center of consideration.
Some limitations have to be considered. First, the analysis includes patients with clinically suspected as well as patients with EMB-proven myocarditis. All patients were hospitalized with clinical manifestation of recent-onset non-ischemic cardiomyopathy and heart failure symptoms, summarizing patients with normal, mid-range, and reduced ejection fraction. This causes a certain inhomogeneity of the analyzed population. Second, as a methodological limitation, sampling errors on principle might contribute to false EMB results. Furthermore, only the first invasively measured LVEF during the EMB was included into the prediction model. We did not focus on therapeutic interventions as well as on the effect on LVEF. Likewise, out of an extensive population of patients who were hospitalized due to acute heart failure, we only could use the insurance data of those who give the written consent for data linking with insurance parameters. This selection bias might impact on results. Furthermore, we did not apply a classification of the work intensity using the provided metabolic equivalents over the time, but focused on a self-assessment of work-related physical load. This subjective stratification could lead to variations between workload categories. Due to the complexity of the RTW process, it is essential to include psychological parameters into the model, which we could not realize due to the retrospective approach of the investigation.
Conclusion
Added to established predictors including advanced age, reduced LVEF, and increased work intensity, bioptic data demonstrated no additional impact for RTW probability. Socio-medical evaluation of patients with suspected myocarditis furthermore remains an individually oriented process based primarily on clinical and functional parameters.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
IRB approval was obtained via the Human Research Ethics Committee of University of Potsdam, Germany (No. 44/2013; 18 March 2014).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the support of the Deutsche Forschungsgemeinschaft and Open Access Publishing Fund of University of Potsdam.
Informed consent
Written informed consent was obtained from all subjects before the study.