
Abstract
Background:
Hyperosmolar hyperglycemic state is a life-threatening endocrine disorder that most commonly affects adults with type 2 diabetes mellitus. The condition results from an osmotic diuresis-induced loss of water exceeding that of sodium. Altered mental status, hypernatremia and hyperglycemia are characteristic features at presentation. Abnormal electroencephalogram findings have been reported. Successful therapy requires judicious fluid replacement and close monitoring.
Case:
A 78-year-old Hispanic female with a significant past medical history of type 2 diabetes mellitus was admitted with altered mental status, severe hypernatremia and hyperglycemia. She was diagnosed with hyperosmolar hyperglycemic state, and fluid therapy was started. A continuous electroencephalogram revealed left frontocentral and temporal periodic lateralized epileptiform discharges that resolved as her hypernatremia and dehydration were treated. She survived and was discharged after 1 week of treatment.
Conclusion:
Abnormal electroencephalogram findings consistent with nonconvulsive seizure activity may be temporary and reversible and do not suggest a poor prognosis in an elderly patient suffering from hyperosmolar hyperglycemic state and altered mental status.
Keywords
Introduction
Hyperosmolar hyperglycemic state (HHS) is a life-threatening endocrine disorder that most commonly affects adults with type 2 diabetes mellitus.1,2 It is characterized by severe dehydration with hypernatremia, marked hyperglycemia, variable degrees of neurologic impairment and mild or no ketosis. 3 A precipitating event can usually be identified in patients with HHS. Although infections are the leading cause in 57% of the cases, 4 other possible antecedent risk factors include the presence of coexisting diseases, medications, noncompliance with medications, undiagnosed diabetes and substance abuse. 5 The neurologic consequences of HHS typically occur in patients with an effective plasma osmolality (POsm) above 320–330 mOsm/kg 6 and range from headache and coma to bizarre manifestations including pseudo brain stem infarctions 7 and seizures. 8 We present a case of an advanced aged woman with HHS, profound hypernatremia, neurologic dysfunction and electroencephalogram (EEG) evidence of left frontocentral and temporal periodic lateralized epileptiform discharges (PLEDs). She had a resolution of the epileptiform EEG and complete clinical recovery to her pre-HHS state after vigorous intravenous therapy and close monitoring.
Case
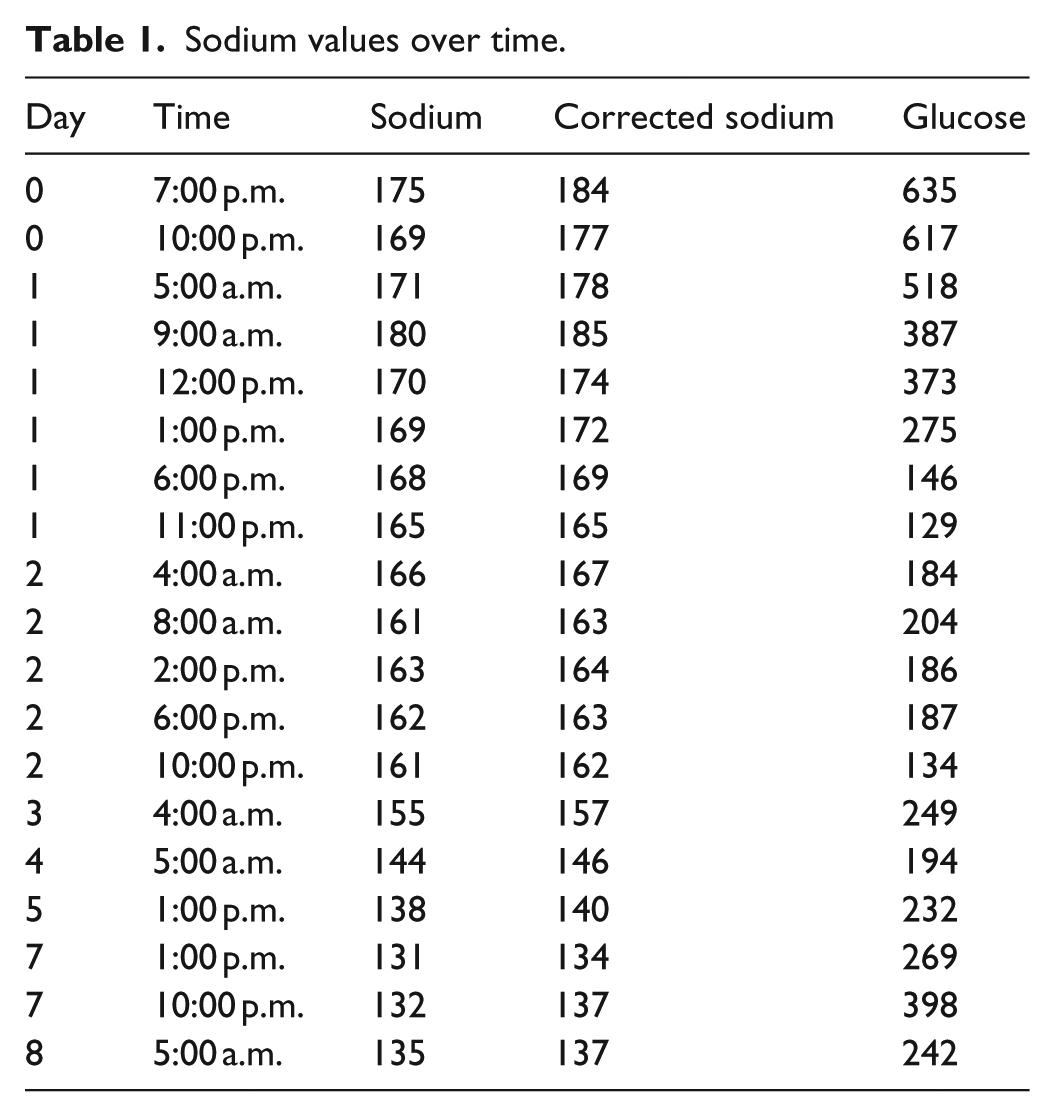
A 78-year-old Hispanic female with a significant past medical history of type 2 diabetes mellitus, hypertension and hypothyroidism presented with altered mental status. She was brought to the emergency department by her family members who assisted with history gathering. According to her family, the patient had a cough and worsening shortness of breath over 3 days prior to admission unrelieved by over-the-counter antihistamine and antitussive medications. The family did not know how long she had been diabetic or hypertensive. Nor could they list her medications. Upon presentation she was lethargic, had labored breathing and was lying in bed shaking. Her blood pressure was 142/67 mmHg in the supine position, heart rate 114 bpm, axillary temperature 36.7°C and she weighed 51.7 kg. On physical examination, she was ill-appearing, obtunded, not following verbal commands and with Glasgow coma scale of 9. She had decreased breath sounds over the left lung lower field. The examination of the heart, abdomen and extremities was normal. On neurological examination, she had hyperreflexia at the patellar and ankle joints, as well as stimulated bilateral clonus and positive Babinski sign. The screening blood tests performed upon her admission to the hospital were consistent with severe HHS. Her initial laboratory findings revealed glucose 635 mg/dL (normal: 70–105), sodium 175 mEq/L (corrected Na: 188 mEq/L) (normal: 135–145 mEq/L), blood urea nitrogen (BUN) 76 mg/dL (normal: 6–20 mg/dL), creatinine 1.61 mg/dL (normal: 0.5–1.2 mg/dL) with a serum osmolality 410 mOsm/kg (normal: 280–300 mOsm/kg). Her urine ketones were negative. On arterial blood gas her pH was 7.43, and HCO3 29 mEq/L (normal: 22–29). Her initial hemoglobin (Hgb) was 16.8 g/dL, white blood cell count (WBC) 18.3 × 103/µL and platelet count 194 × 103/µL. The initial chest X-ray and noncontrast head computed tomogram (CT) were negative with the head CT showing only mild diffuse cortical atrophy, proportional to the size of the ventricular system. The calculated water deficit on admission was about 5.5 L. In the emergency department, aggressive fluid resuscitation for volume replacement was started using normal saline (NS), which initially caused worsening in sodium values to 180 mEq/L (corrected Na: 193 mEq/L). After 2 L of NS, WBC was 23.2 × 103/µL, Hgb was 15.1 g/dL, platelet was 160 × 103/µL and her HCO3 was within normal limits in our laboratory at 28 HCO3 mEq/L. She was admitted to the intensive care unit (ICU), and nephrology was consulted. She was started on 0.45% NS and subsequently switched to 5% dextrose in water. The sodium began to trend down, while maintaining a mean steady decrease of 6 mEq/L of sodium daily, resulting in desired sodium range within 5 days (Table 1). An insulin drip was placed to control the severe hyperglycemia, which resolved steadily over the first 48 h. The insulin drip was discontinued, and insulin glargine with correctional insulin lispro was started. An abdominal pelvic CT was negative. Due to her neurological findings, a continuous EEG (cEEG) was ordered, which showed left frontocentral and temporal PLEDs on day 1. By day 2, the cEEG showed only abnormal slowing without epileptiform discharges. During the hospitalization, a nasogastric tube was placed and tube feeds were started due to her poor mentation. Her kidney function improved and returned to baseline. She was also found to have a left lower lobe infiltrate and was treated for community acquired pneumonia. She was initially treated with ceftriaxone and azithromycin; however, over the hospital course she clinically improved and was switched over to oral cephalexin to finish the course. Her mental status improved and returned back to baseline. In order to prevent potential aspiration, she underwent a successful swallow study with modified barium and was started on regular diabetic diet. She stayed in the hospital for 7 days and was diagnosed with severe hypernatremia secondary to osmotic diuresis and dehydration from HHS. Her hemoglobin A1c was found to be 9.9%, and upon discharge, she was placed on metformin, insulin glargine and insulin lispro sliding scale. Due to her decline in functional status and deconditioning, she was discharged to a skilled nursing facility. She received diabetes teaching, which included lifestyle modifications, proper nutrition, insulin administration and glucose checks. Unfortunately, there was no good follow-up with the patient, because she returned to her home abroad.
Sodium values over time.
Discussion
This case is important for three reasons. First, she survived an endocrine emergency that has a mortality rate of up to 50%. 9 Second, she displayed unique epileptiform features on cEEG monitoring, and third, she had profound hypernatremia that carries a high mortality risk by itself and requires a monitored correction. With regard to the first important feature, HHS is diagnosed when the serum glucose is over 600 mg/dL and serum osmolarity is over 320 mOsm/L. It is a dangerous metabolically driven form of volume depletion, resulting in disruption of normal water homeostasis. Without judicious fluid replacement, glucose correction and electrolyte replacement, acute renal failure can result in multisystem failure and death. Elderly diabetics presenting with altered mental status and dehydration are likely candidates for HHS and should be evaluated and managed accordingly. Delayed management is as dangerous as overcorrection over a short period of time. The second important consideration of this case is the cEEG finding of PLEDs on admission. By hospital day 2, the cEEG displayed abnormal slowing but no epileptiform discharges, which suggests that a component of HHS was, in fact, the origin of the PLEDs. Over the days prior to her admission she became more volume depleted, her hyperosmolarity worsened and the central nervous system (CNS) deteriorated from the subsequent intracellular edema. It is also possible that her worsening level of consciousness was due to the epileptiform activity. The initial cEEG findings of her illness are notable and unique. That EEG confirmed the presence of temporal PLEDs consistent with nonconvulsive seizure activity. 10 While neurological manifestations are not unusual in HHS, the nonconvulsive seizure activity is unexpected. This EEG finding could represent the manifestation of her ongoing concurrent pathologies considering she was also suffering from profound hypernatremia and hyperglycemia. Or it could simply be that this finding is common but unreported in HHS because cEEG is not frequently employed, or the EEG findings are temporary and quickly reversible. Nonetheless, the notable element in this circumstance is that if similar EEG findings are noted in severe HHS in an elderly individual with HHS and type 2 diabetes, there can still be an expectation of a favorable prognosis and survival with proper fluid management and treatment and antiseizure medication or sedation may not be necessary initially. Of note is that other serious neurologic conditions have been reported as a consequence of HHS. In fact, focal seizures, particularly epilepsia partialis continua, may even be a presenting feature of severe HHS. 11 The third important element to the case was the extreme hypernatremia due to dehydration. In patients with HHS, hypernatremia is causally associated with a water deficit secondary to an osmotic diuresis-induced hypotonic loss, which results in a loss of water exceeding that of sodium. 12 In our patient, however, due to her reduced level of consciousness, her extreme hypernatremia was likely caused by a combination of reduced water intake together with the osmotic diuresis. HHS typically includes serious electrolyte disturbances with hypernatremia, but our patient’s serum sodium concentration is extreme. Goldszer and Coodley 13 reported the first case of natremia of over 200 mmol/L related to dehydration in a 74-year-old woman who also had altered mental state. Unfortunately, an EEG was not performed but intact survival was reported. Hypernatremia (serum sodium concentration ⩾145 mEq/L) is not an uncommon electrolyte disorder with increased morbidity and mortality, especially in the elderly and critically ill patients. Severe hypernatremia, however, is unusual and by itself is associated with a slow compensatory increase in brain osmolar content. In fact, hypernatremia rather than hyperglycemia may be the cause of mental alteration in HHS patients. 14 Our patient had been symptomatic for several days, suggesting a lengthy and progressively worsening electrolyte imbalance. Her condition likely deteriorated rapidly right before admission because of pneumonia. She was initially given NS in order to expand her extracellular volume. Then, we chose 0.45% NS infusions to slowly reduce the hypernatremia since a rapid correction can only be made if it can be documented that the hypernatremia has been present less than a few hours. 15 Many clinicians consider a cutoff time of 48 h. Less than 48 h implies that the disturbance is “acute,” while more than 48 h implies it is “chronic.” In summary, this case describes PLEDs on cEEG in the early phases of treatment for HHS with severe hypernatremia. This is an important observation since its presence appears to be unrelated to patient survival as long as it resolves quickly with fluid resuscitation.
Conclusion
In summary, the information in this case is new and helpful regarding the cEEG findings that occurred during cerebral edema from HHS. Importantly, nonconvulsive seizure activity may be temporary and managed simply by watchful monitoring rather than sedation and antiseizure medication. In addition, nonconvulsive seizure activity that resolves with treatment of the HHS should not be used as a prognostic factor.
Footnotes
Author contributions
All authors had access to the data and a role in writing the manuscript, no disclaimers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series. The Orlando Regional Medical Center (ORMC) Institutional Review Board (IRB) has reviewed the case [1355638-1] and concluded “DETERMINATION OF NOT RESEARCH.”
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.