
Abstract
Thymic carcinoma typically exhibits more clinically aggressive behavior and portends a worse prognosis as compared to thymoma. Venous thromboembolism is a significant cause of morbidity and mortality in oncologic patients. Traditionally, the standard-of-care management of cancer-associated venous thromboembolism has been therapeutic anticoagulation with low molecular weight heparins; however, with the advent of direct oral anticoagulants, there is an ongoing paradigm shift to transition to these novel agents in an attempt to attenuate cancer-associated venous thromboembolism events. We describe an exceedingly rare case of metastatic thymic carcinoma–associated right atrial thrombus with high-risk embolic features, which subsequently underwent near-complete dissolution with rivaroxaban after 3 months.
Introduction
Thymic carcinoma, derived from thymic epithelial cells, was initially identified by Shimosato et al. 1 in 1977. The interplay between thymoma and thymic carcinoma is still controversial with thymic carcinoma, typically exhibiting more clinically aggressive behavior and portending a worse prognosis. 2 Currently, there is a striking paucity of literature describing thymic carcinoma, which is considered to be relatively rare. 3 The incidence of thymic carcinoma has minimally increased from 0.03% to 0.07% from 2001 to 2015, respectively.4,5 The International Thymic Malignancies Interest Group (ITMIG) was established to increase collaborative efforts in the treatment of these tumors.6,7
Venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism, is a significant cause of morbidity and mortality in patients with cancer. 8 The cumulative relative risk ranges from 7-fold to as high as 28-fold in advanced neoplasia. 9 Traditionally, the standard-of-care management of cancer-associated VTE has been therapeutic anticoagulation with low molecular weight heparins (LMWHs); however, with the advent of direct oral anticoagulants (DOACs), there is an ongoing paradigm shift to these novel agents in an attempt to attenuate cancer-associated VTE events.10,11
We describe an exceedingly rare case of metastatic thymic carcinoma–associated right atrial thrombus with high-risk embolic features, which subsequently underwent near-complete dissolution with rivaroxaban after 3 months.
Case report
A 33-year-old Caribbean Black woman with no prior medical history presented to the emergency department with a 1-week history of fever, dyspnea, and generalized weakness. There was no reported history of night sweats. The patient experienced a 5-month duration of unintentional weight loss of approximately 20 pounds. The patient is a medical doctor; however, there was no exposure to patients with tuberculosis. The family history was significant for first-degree relatives with Hodgkin’s lymphoma and cholangiocarcinoma.
The patient was tachycardic at 130 beats per minute, tachypneic at 24 breaths per minute, saturating 92% on high flow nasal cannula. There was decreased air entry at the lower base of the left lung. A chest radiograph revealed complete opacification of the left lung zone (“white-out”) and a mediastinal mass. A 12-lead electrocardiogram demonstrated marked sinus tachycardia with secondary ST-T changes suggestive of “demand-ischemia.” An arterial blood gas sample was consistent with mixed respiratory and metabolic acidosis. The initial tentative diagnosis was suspected type 1 respiratory failure, likely multifactorial from the large pleural effusion in addition to suspected pulmonary embolism. A subsequent computed tomography “pulmonary embolism protocol” scan confirmed an anterior mediastinal mass (6.9 cm × 3.2 cm × 2.6 cm) with an associated large-sized left pleural effusion with perihilar lymphadenopathy and metastatic nodules. It also revealed a large right atrial thrombus (3.8 cm × 2.5 cm × 3.2 cm) without overt pulmonary emboli (see Figures 1 and 2).

Cardiac magnetic resonance imaging (cMRI) series: (a) Transverse section with left circle encapsulating pleural and lung metastases and center circle encapsulating the right atrial thrombus, (b) coronal section with white circle enveloping the large right atrial thrombus also demonstrating its heterogeneous appearance, (c) sagittal section with white circle enveloping the large right atrial thrombus again demonstrating its heterogeneous appearance, and (d) transverse section indicating the encircled pedunculated heterogeneous thrombus attached by a stalk from the right atrial free wall.

Transesophageal echocardiography (TEE) imaging series: (a–c) 90°, 120°, and 180° bicaval views, respectively, with a circle encapsulating the large right atrial thrombus, demonstrating a heterogeneous appearance; (d) 90° bicaval view demonstrating the dimensions of the right atrial thrombus before initiation of therapy.
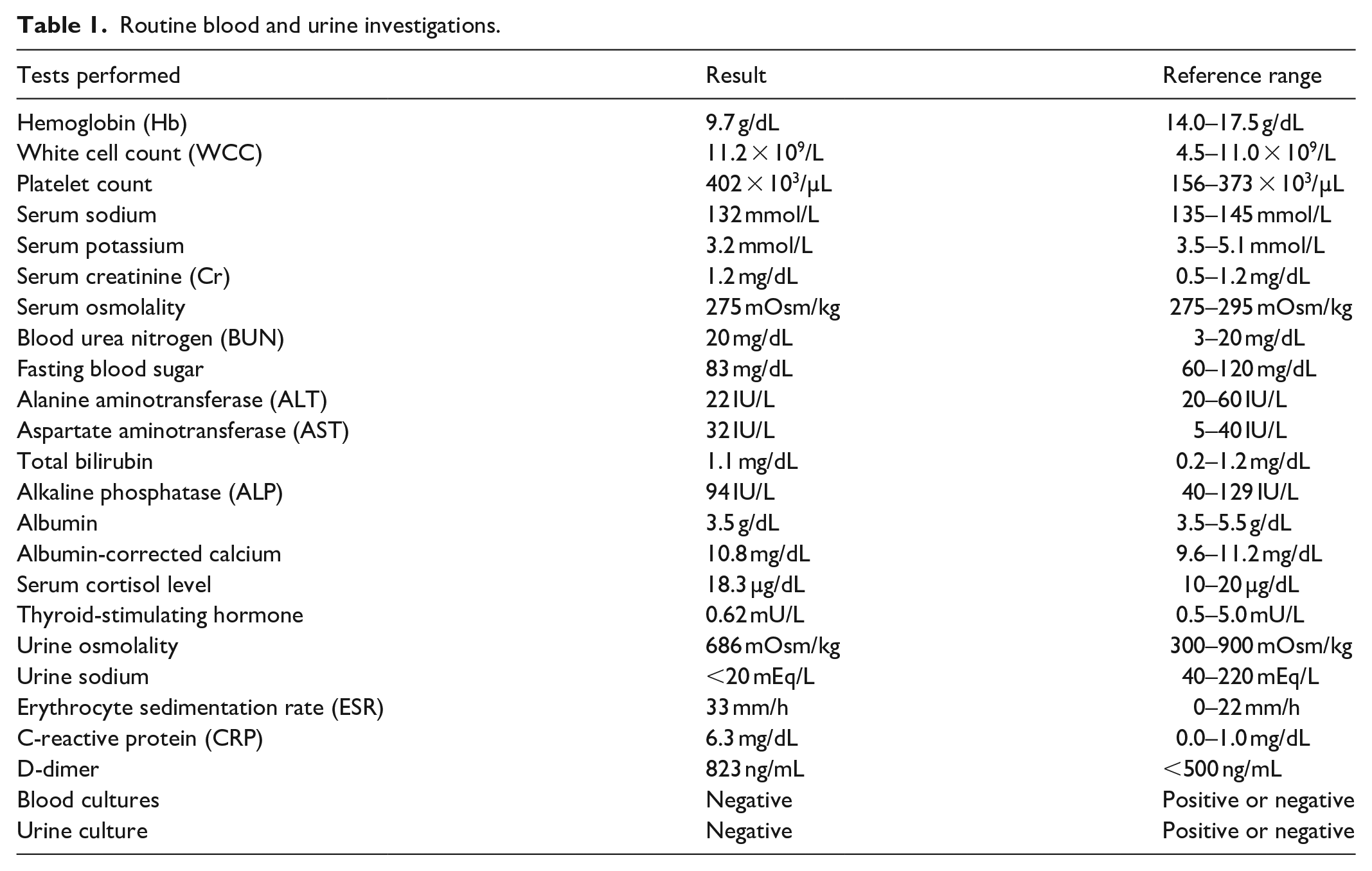
She was subsequently transferred to the intensive care unit, where she was stabilized and initiated upon therapeutic enoxaparin, low-dose aspirin, statin, ivabradine, and beta-blockade based on her high-risk Khorana score of 3. 12 Her routine blood investigations were reflective of dehydration (see Table 1). She also had 350 mL of serosanguinous fluid aspirated from her left lung via thoracentesis. Blood, urine, and pleural fluid cultures returned without bacterial growth. During her ensuing 2-week hospitalization, histopathology revealed features suggestive of thymic carcinoma. Neoadjuvant therapy comprising cisplatin, doxorubicin, vincristine, and cyclophosphamide (ADOC) was commenced. Surgical resection of the mass was performed where it was discovered that the tumor had metastasized to the left lung. Subsequent biopsies confirmed this diagnosis, and the neoplasia was staged as pT4 Nx M1. A transesophageal echocardiogram and cardiac MRI (magnetic resonance imaging) confirmed the presence of the right atrial thrombus (see Figures 1 and 2) with a preserved ejection fraction and no McConnell’s 13 sign.
Routine blood and urine investigations.
She was discharged on most of her inpatient regimen and also transitioned from enoxaparin to oral rivaroxaban at 15 mg twice daily for 3 weeks, thereafter at 20 mg daily for 3 months based on her intermediate-risk HAS-BLED score of 2. During this period, she underwent six cycles of gemcitabine and capecitabine chemotherapy, and a subsequent computed tomography scan 3 months later revealed near-complete right atrial thrombus dissolution (1.1 cm × 2.1 cm × 0.9 cm) (see Figure 3). She has a scheduled serial scan in 3 months with interim outpatient cardiology follow-up appointments.
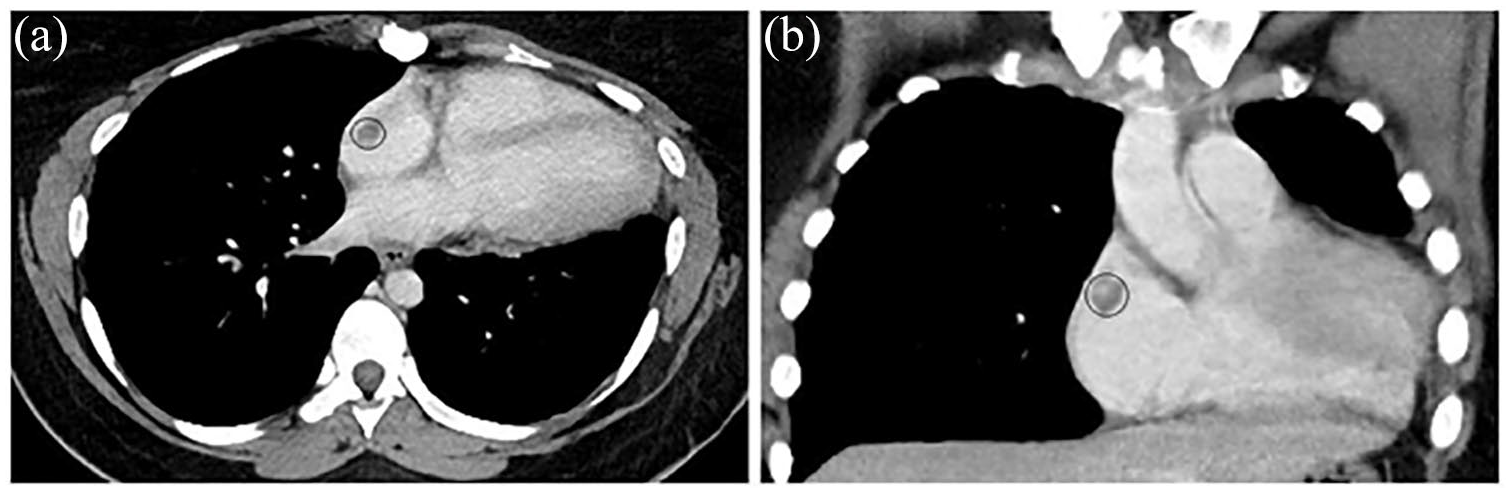
Computed tomography imaging (CT) series: (a) Transverse view demonstrating the encircled residual thrombus burden, which has been considerably attenuated by direct oral anticoagulation with rivaroxaban for 3 months and (b) sagittal view again demonstrating the residual thrombus burden.
Discussion
The pathophysiology of cancer-associated thrombosis (CAT) is complex and not fully elucidated. Several complex and interrelated mechanistic effects, including tumor cells, host cells, and the coagulation cascade results in a thrombophilic milieu. 14 Platelets and plasmatic factors also play a crucial role, culminating in the hypercoagulable state via proaggregatory and procoagulant pathways. Some of these involve the release of inflammatory and angiogenic cytokines, and direct interaction with host vasculature and erythrocytes through adhesion molecules. 15 Specific chemotherapeutic regimens and radiotherapy can also accentuate activation of the coagulation cascade. 16
There are three echocardiographic classifications for right heart thrombi (RiHTs), namely type A, which is the most common, serpiginous and has the highest risk of embolization; type B which is firmly attached to the chamber wall, ovoid shape; and finally, type C, which is rare and mimics cardiac myxomas. 17 Based on the cardiac magnetic resonance and transesophageal imaging sequences, our patient’s thrombus was most consistent with type B.
The Masaoka staging system is the most widely accepted system for staging and prognostication for thymic carcinoma. However, most patients are at an advanced stage at index presentation, and its clinical utility is dubious at best.18 –20 According to the current literature, the 5-year survival rate for thymic carcinoma is bordering 30%, and an optimal management algorithm has yet to be devised and hence, the rationale for ITMIG in an attempt to harmonize management strategies. 21
The tentative diagnosis on index presentation was pulmonary embolism as the D-dimer was abnormally elevated; however, the computed tomography scan only revealed the right atrial thrombus, fully acknowledging that this imaging modality has a sensitivity of approximately 85%–90% and a specificity between 88% and 95%. 22 RiHT is a rather uncommon finding and can be detected in approximately 4% of patients with pulmonary embolism. 23 The proper management of these patients is still a matter of debate. 24
VTE complicates the clinical course of almost one-third of all oncologic patients. 25 Anticoagulation in these patients is often a challenging dilemma as it poses an intricate juxtaposition between thromboembolic events and bleeding risk. LMWHs have long been the conventional mainstay pharmacotherapy; however, they require subcutaneous administration, whereas, conversely, the DOACs possess preferable pharmacokinetic and pharmacodynamic profiles, such as oral administration, immediate onset of action, and short half-lives as demonstrated in the cardiovascular arena. Data are now emerging for the use of DOACs in the oncologic subpopulation from dedicated clinical trials. Two recent systematic reviews, including the SELECT-D trial and Hokusai VTE trials, demonstrated that DOACs are non-inferior to LMWH for the prevention of recurrent VTE, albeit with an increased bleeding signal.26 –29 Low-dose aspirin and statin can also be considered as they confer a marginally protective benefit in high-risk cancers presenting with VTE.30 –32
The patient was initiated upon rivaroxaban for a myriad of reasons, including local accessibility, track-record in the SELECT-D trial, and prior cardiovascular experience in left ventricular mural thrombus dissolution. 33 The recommended dosage was instituted in addition to low aspirin and statin therapy as the multidisciplinary team considered the patient to be an advanced oncologic patient, given the metastatic thymic carcinoma and Khorana score of 3 coupled with an intermediate risk of bleeding as per the HAS-BLED scoring system. When cancer is included as an individual covariate along with components of the HAS-BLED score, it was considered the strongest predictor of major and overall bleeding.34,35 The HAS-BLED score has good predictive validity for bleeding risks in patients with VTE, where a HAS-BLED score of ⩾4 indicated a clear delineation for those at high risk for major bleeding when comparing risk for major bleeding among cancer and non-cancer patients. In addition, the inclusion of cancer as an independent risk factor to bleeding risk merits consideration, possibly as part of the B criterion (“bleeding tendency or predisposition”) of the HAS-BLED score. 35
The thrombus burden was substantial; in addition to displaying some embolic features, we opted for a robust, individualized regimen with a 3-month interval imaging, which displayed a markedly attenuated residual thrombus. 36 In light of her intermediate-risk HAS-BLED score, we also added adjunctive high-intensity statin therapy in addition to aspirin in an attempt to mitigate recurrent VTEs, fully acknowledging that this may increase her bleeding risk.37 –39
Conclusion
Direct oral anticoagulation with rivaroxaban instead of conventional therapy with LMWH represents an evolving pharmacotherapeutic alternative for right atrial thrombus dissolution in advanced oncologic patients. Presently, there is a paradigm shift, where individualized antithrombotic regimens with this novel class are being adopted due to their key advantageous characteristics. Furthermore, there are several emerging and ongoing studies that are assessing the clinical safety and efficacy of these agents in CAT.
Footnotes
Author contributions
C.N., J.K., R.S., V.S., S.P., K.R., and N.A.S. all contributed equally in writing the manuscript. All authors read and approved the final manuscript.
Data sharing statement
All available data can be obtained by contacting the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.