
Abstract
We present the case of a 43-year-old boy who presented with progressive pain as a result of history of lateral avascular necrosis of the talus secondary to traumatic open ankle luxation 20 years ago. Conservative treatment (12-month period) prior to surgery failed. It consisted of physiokinetic treatment, insoles and analgesic medication. A diagnostic injection was used in the ankle (positive) and subtalar joint (negative) in order to recognize origin of pain. Hemilateral avascular necrosis of the talus is rare. There are no prior reported cases of the use of hemi-implants. This case highlights the potential use of a patient-specific three-dimensional printed Ti6Al4V prosthesis presented in a complex scenario.
Keywords
Introduction
Avascular necrosis (AVN) or osteonecrosis (ON) of the talus presents a treatment challenge to foot and ankle surgeons.1,2 Although ankle arthrodesis continues to be a valid procedure, it eliminates ankle motion and pseudarthrosis may happen.2–4 Reconstruction options that preserves motion has been described through a diversity of procedures counting core decompression,1,5,6 vascularized pedicle bone grafting from the cuboid, 7 vascularized cuneiform bone flap and autograft, 8 ankle cartilage allograft replacement,4,9–11 autograft bone cancellous grafting with/without tissue transfer 12 and three-dimensional (3D) printed titanium cages. 13 Also, in order to maintain mobility, some authors published their results using a total talar replacement such as alumina ceramic prosthesis, 14 stainless-steel talar body prosthesis 15 and nickel-plated cobalt implants. 16
Fixation procedures may include utilization of fibula for tibiotalocalcaneal arthrodesis,17,18 tibiocalcaneal arthrodesis with a porous tantalum spacer 19 and hindfoot fusion. 20
The 3D printing – also called additive manufacturing – is the procedure of designing a preordained item or article via correct placement of materials in a layer-by-layer pattern. Additive manufacturing can build infinite structures with a multiplicity of materials, including plastics, metals, and living cells if necessary.21,22
This case report describes successful and rewarding reconstruction and consequent limb reconstruction procedure through the utilization of a patient-specific 3D printed Ti6Al4V ELI PER ASTM F3001 hemi-prosthesis to change a hemilateral AVN, thus preserving ankle joint.
Case report
Written informed consent was obtained from the patient for their anonymized information to be published in this article. Our institution does not require ethical approval for reporting individual cases. No permission was needed to reproduce any figures in this case report. A 43-year-old male patient presented with a talar AVN associated with progressive pain as a result of a traumatic open ankle dislocation 20 years earlier. The wound was laterally based and moderately contaminated. The patient initially underwent deep debridement and continuous irrigation of the open wound. Finally, he was stabilized with plaster and completed treatment with intravenous antibiotic for 2 weeks. The patient presented an AVN Irwin grade I 4 (Chart 1): segmental articular deficit isolated to either a talar portion; subtype B: AVN deep to the articular segment (Figures 1 and 2). A percutaneous bone biopsy was made in order to confirm the AVN diagnosis (Figure 3). Conservative treatment (12-month period) prior to surgery failed. It consisted of physiokinetic treatment, insoles, and analgesic medication. A diagnostic injection was done in the ankle (Result positive 3/3) and subtalar joint (Result positive 2/3) to recognize origin of pain.

(a) AP and (b) lateral view showing lateral signs of AVN. (c) Varus hindfoot.
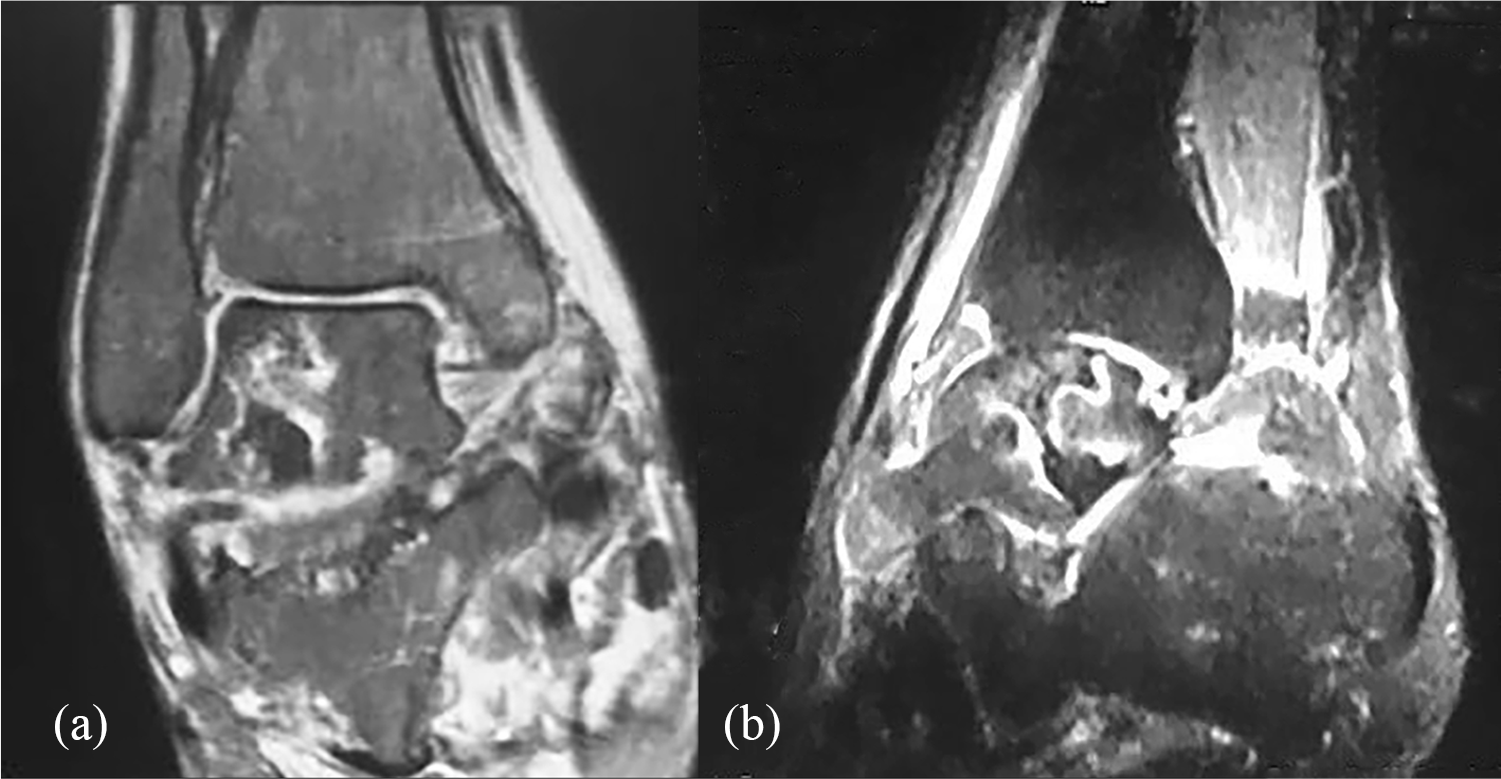
(a) Osteonecrosis of the talus on a T2-weighted sagittal MRI slice and (b) 50% of lateral talus was compromised.

(a) AP and (b) lateral view. Radioscopic-guided bone biopsy.
The use of patient-specific 3D printed Ti6Al4V ELI PER ASTM F3001 prosthesis with standard screws was deliberated with the patient. A computed tomography (CT) scan slices of 1 mm in all planes of the left ankle were collected and sent to medical application for processing and producing the implant. The manufacturer was Biotrom SA (Argentina); 3D printing vendor: Protolabs (Munich, Germany). The cost of the prosthesis was US$2498. The information was saved into a software (Mimics 11; Materialize®, Belgium) that allowed for 3D handling of the bones and articulations (Figure 4).

(a) Patient-specific cutting guide, (b) medial view of the implant showing internal structure, (c) posterior view of the implant showing medial pegs and screws and (d) final position implant.
Then, fibular and tibial plafond osteotomy was made to allow correct visualization (not done to correct ankle malalignment) of the lateral region of the talus. When lateral portion of the talus was resected, it showed macroscopic signs of AVN (Figure 5). The Ti6Al4V prosthesis was implanted with a matching less than 1 mm (Figures 6 and 7) and subtalar arthrodesis (evident subtalar chondral lesion was seen under direct vision) was added to correct varus hindfoot.

Macroscopic signs of hemi talar AVN.

(a) Lateral and (b) medial view of the implant showing mirror-polished articular surface and combined solid-lattice internal structure.

(a–d) Tibial oblique plafondplasty, resection of hemilateral talus, test prosthesis placement.
Postoperatively, the patient continued non-weightbearing with a plaster for 8 weeks followed by 2 weeks of controlled weightbearing in a walker boot. He then changed to full weightbearing for 2 weeks. Weightbearing was allowed prior to full CT consolidation. By 4 months, CT showed complete bone integration. X-rays and CT scan showed successful bone integration (Figure 8).

(a) AP and (b) lateral view showing the patient-specific 3D-printed hemi talar prostheses. (c) Axial CT scan osteointegration.
At final follow-up (18 months), the patient showed improvement in different scores: foot and ankle ability measure (FAAM) activities of daily living (AVD) 23 improved as 22.62 points (range: 38.09–60.71), FAMM sports enhanced as 35.71 points (range: 28.57–64.28), and the visual analogue scale (VAS) improved 6 points (range: 9–3).
Discussion
Treatment of AVN of talus has proven problematic for orthopaedic surgeons. According to some authors, a lengthy period of non-surgical treatment, including non-weightbearing combined with extracorporeal shock wave therapy (ESWT), followed by surgical treatment may be the best option.1,5 Gross et al. recommend – weak evidence – core decompression or bone grafting in patients with Ficat 24 grades I to III, and arthrodesis may become an excellent revision procedure. 1 According to some authors, core decompression continues to be a valid treatment for AVN5,6 at initial stages.
Although autografting may be a valid alternative for some authors, 25 it has major inconveniences such as donor site morbidity and finite quantity, 12 besides the difficulty to reproduce the anatomical structure in the receptor region. In the case presented this option was not viable because of the size needed.
Allografts are also likely limited in size and are less osteogenic with higher risk of malunion/non-union. Also, they may carry the abstract risk of infection transmission.26,27 Moreover, allograft has showed delayed failure leading to structural deterioration and can be limited by the ability to accurately arrive to the ideal configuration for limb salvage surgery.26–28 According to other authors, factors not found to be statistically different between the success group and the failure group were the time from death of the donor to transplantation, the donor’s age, the thickness of the both (ankle joint) allografts, and the postoperativealignment.29,30 Innovation technology, such as 3D printing, may arrange many of the problems of total or hemi allograft transplant. 20
Although ankle arthrodesis continues to be the gold standard, 3 implicit long-term difficulties are related to this alternative. Recently, some authors showed the results of the utilization of fibula for tibio-talo-calcaneal (TTC) fusion (union rate near 85%)14,18,31,32 and tibiocalcaneal arthrodesis with a porous tantalum spacer. 19 According to authors, this treatment offers a reliable option for complex salvage patients.
Fresh osteochondral allograft (OCA) can be used as a treatment option without excluding subsequent salvage surgeries such as repeat allograft transplantation, ankle arthrodesis or conversion to total ankle arthroplasty. 33 The OCA viability must be defined and supported by the role of immunosuppression, thus confirmed by new studies. 4 According to some authors, the high reoperation rate (2/17) and failure rate (5/17) must be taken into consideration 9 and represent an option for young patients with advanced damage to the ankle. Post-implantation limb alignment, optimal host-graft size matching and fit, and meticulous transplantation technique have been shown to enhance results. Other factors such as the optimal graft thickness, duration of post-implantation non-weightbearing status, and histocompatibility matching are not clear enough, and this continues to explain the high complication rate shown in previous clinical studies.11,34,35 In a recent systematic review, Johnson and Lee showed a 13%–42% incidence of complications associated with cartilage allograft implantation. Although it persists as a good treatment option, both authors showed that the overall quality of the existing studies is relatively insufficient and they recommend the design of randomized controlled trials (RCT) and prospective cohort studies in order to focus on better understanding indications and evolution of OCA. 10
Nunley and Hamid showed their results during the treatment of 13 patients with talar ON and managed with vascularized pedicle bone grafting from the cuboid. The two patients who went on revision surgery with a total ankle arthroplasty were considered to have treatment failure and did not complete a postoperative questionnaire as it was non-contributory to an as-treated analysis. 7
Recently, some authors published their results using different total talar replacement.14–16 The overall survival rate varies from 85% to 100%. Although this kind of procedures seems to be technically easy to perform, it does not allow too many options in case of revision surgery. The main indication would be a massive talar AVN, which was not the case presented.
The adaptability of 3D printing with regard to size, structure and biocompatible materials endures an interesting alternative for the treatment of segmental and cavitary defects in the distal tibia, ankle and foot as well. 21
Conclusion
The adaption of a patient-specific 3D printed Ti6Al4V prosthesis contributed to a successful reconstructive procedure in a case of substantial hemilateral talar bone loss. Additive manufacturing prosthesis can evade the complications and disadvantages of autografts, allografts and arthrodesis procedures. Moreover, costs of 3D printers as well as implantable metallic biomaterials are decreasing their cost due to the demand of the health market and thus increase accessibility. New studies are needed to asses delayed complications such as implant failure and stress shielding, among others.
Footnotes
Acknowledgements
All authors are equally conceived and designed the study, conducted research, provided research materials and collected and organized data, and analysed and interpreted data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.