
Abstract
A 76-year-old man who had undergone percutaneous coronary intervention suffered intermittent claudication. Duplex ultrasonography revealed superficial femoral artery stenosis with an intraluminal heterogeneous echogenic mass. We suspected that stenosis was caused by the puncture procedure of the Angio-Seal. Open surgery revealed that a collagen sponge that should have been outside the arterial wall was misplaced in the wall with massive granulation, and atherectomy with patchplasty was performed. Vessel deterioration was considered due to several factors, including inappropriate access site, arterial wall calcification, and comorbidities like Behçet’s disease. Ultrasonography is a convenient and useful method to evaluate arterial lesions.
Introduction
Angio-Seal® (St. Jude Medical Company, St Paul, MN, USA) is one of the most widely used vascular closure devices (VCDs) in the world, consisting of an extra-arterial collagen-sponge, an intra-arterial anchor, and a bio-absorbable suture connecting them, which induces hemostasis through a sandwich technique. 1 We report a case of collagen sponge misplacement into the arterial lumen during the use of Angio-Seal, which was repaired surgically immediately after the detection of symptomatic lesions via duplex ultrasonography (DUS).
Case report
A 76-year-old man with comorbidities including hypertension, dyslipidemia, chronic renal disease (serum creatinine: 1.6 mg/dL), ischemic coronary disease, and Behçet’s disease underwent percutaneous coronary artery intervention through the right femoral artery with a 6 Fr sheath, and the Angio-Seal device was used for the closure of the access site. Three days after discharge, the patient experienced intermittent claudication, and he was re-admitted to our hospital. The ankle-brachial pressure index (ABI) had worsened starting from before, to immediately after, and 3 days after the intervention (1.03, 0.88, and 0.63, respectively). Procedure-related arterial stenosis was suspected, and he was referred to the Department of Vascular Surgery.
An initial survey with DUS revealed a heterogeneous echogenic mass in the proximal superficial femoral artery (SFA) that caused hemodynamically significant stenosis, which was indicated by high blood flow of more than 4 m/s (Figure 1(a) and (b)). The “anchor” of the Angio-Seal, which should be tagged to the intra-arterial lumen, cannot usually be observed as such a mass. Therefore, we assumed that the collagen sponge connected to the suture was misplaced into the arterial lumen. Contrast-induced computed tomography (CT) revealed that the access site was in the SFA and was adjacent to arterial wall calcification (Figure 1(c)). Surgical re-intervention was required for the stenosis with clinical ischemic symptoms, high blood flow on DUS, and low ABI. We considered endovascular intervention, including stenting or stent-grafting, to be contraindicated in this case because the punctured site was located in the inguinal region, a so-called “non-stenting zone.”
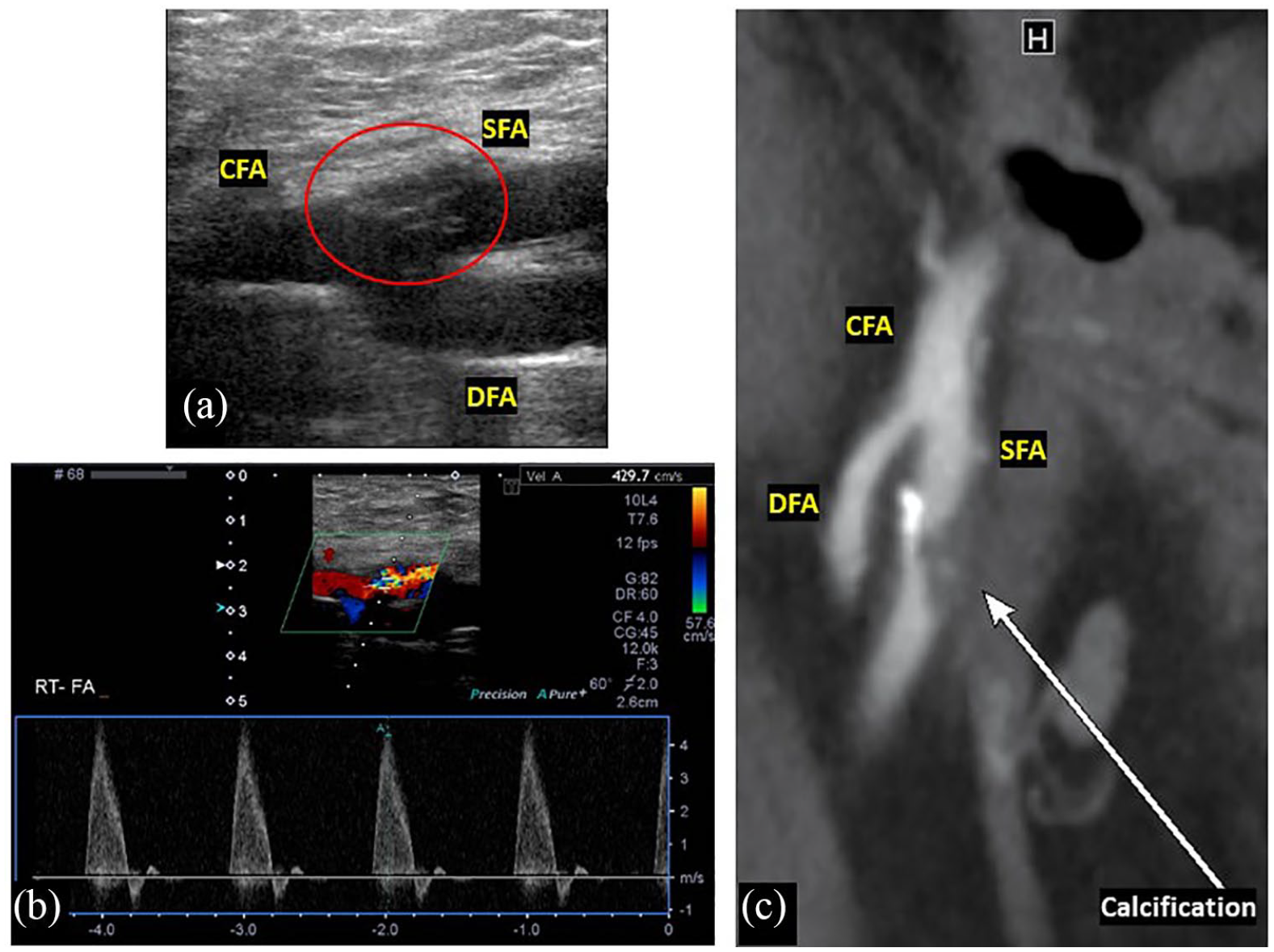
(a) Duplex ultrasonography demonstrated the femoral bifurcation and a heterogeneous echogenic mass (red circle). (b) Doppler ultrasound analysis revealed severe stenosis of the SFA (peak systolic velocity: 429.7 cm/s). (c) Contrast-enhanced CT revealed stenosis and adjacent arterial calcification.
An incision in the femoral artery revealed the intra-arterial lumen with an artifact mass, granulation, and small blood clots (Figure 2). After atherectomy and patchplasty, the ABI improved to the normal range (1.06).

The incision in the femoral artery revealed the intra-arterial lumen with an artifact mass, granulation, and small blood clots.
The pathological findings revealed that the resected specimen included a sponge-like artifact and granulation accompanied by inflammatory cells. The postoperative course was uneventful, and the patient was discharged on postoperative day 3.
Discussion
Contrast-enhanced CT demonstrated the site of stenosis and calcification distribution well. However, it could not reveal the structure of the intraluminal mass or the severity of the stenosis. Ultrasonography is known to decrease the number of attempts as well as the time required for successful puncture. In contrast, ultrasound guidance has been reported to be time-consuming in cases with strong femoral artery pulsation. 2 However, the information gained from DUS—detecting the morphology of the femoral bifurcation, severity of the stenosis, and arterial wall structure—should be important for successful deployment of the Angio-Seal device.
SFA puncture using Angio-Seal is contraindicated. 3 Kadner et al. revealed that only seven cases (0.4%) among 1600 Angio-Seal deployments showed vascular complications. However, all severe complications occurred following SFA puncture. 4 Yokoyama et al. reported five major complications that required vascular surgery in a total of 283 cases using the Angio-Seal device, and three of the five had undergone SFA puncture. 3 They recommended re-puncture at the common femoral artery (CFA) in case the SFA was found to have been punctured by fluoroscopy. We assume that DUS should also be used due to its less invasiveness.
The femoral bifurcation, which can sometimes cause migration of catheters or wires, should be one of the reasons for contraindication of SFA puncture, besides the relatively smaller diameter of the SFA compared to the CFA. Six of the 7 major complications in the previous report required reconstruction of the femoral bifurcation using a bovine pericardial patch, as in our case. 4 As most patients who undergo endovascular therapy have an atherosclerotic nature, local plaque, calcification, and poor run-off of the lower extremity would be risk factors for arterial issues. 5 DUS should be handy and useful not only for detecting calcification adjacent to the puncture site but also for evaluating the severity of SFA calcification. 6 In our case, deeper examination with DUS should have been performed even on the hostile groin due to multiple interventions.
Vascular Behçet’s disease is characterized by early occurrence of an anastomotic false aneurysm due to vessel deterioration. 7 We recognized this intractable recurrent chronic systemic inflammatory disease, which should be paid full attention before intervention. 8 Information regarding the patients’ comorbidities, including inflammatory and genetic diseases, would be important to predict tissue fragility. In this case, however, we believe that the complication was mainly due to procedural failure and that the Behçet’s disease was not a significant factor.
We will use the DUS guidance more frequently in the future, especially for obese patients or those with calcification or systemic inflammatory/genetic backgrounds, based on the lessons learned from this case.
Conclusion
We reported a case of collagen sponge misplacement into the arterial lumen during the use of Angio-Seal, which was immediately and concisely detected via duplex ultrasonography.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent has been obtained from the patient for publication of the case report and accompanying images.