
Abstract
A 68-year-old man was scheduled to undergo percutaneous coronary intervention for in-stent total occlusion of the severely tortuous right coronary artery. Intravascular ultrasound revealed heavy in-stent calcification. Lesion atherectomy was required; however, severe proximal vessel tortuosity was detected. We introduced a 7-Fr guide-extension catheter beyond the severely tortuous part and performed rotational atherectomy with a 1.5 mm burr. However, the balloon could not expand; therefore, we changed to an orbital atherectomy system. Subsequently, the balloon successfully expanded, and intravascular ultrasound revealed an enlarged lumen. Severe proximal vessel tortuosity limits the use of atherectomy devices; however, a guide-extension catheter delivers the atherectomy device beyond the tortuosity. The delivery of the orbital atherectomy system inside the guide-extension catheter is easy due to its low profile; the debulking effect increases with the number of passes and rotational speed. This strategy is a useful option for treating severe calcified lesions with proximal vessel tortuosity.
Keywords
Introduction
Severely calcified coronary lesions are challenging to treat with percutaneous coronary intervention (PCI). 1 Although atherectomy devices are used to treat calcified lesions, delivery of the atherectomy devices is difficult in severely tortuous vessels. Diamondback 360® Coronary Orbital Atherectomy System (OAS) (Cardiovascular Systems Inc.) has only one crown of a small size (1.25 mm), so it is easy to deliver and has a dual mechanism of action, which is different from that of rotational atherectomy (RA) (Rotalink PlusTM, Boston Scientific, Natic, MA, USA). 2 We present a case wherein a severe calcified coronary lesion with proximal vessel tortuosity was successfully treated using OAS with the backup of a guide-extension (GE) catheter.
Case
A 68-year-old man underwent PCI for an in-stent total occlusion of a severe tortuous right coronary artery (RCA) (Figure 1(a) and (b)). We performed PCI via the right femoral artery using a 7-Fr guiding catheter (AL 1.0, Launcher, Medtronic, USA). The previous stent was implanted 3 years prior; severe tortuosity had been observed in the middle part. We performed the knuckle wire technique using a 0.014-in guide wire (Fielder FC, ASAHI INTECC, Japan) with microcatheter backup. After the guide wire successfully crossed the lesion, we performed balloon angioplasty using a 3.0 mm balloon throughout the lesion; however, the distal part of the RCA could not expand sufficiently after balloon dilatation (Figure 1(c)). Intravascular ultrasound (IVUS) revealed heavy calcification inside the stent (Figure 1(d)); therefore, we decided to use an atherectomy device. We introduced a 7-Fr GE catheter (GuidezillerTM, Boston Scientific, Natick, MA, USA) beyond the proximal vessel tortuosity and performed RA, initially using a 1.5 mm burr (Figure 2(a)). The selected burr speed was 220,00 r/min, and we performed seven passes of RA. However, the 3.5 mm cutting balloon could not expand sufficiently after that (Figure 2(b)). Therefore, we switched to using the OAS with low speed (50,000 r/min), and we performed eight passes of OAS at the speed of 1 mm/s (Figure 2(c)); after balloon dilatation, IVUS revealed an enlarged lumen area (Figure 2(d)). Final angiography showed no residual stenosis (Figure 2(e)).
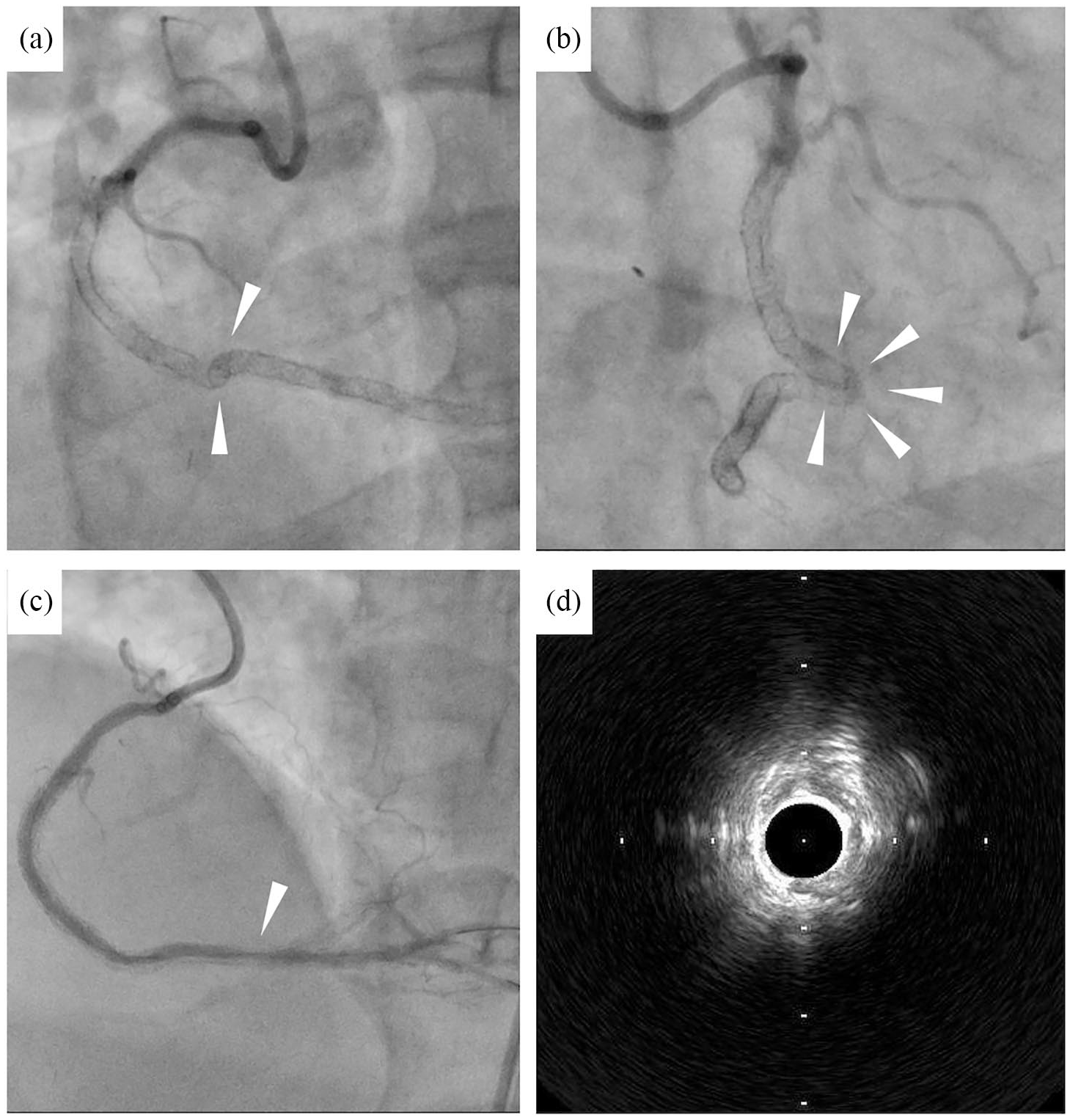
(a) Left anterior oblique view (45°), severely tortuous vessel (arrowhead), (b) right anterior oblique view (30°), severely tortuous vessel (arrowhead), (c) insufficient balloon expansion (arrowhead), and (d) IVUS findings. IVUS showed that the entire circumference inside the stent was heavily calcified. The lumen was extremely small even after balloon angioplasty using a 3.0 mm balloon. Debulking of the calcification was needed for enough balloon dilatation.

(a) RA with a 1.5 mm burr through the GE catheter, (b) Insufficient balloon expansion after RA (arrowhead), (c) OAS through the GE catheter, (d) IVUS findings after OAS, and (e) final angiography.
Discussion
RA is difficult to use for calcified lesions with proximal vessel tortuosity due to the risk of the device getting trapped or causing a vessel injury at the tortuous part of the vessel. 3 The GE catheter helps to improve the backup force and enables atherectomy devices to cross the lesion. 4 We consider that the GE catheter is also useful to safely deliver atherectomy devices beyond the proximal vessel tortuosity and perform lesion atherectomy. We used a 7-Fr GE catheter (GuidezillerTM) in the present case because its inner lumen is the largest compared to other types of commercially available 7-Fr GE catheters. 5 However, the maximum burr size of the RA deliverable into the 7-Fr GE catheter is 1.5 mm; thus, the ability to modify the lesion is limited. On the contrary, the profile of the OAS is 1.25 mm, 2 and it is easier to deliver into the 7-Fr GE catheter than RA. Furthermore, the lumen area increases according to the number of passes and rotational speed; 2 therefore, OAS is the ideal debulking device when additional debulking is needed, but increasing the burr size of the RA is impossible. In addition, we considered that one of the possible mechanisms to explain why OAS, but not RA, was successful in treating this heavily calcified in-stent restenosis was plaque modification of calcification behind the stent, although this could not be confirmed by IVUS. The ORBIT II trial demonstrated that after use of the OAS, the freedom from 30-day major adverse cardiac events was 89.6%, and residual stenosis <50% post-stent without in-hospital major adverse cardiac events was 88.9%. 6 Although further research is needed to confirm the safety and efficacy of OAS for very complicated calcified coronary lesions, it may be a promising device for severe calcified coronary lesions with proximal vessel tortuosity under the backup of the GE catheter.
Conclusion
We present a case of severe tortuous calcified coronary lesion that was successfully treated by using OAS with the GE catheter as a backup. Although this technique is off-label, it may be a useful option to treat severe tortuous calcified coronary lesions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.