
Abstract
Objective:
We aimed to evaluate risk factors and outcome of cerebral edema in children with diarrhea.
Methods:
In this retrospective chart analysis, data of all diarrheal children under 5 years of age having convulsion and admitted in intensive care unit were retrieved from an electronic medical record system of Dhaka Hospital of International Centre for Diarrhoeal Disease Research, Bangladesh, from 1st January 2011 to 31st December 2016. Comparison of clinical and laboratory characteristics was made between children with (cases = 22) and without cerebral edema (controls = 66).
Results:
Cases more often had a fatal outcome than controls (36% vs 8%, p = 0.003). In logistic regression analysis, after adjusting for potential confounders, the cases were independently associated with respiratory distress (odds ratio = 5.5, confidence interval = 1.55–19.62, p = 0.008), severe sepsis (odds ratio = 4.6, confidence interval = 1.24–16.77, p = 0.022), and severe malnutrition (odds ratio = 0.16, confidence interval = 0.04–0.74, p = 0.019). A rapid drop (>0.5 mmol/L per hour) in serum sodium did not have any impact on developing cerebral edema (p = 0.090).
Conclusion:
Identification of simple clinical predictors may help in the early treatment of cerebral edema that may further help in reducing deaths in such children especially in resource-poor settings. However, further research with prospective design is needed to consolidate our observation.
Introduction
Cerebral edema is one of the life-threatening conditions that occur due to the accumulation of a large amount of water in the spaces of the brain. 1 Cerebral edema causes loss of subtle cerebral functions, 2 so that its early recognition and treatment should not be neglected. Cerebral edema usually presents with alteration in the level of consciousness, the appearance of bradycardia, rise in blood pressure, abnormal breathing patterns, evidence of extraocular movement abnormalities, alteration and inequality of pupillary size, and extensor plantar response on the side of the lesion. 1 In acute encephalitis, preceding seizures and status epilepticus are important risk factors for fulminant cerebral edema. 3 Hyperammonaemia (⩾200 μmol/L) in case of reduced hepatocyte function and during rapid correction is considered to be a risk factor for cerebral edema. 4
There are different causes of cerebral edema. Infective causes include meningitis, encephalitis, toxoplasmosis, and subdural empyema. 1 Non-infective causes include trauma or head injury, 5 diabetic ketoacidosis,1,6 massive cerebral infarction, ischemic stroke, intracerebral hemorrhages, brain tumor, hypoxia, other toxic or metabolic factors, 7 dysnatremia, 8 fulminant viral hepatitis, hepatic encephalopathy, systemic poisoning, syndrome of inappropriate antidiuretic hormone secretion (SIADH), opioid drug abuse and dependence, bites of certain reptiles and marine animals, and high-altitude cerebral edema. 1 However, there is no such study that looked for the risk factors of developing cerebral edema in children hospitalized for a diarrheal illness in a critical care ward. Intensive care unit (ICU) of the Dhaka hospital of International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) treats a lot of cases with convulsion. 9 Some of them had cerebral edema and often ended up with a fatal outcome. Thus, our aim was to find out the risk factors of cerebral edema in diarrheal children and their outcome after treatment.
Methods
Ethical statement
This is a retrospective chart analysis of the data that were initially obtained for patient management at Dhaka Hospital of icddr, b; patients or caregivers were not asked for an interview. The data were anonymized before they were retrieved. The written approval of the study was taken by the Institutional Review Board (IRB) of icddr, b, comprised of Research Review Committee (RRC) and Ethical Review Committee (ERC) of icddr,b.
Study design
We performed a retrospective chart analysis with an unmatched case-control design. All children of either sex, aged 0–59 months, admitted in the ICU with documented convulsion either at admission or after admission in ICU from 2011 through 2016 constituted the study population. Convulsive children who were assessed to have cerebral edema constituted the cases, and those without cerebral edema constituted the controls. We have only scope to diagnose cerebral edema depending on fundoscopy. On that basis, we did not find the features of cerebral edema in the control group. Controls were taken by randomization, which was 3-fold of the cases. In convulsing children, fundoscopic documentation 10 of papilledema (blurring of optic disk margin, other than medial margin which is a normal variant 11 ) was considered as a surrogate marker of cerebral edema. Fundoscopy was done multiple times a day, minimum once. It is prudent to mention that Dhaka hospital of icddr,b has no brain imaging (MRI, CT-scan) or intracranial pressure monitoring 7 facilities, and it is also not possible to send a clinically unstable child for imaging in a distant center. Presence of papilledema was diagnosed by attending physician and thereafter confirmed by a qualified pediatric intensivist (either M.C. or F.A.). Another objective criterion in diagnosing papilledema was the disappearance of blurring of an optic disk partially or completely within 24 h of initiation of treatment with either mannitol or 3% NaCl. After 6–8 h of each dose of mannitol, the response was evaluated by repeating the fundoscopic examination.
Study setting
The study children were admitted and treated at the ICU of the Dhaka Hospital of icddr,b. Description of the study site has been provided elsewhere. 12 ICU has the facilities for inotrope support, central oxygen support, noninvasive ventilation and mechanical ventilation in case of respiratory failure, and machine for continuous monitoring support. Data are documented in the electronic server of the hospital by ICU doctors. ICU team comprises of 9 doctors and 14 nurses with other supporting staff. Five junior doctors work according to the roster over 24 h. They are directly supervised by two mid-level physicians and finally overseen by two senior pediatric intensivists.
Patient management
Both the cases and the controls received anticonvulsant. In the ICU, they were followed up by ophthalmoscopy to detect cerebral edema if there was an alteration of mentation or irregular respiration. No children in the control group developed papilledema. The cases additionally received either mannitol or 3% NaCl. No child developed rebound raised ICP post mannitol. Hydration status was also routinely checked in every patient and found to be normal.
We treated hypernatremia by using G-ORS following Adrogue and Madias. 13 Patients who were kept nothing per oral for their clinical management perspective, their hypernatremia were treated with ½ strength Normal Saline and 5% dextrose. Fluid resuscitation was given to children with severe sepsis. 14 Inotropes were used for children who had septic shock. Bubble CPAP (continuous positive airway pressure), noninvasive ventilatory support was used for children having severe pneumonia with hypoxemia. 12 Mechanical ventilators were used in case of respiratory failure. Other management of the patients was done following a standardized protocol followed in the Dhaka hospital of icddr,b and the other management of hospitalized patient has also been described elsewhere. 15
Measurements
Case report forms (CRFs) were developed, pretested, and finalized for the acquisition of relevant data. Characteristics analyzed included age, sex, severe malnutrition (severe wasting (z score for weight for height/length <−3 of World Health Organization (WHO) growth standard), or severe underweight (z score for weight for age <−3 of WHO growth standard) or edematous malnutrition), presence of cough, respiratory distress, presence of vomiting, presence of fever (axillary temperature ⩾ 38ºC), presence of severe sepsis (sepsis-induced tissue hypoperfusion or organ dysfunction), 16 responsiveness, ileus, features of heart failure or fluid overload, presence of pneumonia, respiratory rate, hypoglycemia (<3 mmol/L), rapid drop in serum sodium (>10 mmol/L per 24 h), hyperkalemia (>5.3 mmol/L), hypokalemia (<3.5 mmol/L), hypernatremia (>150 mmol/L), hyponatremia (<135 mmol/L), metabolic acidosis (TCO2 < 18 mmol/L), hypocalcemia (<2.12 mmol/L), hypomagnesemia (<0.65 mmol/L), raised creatinine (1.5 times of upper limit of normal for age), growth of micro-organism in blood culture and rectal swab culture, duration of hospital stay, development of healthcare associated infection (evidence of new infections that was identified at least after 48 h of admission),17,18 and outcome.
Sample size calculation
During the 6-year study period, we have screened 1225 children under 5 years of age who presented with convulsion to the ICU, and only 22 fulfilled the criteria of cases; from the remaining patients, three controls for each case were selected randomly; thus, there were 66 controls.
Analysis
All data were entered into a personal computer and edited before analysis using SPSS for Windows (Version 20.0; IBM Corp., Armonk, NY) and Epi Info (version 7.0; Epi Info™ software; Centers for Disease Control and Prevention, Atlanta, GA, USA). Differences in proportions were compared by the chi-square test. To compare the means of normally distributed data, Student’s t-test was used and for comparison of data that were not normally distributed, Mann–Whitney test was used. A probability of less than 0.05 was considered statistically significant. The strength of association was determined by calculating the odds ratio (OR) and their 95% confidence intervals (CIs). Variables identified as significant in the bivariate analysis were used as independent variables to develop a predictive model using logistic regression. The dependent variable in that model was cerebral edema. Thus, independent risks for cerebral edema were identified using stepwise logistic regression analysis after controlling for the covariates.
Results
Median (inter-quartile range) age of the study children was 9.5 (4.3–16.5) months among cases and 8 (5.37–14) months among controls. Both the cases and controls had higher male child, 73% and 58% respectively (Table 1). In bivariate analysis, the cases most often found to have respiratory distress and severe sepsis and less likely to be severely malnourished compared to the controls (Table 1). The cases require more days to recover (Table 1), more often required a blood transfusion, mechanical ventilation and had higher case-fatality-rate compared to the controls (Table 2). Laboratory parameters were also similar in both groups. In all, 38 patients had hypernatremia (11 with cerebral edema and 27 without cerebral edema) (Table 3) and were treated by using G-ORS. Rapid drop of serum sodium (>10 mmol/day) was observed in 41% of cases and 20% of controls, and the difference was statistically insignificant. Other variables in Tables 1 and 3 were comparable among the groups. In logistic regression analysis, after adjusting for potential confounders, the independently associated factors for cerebral edema in diarrheal children under 5 years of age with convulsion were respiratory distress, severe sepsis, and severe malnutrition (Table 4).
Clinical characteristic of children under 5 years with (cases) or without (controls) cerebral edema admitted in ICU.
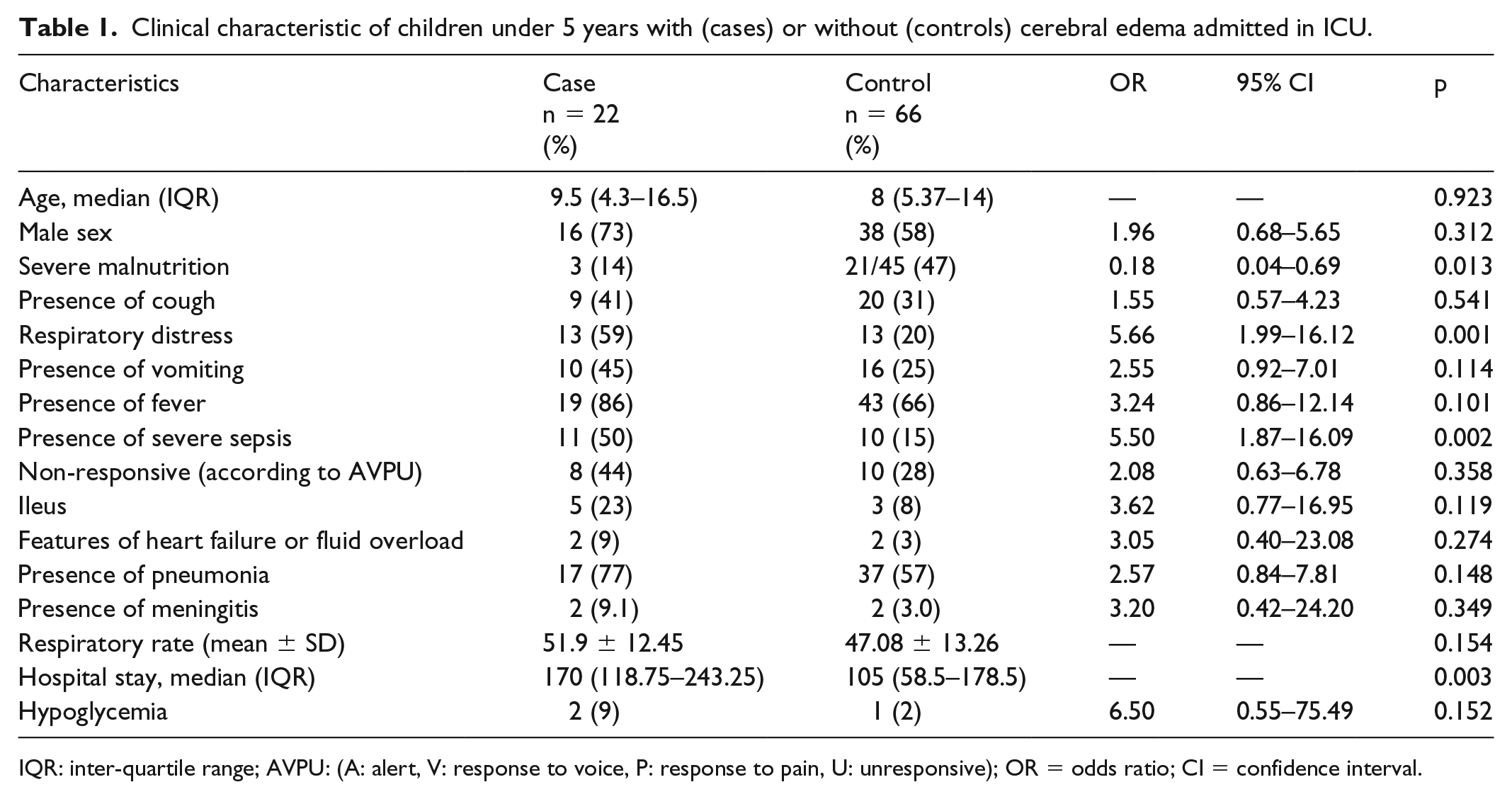
IQR: inter-quartile range; AVPU: (A: alert, V: response to voice, P: response to pain, U: unresponsive); OR = odds ratio; CI = confidence interval.
Outcome of the study patients.
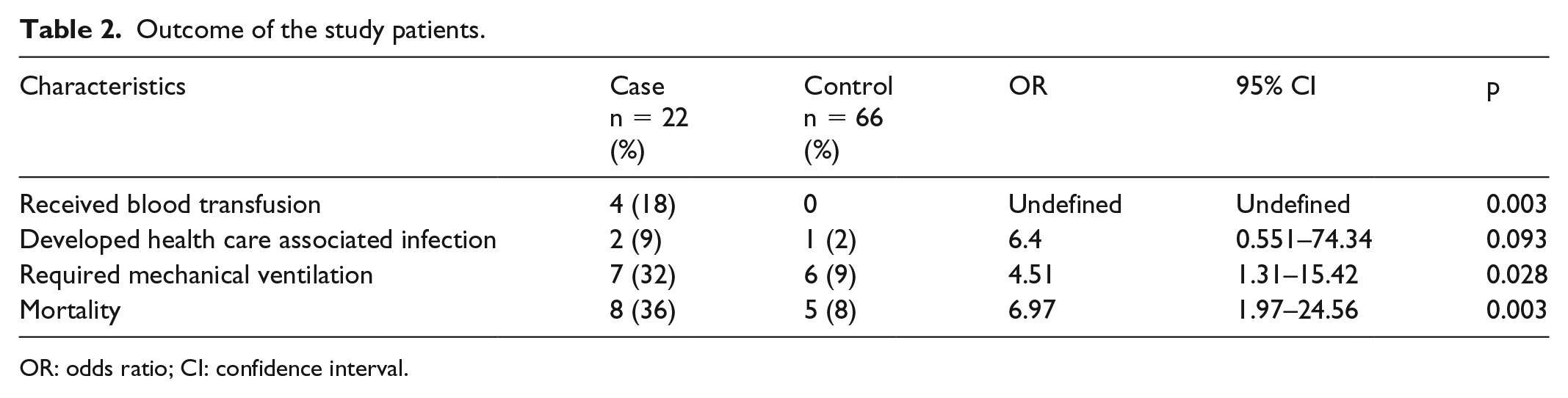
OR: odds ratio; CI: confidence interval.
Laboratory characteristics of study patients.

OR: odds ratio; CI: confidence interval.
Results of logistic regression analysis to explore the independent risk of cerebral edema in children with diarrhea.
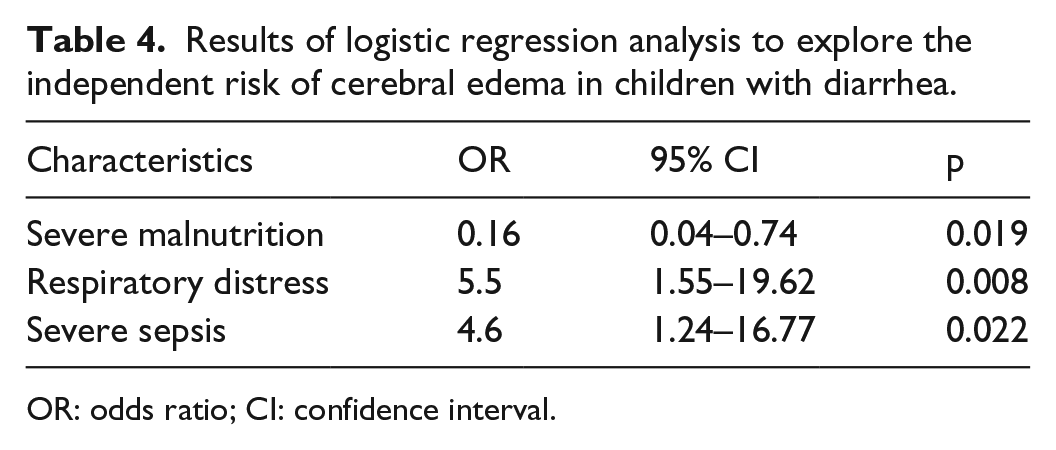
OR: odds ratio; CI: confidence interval.
No children in the control group developed papilledema. The cases additionally received either mannitol (16 patients) or 3% NaCl (6 patients).
Discussion
To our knowledge, this is the only study that evaluated the independently associated factors with cerebral edema in children suffering from diarrhea. However, we identified only 22 cases of cerebral edema. As blurring of the optic disk is the late sign of cerebral edema, we might miss a number of cases of cerebral edema among the children who had convulsions and even among the controls.
Our observation of an independent association of cerebral edema with respiratory distress and sepsis is important for the clinicians in developing countries, especially in resource-limited settings. The presence of these features in children who present with a convulsion in a critical care medicine ward may prompt our clinicians to early identification and prompt treatment in order to reduce mortality in these children. Previous studies also revealed the independent association of severe respiratory distress followed by hypoxemic respiratory failure with cerebral edema 19 and diabetic ketoacidosis–related cerebral edema. 20 A number of previous studies also showed that severe sepsis and its cascades are associated with cerebral edema. 21
We treated the study children with cerebral edema either with mannitol or 3% NaCl. Being an osmotic agent, mannitol reduces blood viscosity and reduces CSF (cerebrospinal fluid) volume by drawing water out of the brain. 1 There is also the role of the hypertonic solution in the management of cerebral edema. Having a higher osmotic reflection coefficient, it improves cerebral perfusion of ischemic areas by reducing edema of vascular endothelial cell and red blood cell. So 3% of NaCl was also used in few patients. 22
Our observation of higher mortality among the children having cerebral edema compared to those without cerebral edema was understandable. Children with cerebral edema in our study were found to be independently associated with severe sepsis and respiratory distress, both of whom are associated with high mortality.23,24 Moreover, children in our study with cerebral edema more often required mechanical ventilation and received a blood transfusion, and both of these associated factors may be responsible for the higher deaths in our study children with cerebral edema.25,26 However, mortality rates in children suffering from cerebral edema in other studies differ according to its causes, the most prominent reason being diabetic ketoacidosis, 6 neonatal seizure, 27 and fulminant hepatic failure. 28
The important observation of the study is that children with severe malnutrition were found to be protective in developing cerebral edema. We do not have any ready explanation for this pioneer observation. There is an alteration of production and activation of cytokines due to impairment of lymphocytes, resulting in a reduction of cytokines in malnourished children. This impairs adequate immunological function in malnourished children29,30 and may lead to a reduced inflammatory response in the brain of the children with severe malnutrition. That may have an impact in lesser observation of cerebral edema in such children.
Another important observation of this study is that the rapid drop in serum sodium did not have any impact on developing cerebral edema in our study children. This observation is consistent with the recent study managing hypernatremia diarrheal children in Bangladesh. 24 However, a number of previous studies had evidence that rapid reduction in the serum sodium concentration can cause cerebral edema. 31
Limitations of the study
The limitation of our study is the retrospective nature of the study, which involves a small number of samples and limited the adequate power of the study and subsequently limited the generalizability of the study results. Another limitation is the clinical diagnosis of cerebral edema relying on fundoscopic examination; thus, a few cases may be underdiagnosed or may fall in the control group.
Conclusion and significance
Cerebral edema in diarrheal children was associated with higher mortality compared to those without cerebral edema. Diarrheal children under 5 years of age having convulsion who also have severe sepsis and respiratory distress are at increased risk of having cerebral edema and those who have severe malnutrition are less likely to have cerebral edema. Identification of these simple clinical characteristics may help in the early case detection and management of cerebral edema and therefore help in reducing deaths in such children, especially in resource-poor settings. However, further research with prospective design and larger sample involving brain imaging in diarrheal children is warranted to substantiate our observation.
Footnotes
Acknowledgements
We gratefully acknowledge the donors for their support and commitment to International Centre for Diarrhoeal Disease Research, Bangladesh’s (icddr,b) research efforts. We would like to express our sincere thanks to all clinical fellows, nurses, members of the feeding team, and cleaners of the hospital for their invaluable support and contribution to patient care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was waived by Institutional Review Board (IRB) of International Centre for Diarrhoeal Disease Research, Bangladesh (icddr, b), consisting of Research Review Committee (RRC) and Ethical Review Committee (ERC), because this retrospective study did not involve any interview with the caregivers. Data used for this study were initially obtained for patient management at Dhaka Hospital of icddr,b. However, written approval was taken from the IRB.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) and its donors, which provide unrestricted support to the institution for its operations and research. Current donors providing unrestricted support include Government of the People’s Republic of Bangladesh, Global Affairs Canada (GAC), Swedish International Development Cooperation Agency (Sida), and the Department for International Development, UK (UKaid).
Informed consent
Informed consent was not sought for the present study because it was a retrospective study, and for this study caregivers were not asked for an interview.