
Abstract
Objectives:
Tuning fork vibration sensation testing is widely used as a diagnostic test to detect diabetic neuropathy. However, evidence-based literature indicates that reliability between examiners is low. Attaching isosceles triangle diagrams on tuning forks lowers the discrepancy between examiners. This study aimed to analyze the relationship between vibration sensation measurement using an improved tuning fork and the presence of callus and wound development in patients with diabetic peripheral neuropathy.
Methods:
Participants included 56 general older adults and 52 patients with diabetic peripheral neuropathy. The methods included confirmation of the presence or absence of callus, range of motion of the ankle and the first metatarsophalangeal joint, vibratory sensitivity of the medial malleolus and the dorsal aspect of the first distal phalanx using an improved tuning fork, and touch-pressure sensitivity of the plantar aspect of the hallux. Patients with diabetic peripheral neuropathy were followed up for 3 years to check for the presence or absence of wounds.
Results:
When compared with the general older adults, the patients with diabetic peripheral neuropathy had significantly lower touch-pressure sensitivity (p < 0.01), vibratory sensitivity at the distal phalanx (p < 0.01) and medial malleolus (p < 0.01), ankle dorsiflexion range of motion (p < 0.01), and metatarsophalangeal joint extension range of motion (p < 0.01). The area under the receiver operating characteristic curve with callus formation was 0.93 for the medial malleolus and 0.96 for the distal phalanx, indicating that the accuracy of the distal phalanx was higher (p < 0.01) than the medial malleolus. According to the Cox proportional hazard analysis, the vibratory sensitivity of the distal phalanx was a significant risk factor for ulcer development (p < 0.05).
Conclusion:
These findings suggest that the vibration sensation test, which we improved via the technique described in this study, is useful for predicting the occurrence of callus and ulcer.
Introduction
The national healthcare expenditure in Japan is reported to have exceeded 43 trillion yen in 2018 and is expected to increase in the future. 1 The medical cost of lower extremity wounds is expected to increase due to the increase in the number of patients with diabetes and chronic dialysis. In addition, there are many patients whose lower extremity wounds lead to amputation, and it has been reported that one limb is amputated every 30 s worldwide.2,3 Therefore, prevention, early detection, and early intervention of lower extremity wounds, including diabetic foot lesions, are important.
Several factors have been reported to contribute to the development of lower extremity wounds. These include decreased visual acuity, limited range of motion (ROM), shoe incompatibility, edema, and decreased somatosensory perception.4–7 In a multivariate meta-analysis review of factors predicting lower extremity wounds, the important clinical predictors were age, sex, duration of diabetes, vibration perception threshold, monofilament, pulse rate, ankle-brachial index, peak plantar pressure, and foot deformity.8,9 Diabetic foot lesions remain a medical, social, and economic problem in many countries, 3 with approximately 25% of the patients with diabetes developing lower extremity wounds during their lifetime and up to 2% requiring amputations. 10 In Western countries, diabetes is the leading cause of non-traumatic amputations, with an amputation rate approximately 15 times higher than that of non-diabetic patients. 11 However, approximately 85% of amputations due to diabetic foot lesions can be prevented with proper care and education. 12
According to epidemiological data on neuropathy, approximately 50% of the cases of diabetic foot lesions are due to neuropathy, 15% are due to peripheral arterial occlusive disease, and the remaining 35% are due to a combination of neuropathy and vascular disease.13–15 Therefore, it is important to understand the extent of diabetic peripheral neuropathy (DPN), as it is the cause of many lower extremity wounds. Furthermore, it is important to determine the presence or absence of DPN, which can cause a variety of ability impairments, such as loss of gait balance, in addition to diabetic foot lesions.16,17
Useful tests for neurological findings indicative of diabetic neuropathy include the Achilles tendon reflex, vibration perception by tuning fork, and touch-pressure sensation by monofilament. 18 In addition, the monofilament test, the vibratory sensation test with a 128-Hz tuning fork, and the Ipswich Touch Test are recommended for determining the loss of protective sensation among the evaluation items. 19 The vibratory sensation test with a 128-Hz tuning fork correlates with a biothesiometer and baroreflex.20,21 In addition, Oyer et al. 22 reported that the vibration test with a tuning fork detected decreased measurements in patients with DPN while monofilament test failed to detect the decrease. High specificity and reliability of the tuning fork test was reported during DPN screening, 23 while its simplicity and availability are known in the clinical setting. 24 However, results by tuning fork are semi-quantitative due to the difficulty in performing in a reproducible manner; hence, a simpler, more quantitative test is needed. In fact, the typical method of measuring vibration perception using a 128-Hz tuning fork has low inter-inspector reliability due to the variation in vibration intensity depending on the striking strength.25,26 However, it is possible to perform vibration perception tests with high inter-inspector reliability by attaching an isosceles triangle diagram to the tuning fork. 27 Using this improved method, we reported an association between a decrease in vibration perception and the prediction of falls. 28 Problems with loss of vibration are reportedly common in patients with foot ulcers; however, the direct relationship is still unclear. 29 Therefore, whether our modified tuning fork vibration test is also useful in predicting callus and ulcer formations of diabetic neuropathy should be clarified. We hypothesized that our modified vibration test, which shows higher inter-examiner reliability, would have a high relationship with callus and wound formation in the lower extremity.
Therefore, the purpose of this study was to determine the usefulness of the vibratory sensation test using our modified tuning fork in predicting calluses and lower extremity wound development. First, we analyzed the area under the receiver operating characteristic (ROC) curve with callus formation in the vibration sensation test on the medial malleolus and first distal phalanx in community-dwelling older adults and patients with DPN to clarify the valid method to detect the callus formation in the patient with DPN. Second, a multivariable analysis was conducted to find the independent relationship of the vibration sensation test with the callus formation. Moreover, we performed a prospective cohort study in patients with DPN to determine the relationship of the modified vibratory sensation test with the occurrence of lower extremity wounds in a multivariable analysis.
Methods
Subjects
Participants included 56 older adults without DPN (26 males and 30 females, 74.1 ± 4.3 years old) and 52 patients with DPN (21 males and 31 females, (mean value ± standard deviation (SD)) 74.1 ± 2.8 years old, 11.9 ± 3.1 years history of diabetes mellitus (DM)). Patients with DPN were defined as those diagnosed with DPN by a physician using the diagnostic criteria for diabetic polyneuropathy from the Japanese Study Group on Diabetic Neuropathy 30 (Supplemental file 1). Exclusion criteria were dementia, central neuropathy, and peripheral neuropathy not caused by DPN. All patients with DPN were diagnosed with type 2 diabetes under glycemic control with oral medications with or without insulin injections. The data of glycated hemoglobin (HbA1c) in the patients with DPN were 8.3 ± 1.5%.
Ethical considerations
The purpose of this study was fully explained to the participants, and informed written consent was obtained. There were ample decision capacity, documentation of consent, and disclosure. This study was approved by the Ethics Committee of the Naragakuen University (approval no. 3-009).
Examination method
Physical examinations were performed to assess the presence or absence of calluses, ROM of the ankle dorsiflexion and the first metatarsophalangeal (MTP) extension, vibratory sensitivity of the medial malleolus and dorsal aspect of the first distal phalanx, and touch-pressure sensitivity of the plantar aspect of the hallux.
Presence of callus
The presence or absence of calluses was assessed by observing the plantar surface of the foot in a supine position. To determine the location of the calluses, the plantar surface was divided into six regions. First, the plantar was divided into three major regions: the rearfoot (27% of the foot length), the midfoot (28% of the foot length), and the forefoot and toes (45% of the foot length). The forefoot was subdivided in width into the medial forefoot (55% of forefoot width) and the lateral forefoot (45% of forefoot width). The forefoot was also subdivided lengthwise into the hallux (final 20% of forefoot length and 33% of forefoot width) and the toe (final 20% of forefoot length and 67% of forefoot width). 31 If two calluses were present, both were described.
Touch-pressure test
The touch-pressure test was performed at the hallux in a supine position using a Semmes-Weinstein Monofilament (SWM) level of 5.07 (10 g). 32 Since the tests at other foot sites showed statistically similar results as at the hallux (Supplemental file 2), we adopted the hallux alone as the test site to avoid multicollinearity in multivariable analyses.
ROM test
ROM of the ankle dorsiflexion and the first MTP extension were measured using a goniometer in increments of 5°. 33 The measurement was performed in a supine position with the knee extended to simulate the motion during walking.
Vibration sensation test
The vibration sensation test was conducted in a supine position using a tuning fork (128 Hz; Nichion, Funabashi, Japan). Ten seconds are generally considered the standard time for the vibration test, as it is one of the simple diagnostic criteria for DPN. 34 However, testing with a tuning fork has some issues, such as variations in the strength of the tapping and the time between the tapping and the initiation of measurement. In addition, there is a lack of uniformity in which part of the body is measured, such as the medial malleolus or toes. Thus, an isosceles triangle was attached to the tuning fork, and improvements were made to keep the intensity of the vibration constant (Figure 1). The modified tuning fork forms an isosceles triangle that gradually becomes larger in the center as the vibration becomes smaller. The measurement was started when the vertex of the isosceles triangle formed by the afterimage reached the third horizontal line from the bottom, and the vibration sensing time (seconds) was measured with a digital stopwatch. The intra-inspector reliability of the conventional method was 0.93–0.99, and the intra-inspector reliability of the improved tuning fork was 0.98–0.99. 27 The inter-inspector reliability of the conventional method was 0.86–0.98, and the inter-inspector reliability of the improved tuning fork was 0.96–0.98. 27 Both the intra-inspector reliability and inter-inspector reliability of the improved tuning fork method were better than those of the conventional method. The measurement was performed at the medial malleolus and dorsal aspect of the first distal phalanx of both feet. The final result of each measurement site was recorded as the mean of two readings.

A tuning fork (C-128 Hz aluminum tuning fork manufactured by Nichion) was used for the test. The tuning fork was modified using an isosceles triangle diagram, because the strength of the vibration varied depending on the intensity of the tapping when used as is. The modified tuning fork forms an isosceles triangle that gradually becomes larger in the center as the vibration becomes smaller. The measurement was started when the vertex of the isosceles triangle formed by the afterimage reached the third horizontal line from the bottom, and the vibration sensing time was measured with a digital stopwatch. 22
Extraction of factors involved in callus formation in patients with DPN
Variables such as age, sex, body mass index (BMI), history of DM, touch-pressure sensation at the hallux, vibration sensation of the medial malleolus and the first distal phalanx, and ROM of the ankle dorsiflexion and the first MTP extension were entered as explanatory variables, and factors significantly related to the presence or absence of callus and the target variable were extracted by a stepwise method using logistic regression modeling analysis.
Effect of vibration sensation of the first distal phalanx on wound development in patients with DPN
For patients with DPN, the foot conditions were assessed every month after the examination was conducted and followed up for 3 years to determine if there was any wound development. For the analysis, we used the forced imputation method in a Cox proportional hazards analysis with ulcer occurrence as the objective variable and the factors involved in callus formation, including vibration sensation at the first distal phalanx and the presence of calluses, which is a major cause of ulcer occurrence, as explanatory variables.
Statistical analyses
Statistical analyses were performed with EZR. 35 The χ2 test was used to compare sex, the presence of callus, and the touch-pressure sensation between the general older adults and the patients with DPN. An unpaired Student’s t-test was performed to compare the results of the ROMs, touch-pressure sensation, and vibration sensing time between the two groups. For the comparison of the measurement sites of the vibration sensation test in the callus formation, the ROC curve was drawn with the presence or absence of the callus as the objective variable and the vibration sensing time of the medial malleolus and the first distal phalanx as the explanatory variable, using the area under the curve. The factors involved in callus formation in patients with DPN were extracted using logistic regression analysis. In addition, a Cox proportional hazards analysis was performed on the occurrence of lower extremity wounds in patients with DPN, with the factors involved in callus formation and the presence of calluses as explanatory variables. All statistical significance levels were set at p < 0.05.
Results
Comparison of general older adults and patients with DPN
Callus was detected in 8 out of 56 general older adults (14%; two calluses were found on the hallux, five on the medial forefoot, and one on the lateral forefoot) and 27 of 52 patients with DPN (51.9%; eight calluses on the hallux, two on the toe, fourteen on the medial forefoot, seven on the lateral forefoot, and five on the rearfoot), and the callus was observed more frequently among patients with DPN (p < 0.01) (Table 1).
Comparison in characteristics between general older adults and patients with DPN.

BMI: body mass index; ROM: range of motion; MTP: metatarsophalangeal; NS: not significant.
ROM of the ankle dorsiflexion was 15.5 ± 3.5 and 12.3 ± 6.3 degrees for the general older adults and the patients with DPN, respectively. ROM of the first MTP extension was 46.9 ± 5.3 and 35.1 ± 11.4 degrees for the general older adults and the patients with DPN, respectively. In both measurement sites, the patients with DPN displayed significantly lower ROMs than the general older adults.
In the SWM test, 49 out of 56 general older adults and 23 out of 52 patients with DPN perceived a 5.07 monofilament, respectively. Thus, the touch-pressure sensation in patients with DPN was significantly lower than that in general older adults.
The difference in sex, presence or absence of callus, and touch-pressure sensitivity was analyzed using the χ2 test. The difference in age, height, weight, BMI, vibration sensation (the medial malleolus), vibration sensation (the first distal phalanx), ROM (the ankle dorsiflexion), and ROM (the first MTP extension) was analyzed with unpaired Student’s t-test.
Comparison of the test sites of the vibration perception test in the callus formation
The vibration sensing time of the medial malleolus was 8.0 ± 1.5 s and 4.9 ± 1.4 s for the general older adults and the patients with DPN, respectively (Tables 2 and 3 and Figures 2 and 3). The vibration sensing time of the first distal phalanx was 8.4 ± 1.7 s and 3.8 ± 1.8 s for the general older adults and the patients with DPN, respectively. The vibration sensing time of both sites was significantly shorter in the patients with DPN than in the general older adults, and the vibration sensing time was significantly shorter at the first distal phalanx than at the medial malleolus in the patients with DPN.
Comparison of vibration sensation on the medial malleolus and the first distal phalanx between the general older adults and the patients with DPN.
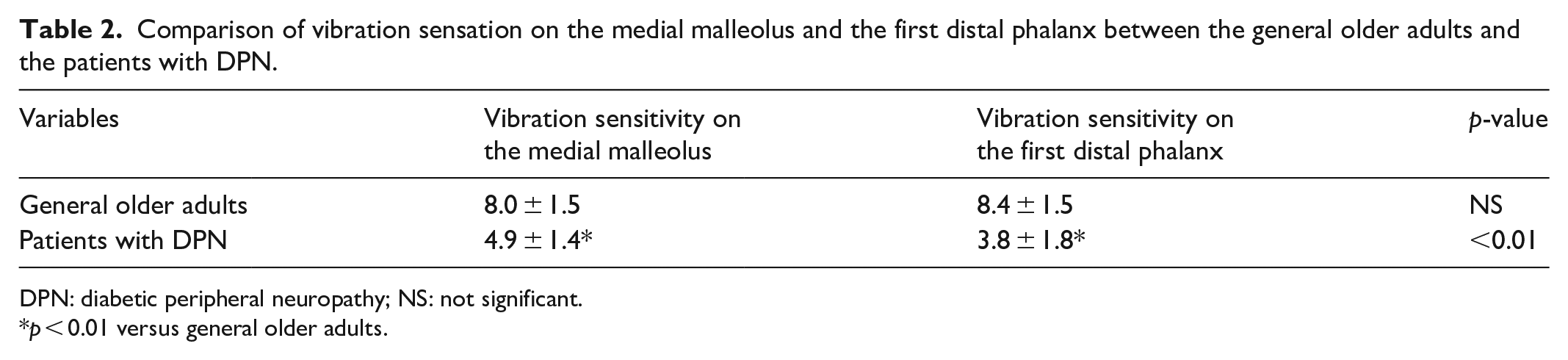
DPN: diabetic peripheral neuropathy; NS: not significant.
p < 0.01 versus general older adults.
Comparison of vibration sensation between the medial malleolus and the first distal phalanx using ROC curve.

Likelihood-ratio test p < 0.0001.

ROC curve of vibration sensation on medial malleolus.

ROC curve of vibration sensation on dorsal aspect of the first distal phalanx.
The area under the ROC curve with callus formation was 0.93 for the medial malleolus and 0.96 for the first distal phalanx. The cutoff values were 6.6 s for the medial malleolus (sensitivity = 78.6%; specificity = 88.5%) and 6.3 s for the first distal phalanx (sensitivity = 87.5%; specificity = 94.2%) with higher accuracy in the distal phalanx when compared with that of the medial malleolus.
Factors involved in callus formation in the patients with DPN
Factors involved in the formation of callus in the patients with DPN were extracted as the independent factors: length of morbidity history, decreased vibration perception on the first distal phalanx, and BMI (Table 4).
Independent factors for the presence or absence of callus in the patient with DPN.

BMI: body mass index.
Likelihood-ratio test p < 0.001.
Three-year investigation of lower extremity wounds in the patients with DPN
Forty-nine patients (20 males and 29 females, 74.3 ± 3.5 years old, 11.8 ± 3.0 years history of DM) were available for a 3-year follow-up of the foot condition of the patients with DPN. Seven of the 49 (14%) patients developed lower extremity wounds in the plantar surface of the hallux (three patients), the metatarsal head (MTH) (two patients), and the fifth toe (two patients) (Figure 4). According to the Cox proportional hazards analysis, factors involved in callus formation and the presence of callus were included as explanatory variables. Only vibration sensation on the first distal phalanx was a significant risk factor for the development of lower extremity wounds (Table 5).
Cox proportional hazard comparison in lower extremity wound development.

BMI: body mass index.
Likelihood-ratio test p < 0.001.

Incidence of lower extremity wounds in subjects followed for 3 years.
Discussion
In this study, we examined whether the previously reported 27 vibratory sensation test using a modified tuning fork could be a predictor of the callus and lower extremity wound formation in patients with DPN. The results showed that (1) the first distal phalanx was found to be more critical than the medial malleolus as a site for measuring vibration sensitivity, which is useful for predicting callus formation; (2) the vibratory sensation test using the modified tuning fork was an independent factor for callus formation; and (3) the test was a stronger predictor of lower extremity wounds than the presence of calluses or other factors involved in callus formation.
First, we compared several measures involved in callus formation, including the vibratory sensation test using our modified tuning fork, in the general older adults and patients with DPN. Previous reports indicate that patients are prone to callus formation due to increased local foot pressure during walking due to decreased ROMs of ankle dorsiflexion and the first MTP extension and increased somatosensory threshold.36–39 In this study, patients with DPN also displayed limited ROMs of the ankle dorsiflexion and the first MTP extension, and increased thresholds of touch-pressure perception and vibration sensation. The prevalence of callus formation was significantly higher in the patients with DPN than in the general older adults (8 of 56 general older adults: 14% vs 27 of 52 patients with DPN: 51.9%; p < 0.01). These results are similar to those reported by Yavuz. 40 These results supported the conclusion that patients with DPN in this study had the symptoms of DPN and can be considered the appropriate sample of patients with DPN.
Before the analysis for callus and wound formation, we found a difference in the vibration sensitivity between the first distal phalanx and the medial malleolus. There was no difference in the vibration sensitivity between the two sites in the general population of older adults, but a significantly shorter vibration perception time was observed in the first distal phalanx than in the medial malleolus in the patients with DPN (p < 0.01). In addition, the sensitivity and specificity of callus formation were higher in the test at the first distal phalanx than at the medial malleolus. Since DPN is a distal polyneuropathy, 41 vibration sensation thresholds may be elevated at more distal sites in the patients with DPN. From these results, the neurological change could be refracted more clearly at the first distal phalanx than at the medial malleolus in the patients with DPN; therefore, we adopted the site of the first distal phalanx for the following investigation.
From the multivariable analysis for callus formation in this study, diabetes duration, BMI, and vibration sensitivity on the first distal phalanx measured by our modified tuning fork were extracted as risk factors. DPN causes autonomic neuropathy and collagen glycation, which leads to decreased mobility and deformity of the foot.42–44 Patients with a long history of DPN are more likely to develop calluses due to repeated abnormal gait with foot deformity and limited ROM. 45 Therefore, callus formation can be affected by various factors, including rigidity. However, this study found that among the above factors, deficient vibration sensation rather than rigidity around the foot was a significant cause for callus formation. These results suggest the importance of considering the independent concepts of neural function as well as disease duration and body thinness, and the predominance of vibration sensitivity as a neural function for the callus formation.
Next, we conducted a prospective cohort study to identify whether a vibratory sensation test using our modified tuning fork could be useful in predicting wound development in patients with DPN. Specifically, we followed the patients with DPN for 3 years to investigate the relationship between lower extremity wounds and the independent factors of callus formation (diabetes duration, BMI, and vibratory sensation on the first distal phalanx measured by the modified tuning fork) or the presence of calluses. Out of 49 patients who were followed up, 7 (14%) were observed to have lower extremity wounds in the plantar surface of the hallux (3 patients), the MTH (2 patients), and the fifth toe (2 patients). Interestingly, the Cox proportional hazards analysis indicated that the vibration sensation test on the dorsal aspect of the first distal phalanx was extracted as an independent risk factor and was a stronger predictor than the presence of callus or other factors involved in callus formation. In this prospective investigation, while 86% of ulcers were developed at the site of callus, the developmental rate of foot ulcer in the patients with callus was only 27%. These results suggest that the callus is a predictive factor of the site of ulcer developments but could not predict ulcer development itself. However, this study found the decrease in vibration sensing time as an independent factor for foot ulcer development, and an additional analysis of ROC curve for ulcer developments indicated the 2.4 s cutoff value (Supplemental file 3). The percentage of patients with ulcer development in the patients with callus and vibration sensing time lower than 2.4 s was 53.8%, which was higher than the ratio in the patients with callus alone. This suggests that vibratory sensation on the first distal phalanx may be one of the most important tests as a predictor of lower extremity wounds and that the vibrotactile sensation test using our modified tuning fork is highly useful. A larger study needs to be conducted to detect a more reliable cutoff value. With respect to the mechanism in the predominance of vibration sensing for ulcer development, the receptor in vibration sensing is Pacinian corpuscles, 46 a receptor known for pressure sense on the dermis. 47 Although the relationship of this receptor and the foot ulcer development has been unclear, the receptor of deep sensory could be a mediator related to ulcer development. More detailed and pathological investigations are needed to reveal the mechanism.
Cognizance is raised to the clinical fact that vibration perception and touch-pressure sensation tests are important in assessing the risk of developing diabetic foot lesions, 48 and it has been reported that the combination of vibration testing using a tuning fork and touch-pressure testing using an SWM provides results that are comparable to those of the International Consensus on the Diabetic Foot. 49 In these reports, the conventional vibration testing method was used. The test using a modified tuning fork, applied in this study using isosceles triangles, is more reliable than the conventional tuning fork test method. This may enable more valid measurements when combined with the touch-pressure test. In fact, the risk factors for diabetic foot lesions are believed to be caused by a combination of several factors. 50 Among these, peripheral neuropathy, foot deformity, trauma, peripheral vascular disease, and peripheral edema are the major causes. Except for trauma, these risk factors do not directly cause lower extremity wounds. 51 According to a 1999 UK–US collaborative study, the most common combination of factors causing lower extremity wounds was peripheral neuropathy, foot deformity, and trauma. 5 Therefore, the measurement of vibration sensation on the dorsal aspect of the first distal phalanx with a modified tuning fork, which was identified as a factor in this study, should also be used in combination with these risk factors.
The limitation of this study is the small sample size in the prospective analysis for wound development. The statistical validities of multivariable analyses of the logistic regression analysis for callus formation and the Cox proportional hazards analysis for ulcer development were supported by the likelihood-ratio test with significant p-value (p < 0.001). However, multivariable analysis generally requires a sample size of 60–80 with 3–4 explanatory variables, and this study has sample sizes of 52 and 49 in the logistic regression analysis and the Cox proportional hazards analysis, respectively. 52 Therefore, the importance of vibration testing on the dorsal aspect of the first distal phalanx requires confirmation with a large-scale study in the future. In addition, the criterion for the diagnosis of DPN in Japan was used, which did not include temperature sensation and acupuncture. The items of exclusion criteria were limited due to the sample number in this study. These limitations are also expected to be addressed in future study.
Conclusion
The results of this study suggest that the vibration sensation test with improved quantification by applying the isosceles triangle to a tuning fork is useful for predicting callus development, and it is also necessary to compare the difference between the medial malleolus and the first distal phalanx in patients with DPN. It is also suggested that the vibration test on the first distal phalanx could be a predictor of lower extremity wounds.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221085097 – Supplemental material for Prediction of callus and ulcer development in patients with diabetic peripheral neuropathy by isosceles triangle-forming tuning fork
Supplemental material, sj-docx-1-smo-10.1177_20503121221085097 for Prediction of callus and ulcer development in patients with diabetic peripheral neuropathy by isosceles triangle-forming tuning fork by Yoshiyuki Yoshikawa, Noriaki Maeshige, Mikiko Uemura, Masayuki Tanaka, Nobuhide Kawabe, Atomu Yamaguchi, Hidemi Fujino and Hiroto Terashi in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221085097 – Supplemental material for Prediction of callus and ulcer development in patients with diabetic peripheral neuropathy by isosceles triangle-forming tuning fork
Supplemental material, sj-docx-2-smo-10.1177_20503121221085097 for Prediction of callus and ulcer development in patients with diabetic peripheral neuropathy by isosceles triangle-forming tuning fork by Yoshiyuki Yoshikawa, Noriaki Maeshige, Mikiko Uemura, Masayuki Tanaka, Nobuhide Kawabe, Atomu Yamaguchi, Hidemi Fujino and Hiroto Terashi in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121221085097 – Supplemental material for Prediction of callus and ulcer development in patients with diabetic peripheral neuropathy by isosceles triangle-forming tuning fork
Supplemental material, sj-docx-3-smo-10.1177_20503121221085097 for Prediction of callus and ulcer development in patients with diabetic peripheral neuropathy by isosceles triangle-forming tuning fork by Yoshiyuki Yoshikawa, Noriaki Maeshige, Mikiko Uemura, Masayuki Tanaka, Nobuhide Kawabe, Atomu Yamaguchi, Hidemi Fujino and Hiroto Terashi in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank general older adults and patients with DPN who participated in the measurements in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the ethics committee of the Naragakuen University (approval no. 3-009).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.