
Abstract
Perivascular epithelioid cell neoplasms represent a group of uncommon mesenchymal tumours with as yet undiscovered benign counterpart. Although perivascular epithelioid cell neoplasms have been described arising in most organ systems as well as in soft tissue and bone, only a small number of perivascular epithelioid cell neoplasms have been reported in the bladder. To date, there is no agreed system for predicting the behaviour of these tumours. We describe a case of a perivascular epithelioid cell neoplasm of the bladder arising in a 57-year-old male and initially diagnosed on biopsy and present a review of the literature focussing on the pathological differential diagnosis and the importance of key histological features in conjunction with a broad immunohistochemical panel. This case report highlights the key features of bladder perivascular epithelioid cell neoplasms that distinguishes these rare neoplasms from other bladder lesions.
Keywords
Introduction
Perivascular epithelioid cell neoplasms (PEComas) are a heterogeneous group of uncommon mesenchymal neoplasms defined by their dual myomelanocytic differentiation.1,2 Originally described as several distinct pathologic entities, the common features shared by tumours belonging to the PEComa family was first intimated by Pea et al. in 1991, who noted the morphologic similarities between angiomyolipomas (AML) and clear cell ‘sugar’ tumours (CCST) of the lung. 3 Subsequent studies in the past decades have expanded our current understanding of the PEComa family, which in addition to its founding members AML, CCST and lymphangiomyomatosis (LAM) now includes clear cell myomelanocytic tumour of the falciform ligament/ligamentum teres (CCMMT), and other clear cell tumours seen in multiple viscera. In practice, the general term PEComa is typically reserved for tumours with dual myomelanocytic phenotype other than the classically defined and specifically named AML, LAM, CCMMT and CCST. The most commonly involved sites are the gynaecological and gastrointestinal tracts,2,4 with sporadic reports describing PEComas in other sites including soft tissue, skin, bone and genitourinary tract. 5 PEComas of the bladder are rare, with just over 20 cases described in the English literature (reviewed by Xuesong et al.), most of which were diagnosed on resection. We describe a bladder PEComa diagnosed on biopsy (later confirmed at partial cystectomy), with emphasis on the differential diagnosis and how immunohistochemistry can be used to diagnose this rare neoplasm on limited material.
Case history
A previously well 57-year-old male presented with recent onset haematuria and left groin pain. A 2-mm ureteric stone was found on computed tomography of kidneys, ureters and bladder (CT KUB) which was managed conservatively, following which the patient’s symptoms resolved. A routine follow-up ultrasound at 7 months detected an incidental 24-mm well-defined hypoechoic lesion indenting the posterior bladder wall. Cystoscopy revealed a well-circumscribed sub-urothelial mass in the right posterior bladder wall. A biopsy was sent for pathological analysis.
Histology demonstrated a tumour involving the detrusor muscle, comprising spindled to ovoid cells with abundant granular cytoplasm (Figure 1). Mild nuclear pleomorphism was observed, but mitoses were not a feature. Immunohistochemistry showed the tumour cells to be positive for HMB45 and smooth muscle actin (SMA; Figure 1). The tumour cells were negative for cytokeratins, desmin, Melan-A, Dog-1, CD117, prostate-specific antigen (PSA), CD34, neuroendocrine markers and CD68. Ki-67 proliferation index was less than 10%. The diagnosis of PEComa was made. Excision was recommended, but a period of surveillance was agreed upon after discussion with the patient. A magnetic resonance imaging (MRI) performed 9 months hence showed an increase in tumour size to 28 mm (Figure 2), and the patient subsequently underwent a robotic partial cystectomy, which was performed without complications.
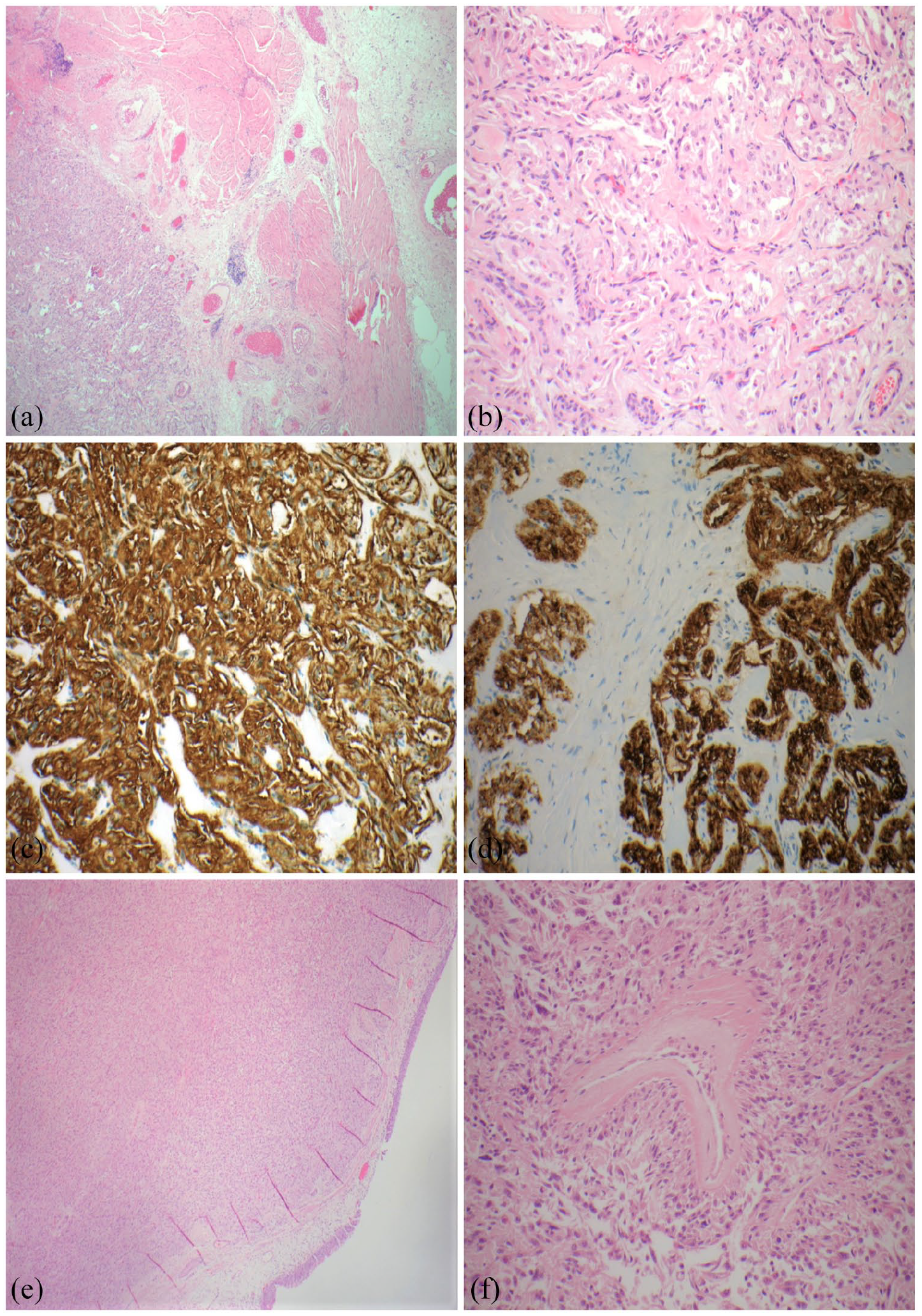
(a–d) Biopsy images and (e and f) resection images: (a) a low power view of the tumour deep to the muscularis propria (H&E, ×4 objective), (b) high power view of spindle/epithelioid cells (H&E, ×20 objective), (c) positive staining for actin (IHC, ×20 objective), (d) positive staining for HMB45 (IHC, ×20 objective), (e) low power view of tumour in bladder wall, extending close to the overlying urothelium (H&E, ×4 objective) and (f) central blood vessel with characteristic tumour cells radiating outwards (H&E, ×20 objective).

Sagittal T2-weighted MRI image demonstrating an intermediate signal intensity soft tissue mass located in the dome of the bladder (arrow) with an intact bladder wall and no extravesical invasion.
Grossly, the tumour measured 37 mm and was centred on the submucosa and muscularis propria, with focal surface ulceration. The tumour had a tan homogeneous cut surface with central cystic change and focal haemorrhage. Microscopically, the appearances were similar to the biopsy findings, with the additional feature of tumour cells arranged perpendicularly to blood vessels (Figure 1(e)). No coagulative necrosis, infiltration or lymphovascular invasion were identified. The mitotic count was 2 per 10 high power fields. Immunostaining confirmed the diagnosis of a PEComa, with tumour cells expressing HMB45, SMA, caldesmon and vimentin, and negative for MyoD1, desmin, Melan-A, AE1/AE3, CD117, synaptophysin and Chromogranin A. The tumour was closely excised by 0.2 mm.
A post-operative MRI 6 months after surgery showed no evidence of local recurrence or metastatic disease. The patient will continue close follow-up with interval cystoscopy surveillance.
Discussion
The term PEComa currently refers to tumours with a dual myomelanocytic phenotype that are related to other members of the PEComa family, including AML and clear cell tumours of the lung. 1 Overall, PEComas show a female predilection; earlier work suggested bladder PEComas were more common in males; 6 however, a recent review describes a slight female predominance, with a median age of 32.1 years (range = 16–65). 7 PEComas may present with non-specific local symptoms but are frequently incidental findings. Bladder PEComas may be associated with abdominopelvic discomfort, lower urinary tract symptoms and haematuria, 6 at times mimicking urothelial carcinoma clinically.
PEComas of the bladder have a similar morphologic appearance to PEComas arising in other organs, with a variable proportion of epithelioid and spindle cells with clear to eosinophilic cytoplasm, round nuclei with smooth nuclear membranes and occasionally prominent nucleoli. 8 A range of architectural patterns have been described, including nests, sheets, fascicles and herringbone ‘fibrosarcoma like’ areas.6,8 As identified in our case, most tumours at least focally display the characteristic finding of epithelioid cells intimately associated with and radiating out from vessel walls. 9 A subset of PEComas harbours a translocation involving TFE3 gene and most commonly SFPQ. 10 These TFE-associated PEComas are usually comprised almost exclusively of epithelioid cells in a nested or alveolar pattern. 11
Immunohistochemistry is crucial in establishing the diagnosis of a PEComa. Melanocytic marker expression is characteristic, but can be patchy or only focal, with HMB45 the most consistently expressed followed by Melan-A and microphthalmia transcription factor (MiTF). 12 S100 positivity has been observed in up to a third of reported cases. 12 Myoid markers similarly show a variation in frequency of expression, with SMA most often positive, and at least focal desmin positivity in approximately 30% of PEComas. 12 Muscle-specific actin and caldesmon expression have also been reported, as well as cytoplasmic MyoD1 staining. 13 TFE-associated PEComas show some differences in their immunoprofiles, displaying diffuse rather than patchy expression of HMB45 and other melanocytic markers, and focal if any myoid biomarker expression. 11
As a rare tumour of the bladder, PEComas may be confused with more common bladder lesions also characterised by a spindle cell/epithelioid morphology. The diagnosis can be even more challenging in biopsy samples as the full spectrum of histological features may not be evident. Several entities enter the differential diagnosis, including smooth muscle tumours, paraganglioma, sarcomatoid urothelial carcinoma, melanoma, schwannoma, inflammatory myofibroblastic tumour (IMT) and post-operative spindle cell nodule (PSCN) (Table 1). While cases of smooth muscle tumours of the gynaecological and urinary tract expressing melanocytic markers have been documented, positivity for HMB45 in these lesions is typically focal and smooth muscle markers are strong and diffuse, with the reverse pattern of expression seen in PEComas. 14
Key immunohistochemical features of PEComa and important differentials in the bladder.

SMA: smooth muscle actin; SMT: smooth muscle tumour; SUC: sarcomatoid urothelial carcinoma; IMT: inflammatory myofibroblastic tumour; PSCN: post-operative spindle cell nodule.
S100 expression in sustentacular cells only.
Positive in melanotic variant.
Paragangliomas express neuroendocrine markers, with S100 positivity confined to sustentacular cells. 15 Differentiation from non-mesenchymal tumours such as sarcomatoid urothelial carcinoma is aided by the lack of expression of cytokeratins.16,17 Melanoma is uncommon in the urinary bladder and is more likely metastatic in origin than a primary tumour. The lack of expression of smooth muscle markers and typically strong and diffuse expression of melanocytic markers, particularly S100, will point to the diagnosis of melanoma. 18 PEComa should also be differentiated from PSCN and IMT. PSCN and IMT share many similarities (Table 1); both lesions are characterised by a spindle cell proliferation, usually in a myxoid or oedematous stroma, with associated chronic inflammation and prominent blood vessels.16,19 Histological features favouring PSCN/IMT over PEComa include (1) the presence of a chronic inflammatory cell infiltrate and myxoid stroma, (2) patchy positivity for cytokeratins on immunohistochemistry and (3) in the case of IMT, ALK-1 reactivity.6,16 Schwannoma is a rare lesion in the bladder, composed of spindle cells with bland round to oval nuclei (Table 1). In contrast to most PEComas, schwannomas show strong immunopositivity for S100 and vimentin, with negative reactivity for actin and other myoid markers. 20
PEComas at most sites have been traditionally managed by complete resection, with adjuvant therapy employed for locally advanced or metastatic disease. Histological findings that may predict aggressive behaviour include tumour size >5 cm, high nuclear grade, infiltrative growth, tumour necrosis and mitotic count >1/50 high power field showing associations with tumour behaviour. 12 Most PEComas arising in the bladder follow a benign course; 6 however, a few cases with metastatic disease have been reported, highlighting the need for long-term follow-up of all patients.
Conclusion
PEComas are rare tumours of the bladder that can present a diagnostic challenge, particularly when they are only partly sampled. Immunohistochemical studies are crucial in confirming the diagnosis and excluding several other entities that may mimic a PEComa but which have significantly different management approaches and prognoses. In our patient, a conservative surgical approach was possible upon establishing the correct diagnosis.
Footnotes
Acknowledgements
The authors are grateful to our patient for their participation and to Ms Andrea Tay for facilitating the patient’s consent.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.