
Abstract
This report describes the case of a 45-year-old woman with Noonan syndrome who developed cubital tunnel syndrome secondary to hypoplasia of the humeral trochlea. Cubital tunnel syndrome, the second-most common peripheral compression neuropathy, is caused by compression of the ulnar nerve at the elbow. Noonan syndrome, an autosomal dominant multisystem disorder, is characterized by variable cognitive deficit and skeletal, ectodermal and hematologic anomalies. Results show three distinctive anatomical features such as (1) hypoplasia of the humeral trochlea and medial epicondyle, (2) absence of the medial intermuscular septum and (3) lack of Osborn’s ligament.
Keywords
Introduction
Cubital tunnel syndrome, a chronic disorder caused by entrapment of the ulnar nerve at the level of the elbow, is the second most common peripheral compression neuropathy after carpal tunnel syndrome. 1 Incidence ratios based on sample population, case definitions and diagnostic method are reportedly 0.08–8 per 1000 person-years.2–4 Depending on the etiology, this syndrome can be categorized into primary or secondary form. The primary form includes abnormalities such as luxation of the ulnar nerve and the presence of anconeus epitrochlearis muscle, which are predisposing factors. The secondary forms follow earlier trauma of the elbow joint, osteoarthritic changes with exostoses, unstable elbow joint, the occupied lesion as ganglion and so on. 1 Noonan and Ehmke first documented Noonan syndrome in 1963 as an autosomal-dominant multisystem disorder characterized by variable cognitive deficit and skeletal, ectodermal and hematologic anomalies.5–7 Various skeletal manifestations have been reported in patients with Noonan syndrome including pectus excavatum, cubitus valgus, scoliosis and vertebral anomalies. 8 This report, which is the first of a study examining cubital tunnel syndrome in the setting of Noonan syndrome, describes an unusual case of cubital tunnel syndrome in Noonan syndrome secondary to hypoplasia of the humeral trochlea.
Case report
A 45-year-old woman was referred to our hospital to evaluate a 3-year history of numbness in her left ring and little finger and the ulnar side of the hand, in addition to a 2-year history of gradually decreasing hand grip strength. She had congenital scoliosis, for which she had undergone spinal arthrodesis as a junior high school student (Figure 1). She had congenital camptodactyly of bilateral little fingers. She was a homemaker who had experienced no upper extremity trauma or surgery.

Anteroposterior radiographs of whole spine.
She was of short stature (136 cm height < third percentile, 37.0 kg weight) with typical facial dysmorphology: high-anterior hair line, widely spaced eyes, neck skin webbing and small chin. Physical examination revealed no cubitus varus or valgus deformity in the left elbow. Active elbow flexion was up to 150°. Passive extension loss was 30° with no instability. The range of forearm motion was 80° for pronation and 90° for supination. A Tinel test was positive proximal to the origin of the flexor carpi ulnaris (FCU). She showed decreased sensation to light touch on both the ring and the little finger. For application of the Semmes–Weinstein test, the dorsal side of the ring finger and the little finger was positive for purple monofilament (4.17 monofilament). The volar side of them was positive red monofilament (5.07 monofilament). Atrophy of the hypothenar muscle and of the dorsal interosseous muscles was found. Grip strength of the affected side was 8 kg (unaffected side: 13 kg). The key pinch strength of the affected side was 2.5 kg (unaffected side: 4.5 kg).
Anteroposterior radiographs of bilateral elbow joints demonstrated hypoplasia of the humeral trochlea and medial epicondyle and slight medial shift of olecranon. The carrying angle of bilateral elbows was 9° (Figure 2(a) and (b)).

(a) Right side and (b) Left side. Bilateral anterioposterior radiographs show hypoplasia of the humeral trochlea and medial epicondyle and slight medial shift of the olecranon. The carrying angles of both sides were 9°.
Ulnar nerve groove view of radiographs of bilateral elbows (Figure 3(a) and (b)) and axial view of computed tomography (CT) showed hypoplasia of the ulnar nerve groove (Figure 4).

(a and b) Ulnar nerve groove view of radiographs of bilateral elbows showed hypoplasia of the ulnar nerve groove.

Axial view of computed tomography showing hypoplasia of the ulnar nerve groove.
Ultrasonography (US) showed hypoplasia of the medial epicondyle and the ulnar nerve groove and ulnar nerve luxation to the anterior. It also showed enlargement of the cross-sectional area of ulnar nerve proximal to the origin of the FCU (Figure 5).
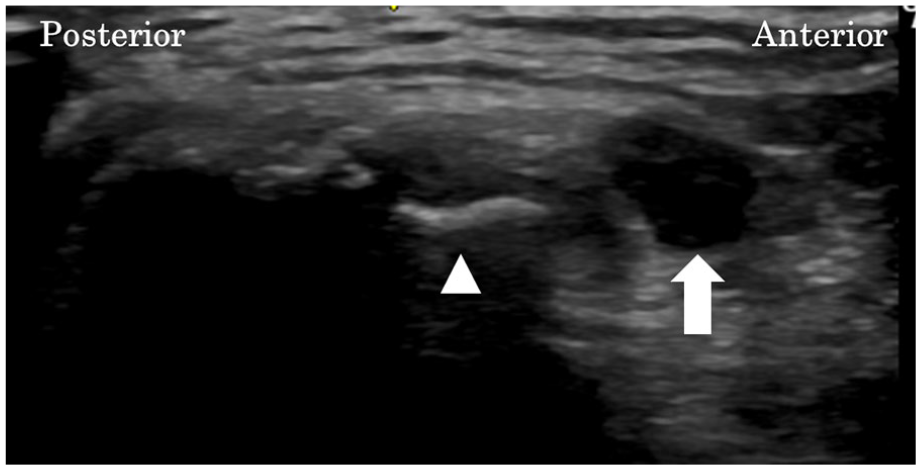
Axial view obtained using ultrasonography shows hypoplasia of the medial epicondyle and the ulnar nerve groove (arrowheads) and ulnar nerve luxation to anterior and enlargement of cross-sectional area of ulnar nerve proximal to the origin of the FCU (arrow).
Nerve conduction study results indicated that motor nerve conduction velocity of the ulnar nerve on the affected side was 41.8 m/s between the upper elbow and the wrist (52.6 m/s on the unaffected side). The sensory nerve conduction velocity on the affected side was 39.5 m/s between the upper elbow and the wrist (69.8 m/s on the unaffected side). Based on clinical and electrophysiological findings, we diagnosed her as having CubTS.
She was treated with open cubital tunnel release under general anaesthesia. A medial skin incision was made at the anterior of the hypoplasia of the medial epicondyle. Intermuscular septum of the upper arm and Osborn’s ligament was not found. The ulnar nerve was identified proximally, anterior at the upper arm. The ulnar nerve was compressed by the fibrous bundle, which was apparently harder and thicker than usual, over the FCU. Neuroedema of the ulnar nerve caused by compression was found at the proximal position of the fibrous bundle (Figure 6(a)). Decompression was performed by releasing the fibrous band and FCU fascia and deep flexor–pronator aponeurosis (Figure 6(b)). The ulnar nerve was covered by a pedunculated fat flap (Figure 6(c)). At the final follow-up, 6 months after the operation, application of the Semmes–Weinstein test, dorsal and side of ring and the little finger was positive for green monofilament (2.83 monofilament). The grip strength of the affected side was restored from 8 to 11 kg. The key pinch strength of the affected side was recovered from 2.5 to 3.0 kg. An electrophysiological study found recovery of the ulnar nerve function. The motor nerve conduction velocity was 66.0 m/s between the upper elbow and the wrist. The sensory nerve conduction velocity was 56.3 m/s.
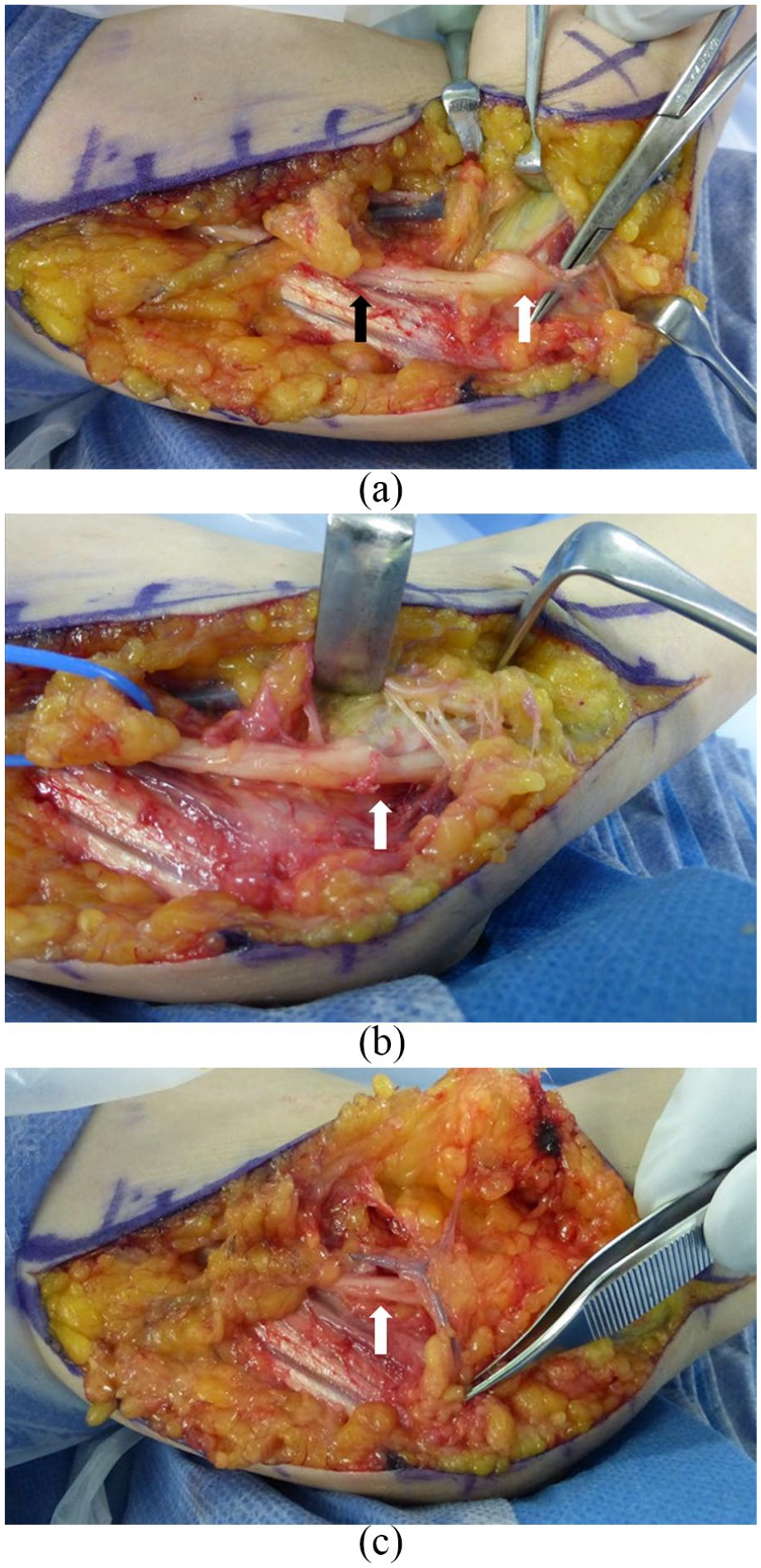
(a) Intermuscular septum of upper arm and Osborn’s ligament were absent. The ulnar nerve was identified proximally, anterior at the upper arm. The ulnar nerve was compressed by the fibrous bundle over the flexor carpi ulnaris (FCU) (arrow). (b) Decompression was performed by releasing the fibrous band and FCU fascia and deep flexor–pronator aponeurosis. Neuroedema of the ulnar nerve caused by compression was found at the proximal position of the fibrous bundle (arrow). (c) The ulnar nerve (arrow) was covered by a pedunculated fat flap.
Discussion
Results show three distinctive anatomical features in this patient with Noonan syndrome who had CubTS: (1) hypoplasia of the humeral trochlea and medial epicondyle, (2) the absence of medial intermuscular septum and (3) the absence of Osborn’s ligament.
First, hypoplasia of the humeral trochlea and medial epicondyle was noted. The olecranon was shifted slightly to the medial side. Earlier reports described cases of CubTS with hypoplasia of the humeral trochlea.9,10 Most reported cases had cubitus varus or valgus deformity and restriction of the range of motion during extension. Some had instability of the elbow joint and loosening and ballooning of the elbow joint capsule and the ganglion. Hypoplasia of the trochlea and the bone and soft tissue around the elbow joint can be expected to give rise to elbow joint instability and the ganglion that caused CubTS. 10 Our case had no alignment deformity or instability of the elbow joint and the ganglion around the elbow joint.
Second, the medial intermuscular septum was absent in the upper arm. The ulnar nerve coursed anterior to the medial head of the triceps and the epicondyle with intraoperative inspection. Two cases with CubTS have been reported for which the ulnar nerve was located anterior to the medial epicondyle. 11 In the two cases, medial intermuscular septum was found. However, the ulnar nerve, located proximally posterior to the intermuscular septum, penetrated the septum proximal to the medial epicondyle where the ulnar nerve was compressed and emerged anteriorly. Our case differed from two cases in terms of the anatomical variant type of the ulnar nerve. Because US can detect the ulnar nerve location and dynamic instability, 12 we performed preoperative US examination, which revealed the anterior location of the ulnar nerve. This information led us to perform electrophysiological tests, which yielded information that has helped to make the ulnar nerve decompression procedure safer.
Finally, obvious Osborn’s ligament was lacking. The fibrous band over the FCU that compressed the ulnar nerve was very extremely thick and firm. An earlier study elucidated anatomical variations of the distal cubital tunnel in 24 embalmed limbs from 13 cadavers: one (4.2%) of the 24 embalmed limbs had thick partial aponeurosis between the FCU and the medial epicondylar muscles. 13 In our case, the fibrous band was thick, with total aponeurosis.
These distinctive clinical features might result from pure chance in our case. Mutations that cause Noonan syndrome alter genes that encode proteins with roles in the Ras/mitogen-activated protein kinase (MAPK) pathway, leading to pathway dysregulation. 14 Wide expression and involvement of tyrosine-protein phosphatase non-receptor type (PTPN) 11 in multiple signal transduction pathways in cooperation with various molecules including growth factors, cytokines and hormone might produce the wide range of clinical findings associated with Noonan syndrome. 15 Given the etiology of Noonan syndrome, the skeletal deformity and soft tissue variant in our patient might be inferred as dysmorphic features related with Noonan syndrome. Based on our experience, attention must be devoted to rare anomalies, especially when performing cubital tunnel release in Noonan syndrome with CubTS.
Conclusion
This report describes a patient with Noonan syndrome who developed cubital tunnel syndrome. Specifically, this patient had hypoplasia of the humeral trochlea and medial epicondyle with no intermuscular septum and anterior location of the ulnar nerve at the elbow. Awareness of these anatomical variants is expected to raise confidence in proper treatment and surgical management to avoid ulnar nerve injury when treating this rare condition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.