
Abstract
Pyloric exclusion is a method of treatment for duodenal injury. Surgery is usually needed to restore digestive continuity in due time, yet a new surgical procedure can be challenging due to fibrotic adhesion development. We present here a retrospective case series of three patients with pyloric exclusion who underwent endoscopic ultrasound–guided duodenal repermeabilization using metallic stents. All procedures were successful with no complication and allowed regular feeding. This case series shows that endoscopic ultrasound–guided recanalization is a feasible and safe procedure.
Background
Pyloric exclusion (PE) and digestive diversion are commonly performed in case of severe duodenal injury (traumatic or after acute pancreatitis). Exclusion is usually achieved by surgical stapling. 1 When duodenum injuries heal, gastroenteric disassembly is necessary to prevent bypass side effects such as malnutrition, diarrhea and dumping syndrome. Most often disassembly is followed by a spontaneous duodenal patency restoration, 2 otherwise a fresh operation is required to avoid upper gastrointestinal (GI) obstruction. Adherence and fibrosis make surgical procedures more challenging. We present here an endoscopic ultrasound (EUS)–guided procedure to restore duodenal permeability after PE.
Endoscopic recanalization procedures were performed under EUS and fluoroscopy guidance and followed the following steps:
A linear echoendoscope (Olympus Medical Systems Tokyo, Japan) was advanced into the stomach to the suture line.
The excluded duodenal loop was identified by EUS imaging and accessed using a 19 gauge “access” needle (19A Echotip Cook Endoscopy, Winston-Salem, NC).
Contrast was injected to confirm the proper location of the duodenal limb.
A 0.035 guide wire (Jagwire™, Boston Scientific, Marlborough, MA, USA) was then advanced through the needle into the duodenum.
In the first case, we dilated the tract with a 6 French (Endo-flex Gmbh, Germany) cystotome and then with a 12 mm diameter balloon (CRE, Boston Scientific). The 12 cm partially covered metal Hanarostent™ was then advanced and deployed through the tract in the duodenum, while the large uncovered proximal flare of the stent was anchored to the stomach with four clips.
In the other two cases, we directly used the Hot AXIOS™ electrocautery enhanced delivery system (AXIOS 15-10-mm) to dilate the tract before deploying the AXIOS stent into the duodenum in a single-step procedure (Figure 1).

Steps of EUS guided duodenal recanalization: (a) Characterization of excluded duodenum, (b) duodenal punction under EUS control, (c) contrast injection to control proper location, (d) opening the distal flange, (e) proximal flange positioning and (f) deployed Axios stent.
Institutional review board (IRB) approval was not needed for this article, all patients gave written consent.
Case presentation
Case 1
A 56-year-old man who underwent PE and jejunostomy 3 months earlier for a duodenal perforation due to an alcoholic necrotizing pancreatitis, was referred for endoscopic duodenal recanalization; endoscopy showed complete pyloric occlusion with no signs of leak or fistula. We restored duodenal continuity with a partially covered metallic 12 cm stent (Hanaro stent, MI Tech, South Korea) anchored to the stomach by TTS clips. The patient resumed oral liquid feeding after 24 h. We performed a follow-up endoscopy 1 month later: proximal stent migration was observed with a stent loose in the stomach, and the pylorus lumen was moderately narrowed, with contrast injection showing a 15 mm diameter mild pyloric stenosis. After hydraulic dilation with a 20 mm diameter balloon, the patient resumed normal oral feeding within 24 h and has remained symptom free since then, with a normal diet.
Case 2
A 36-year-old man underwent PE and gastrojejunal diversion for ballistic duodenal injury; gastrojejunostomy was disassembled after a good outcome. The patient was referred after experiencing occlusion symptoms, and the endoscopic evaluation noted a complete duodenal occlusion, with no duodenal contrast passage. We performed a duodenal recanalization using a 15 mm wide Hot AXIOS™ stent (Boston Scientific). The patient was discharged the next day and was able to resume oral liquid feeding. One month later, the stent was still in place, no dilation was necessary after stent removal. The patient resumed normal oral feeding, but he experienced pseudo-occlusion symptoms 1 month later; endoscopy showed mild pyloric stenosis which was successfully treated by balloon dilation sessions.
Case 3
A 29-year-old male who underwent a PE and gastrojejunostomy 18 months earlier after a car accident was referred for endoscopic duodenal recanalization. Endoscopy found a complete duodenal occlusion. Endoscopic duodenoduodenostomy was performed using a 15 mm wide Hot AXIOS™ stent; the patient resumed oral feeding 1 day after the procedure. One month later, the stent was easily removed and the tract presented a good patency. The 2-month control endoscopy showed a patent tract, with a smooth scope passage (Figure 2). However, dilation was performed with an 18 mm diameter balloon before diversion reversal in order to consolidate patency and allow fully solid food intake.
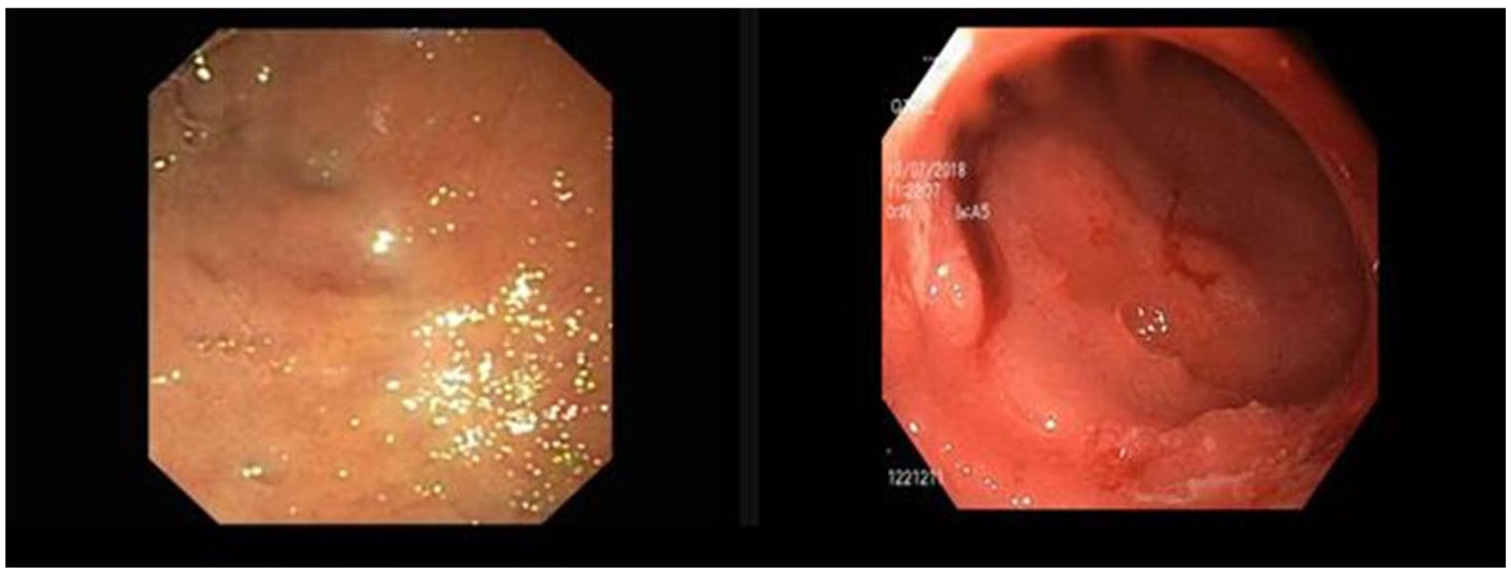
Left image: Duodenal occlusion before recanalization; right image: recanalized track after stent removal.
Discussion
PE with gastrojejunostomy was originally described in 1977 as treatment for severe duodenal injury. This technique temporarily occludes the pylorus and diverts the gastric’s stream from the duodenum during the healing phase. In 94% of the cases, pylorus patency resumes spontaneously, 1 otherwise a new procedure is necessary to restore normal flow through the duodenum.
CO2 insufflation and new endoscopic devices have brought new insights in digestive therapeutic endoscopy. Where digestive perforations used to be deemed dreadful complications in the past, creating an access through the digestive wall and getting inside the peritoneal cavity can now be part of some endoscopic procedures.
Recanalization of complete digestive obstruction has been described in case reports, using the rendez-vous technique,3,4 which requires a prior ostomy and two operators with two scopes, or using a needle knife5,6 to create a passage for a guidewire through the occluded web. However, this latter approach is “blind” and subsequently unsafe in the absence of direct or indirect view of the occluded path.
EUS-guided recanalization technique as described here allows an easy and safe access to the duodenum, under direct and live sonographic view of the occluded limb, no prior ostomy is needed, and all the procedure can be performed expeditiously by a single operator.
Metallic stents are commonly used in digestive stenosis. Stent expansion is intended to apply a constant radial force to the stenotic track and therefore induce tissue remodeling. However, covered metal stents experience a high migration rate, especially when used for benign stenosis. Choi and Al reported a 62.5% migration rate for benign pyloric stenosis, 7 making stenting less effective and responsible for symptom recurrence. Even if some anchoring methods are available such as stent fixation with endoscopic snare, 8 or with through-the-scope (TTS), 9 Ovesco clips 10 or suturing systems, 11 these methods are either ineffective, unpractical or technically demanding, and often expensive.
Lumen-apposing metal stents (LAMS) seem to be more appropriate as they experience a lower migration rate thanks to their dumbbell design that allows better anchorage. In addition, LAMS are well tolerated and easy to deploy and to remove.12,13 Hot AXIOS™ delivery system allows a single-step stent insertion with no device exchange, for a safe and faster procedure while maintaining relative cost neutrality. 14
After stent removal, hydraulic balloon dilation can still be necessary to increase tract diameter and ensure comfortable and regular oral ingesta, because the repermeabilized tract diameter may not be sufficient at the time of stent removal; in our experience stent migration for the first patient and diameter of the AXIOS stent (15 mm) may have been responsible of the tightening of the tract. It will need to be seen whether a longer indwelling duration and a larger stent diameter may improve the results and avoid subsequent endoscopic dilation.
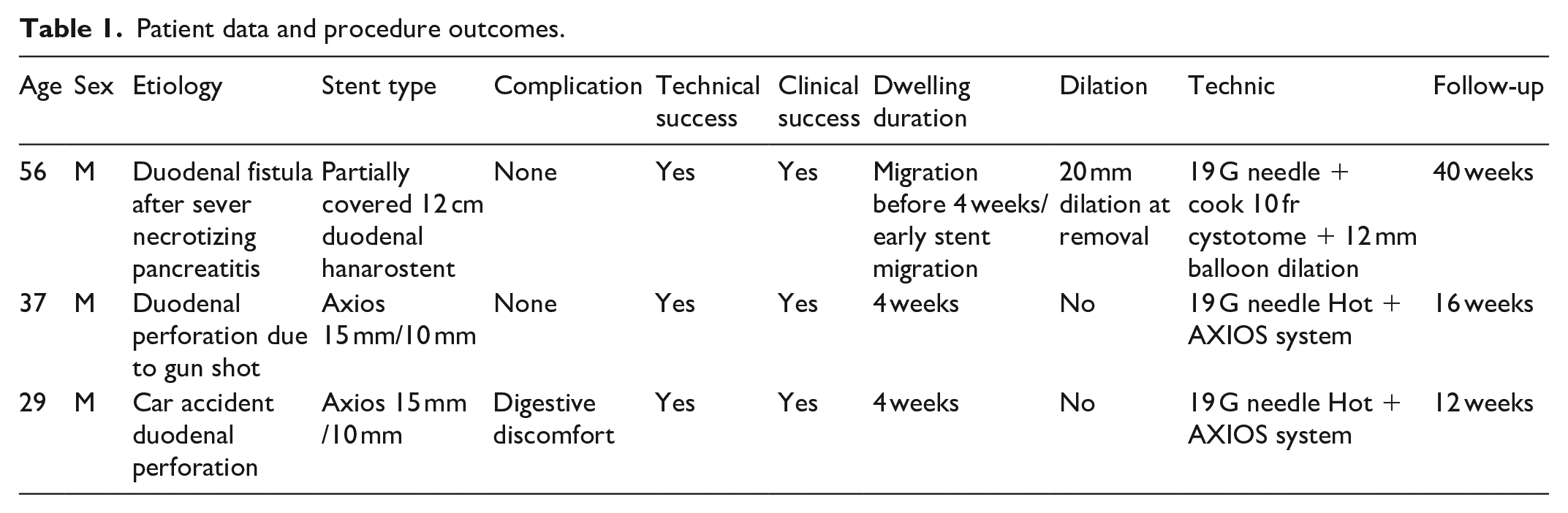
M Martínez-Guillén et al. 15 also reported EUS-guided recanalization in the esophagus and colon with good result. Yet to our knowledge, this is the first case series reporting duodenal/pyloric recanalization (Table 1).
Patient data and procedure outcomes.
Conclusion
All procedures were successful with no complications. This shows that endoscopic recanalization procedures are possible and safe; they offer a good alternative to surgery with a short recovery time, a high success rate and less morbidity.
Footnotes
Author contributions
Hicham El Bacha wrote the manuscript. Frederic Prat is the professor in charge of the medical care and the following of the patient; he did the correction of the paper. All authors read and approved the final manuscript. Carlo Jung, Bertrand Brieau, Benoit Bordacahar, Sarah Leblanc, Maximillien Barret, Arthus de Chaumont, Bertand Dousset are patients’ physicians in charge of diagnosis and follow-up.
Availability of data and materials
Data and supporting materials are available freely to any scientist wishing to use them.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patients for publication of this case series and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.