
Abstract
We report the case of a patient with a giant right atrial myxoma that remained clinically silent until it almost completely obliterated the right atrium, prolapsed into the right ventricle and obstructed the tricuspid valve inflow. This case illustrates the importance of rapid surgical intervention in the setting of acute heart failure caused by tumor masses obliterating heart valves or cardiac chambers.
Introduction
Myxomas account for the vast majority of heart tumors in adults. About 75% originate in the left atrium. 1 The shares of right atrial myxomas reported vary from 10% or less2,3 to 15%–20%. 1 The growth of large myxomas is possible because they often remain clinically silent or cause only unspecific symptoms such as fatigue or palpitations until they have grown to a considerable size. Giant myxoma, however, is a rare finding, and reports of giant myxomas in the right cardiac chambers have remained limited to a few case studies over the past few decades.4,5
In spite of their benign nature and paucity of specific symptoms, right atrial myxomas may entail severe consequences. Accounts of embolization of thrombi or tumor fragments into the pulmonary vessels with subsequent pulmonary hypertension or of fulminant pulmonary embolism resulting from myxomas are not uncommon,6–8 even though clinically evident embolic events are considerably less frequent in patients with right than with left atrial myxoma. 1 Beyond this, right atrial myxomas may obstruct the tricuspid valve and lead to functional tricuspid stenosis during diastole, symptoms of right heart failure, syncope or even sudden death.
We report a rare case of giant right atrial myxoma that gave rise to acute life-threatening symptoms and required emergent surgery due to its size and location.
Case
A 63-year-old obese male presented with cardiovascular collapse after suffering from increasing fatigue, dyspnea (New York Heart Association (NYHA) III), chest tightness, intermittent dizziness and edema of the legs for some time. He presented with engorged neck veins, dyspnea and systolic pressure readings that alternated between >135 and <90 mmHg. His vital signs included normal temperature, a heart rate between 70 and 90 bpm with intermittent tachycardia and an oxygen saturation of 91% on oxygen therapy; electrocardiography (ECG) showed a right bundle branch block and transthoracic echocardiography revealed a right atrium almost completely obliterated by a large pedunculated mobile structure that prolapsed into the right ventricle and obstructed the tricuspid valve inflow. In a computed tomography (CT) ordered to exclude pulmonary embolism, the tumor measured 9 × 7 cm in its greatest dimensions (Figure 1(a)).
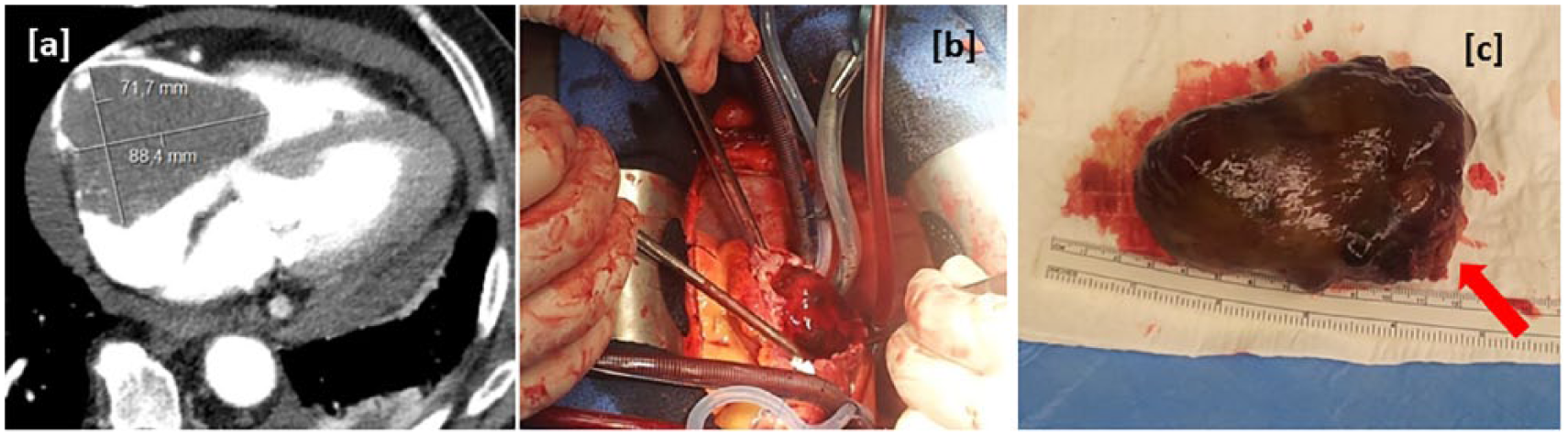
(a) CT showing large mass prolapsing from the right atrium into the right ventricle; (b) giant tumor protruding from the incision in the right atrium and (c) smooth-surfaced tumor removed as a whole from the right atrium. Arrow shows base of the tumor.
Immediately after the CT scan, the patient was transferred to our department for urgent surgery and underwent full sternotomy. The pericardium was found distended and filled with a moderate quantity of pericardial effusion. In the right atrium, which was prominent and appeared distended, a large mobile structure was palpable. Bicaval cardiopulmonary bypass (CPB) was established, taking care not to fragment or dislocate the tumor mass within the right atrium. A longitudinal right atriotomy incision performed on the normothermic beating heart revealed a large, solid tumor with a smooth, shiny surface (Figure 1(b)). Its base was approximately 2 cm in diameter and attached to the free right atrial wall.
The tumor was removed together with the portion of right atrial wall to which its base was attached (Figure 1(c)). Following this, and after inspection of the tricuspid valve for damage, the right atrium was closed.
Weaning from CPB, decannulation and chest closure were performed in standard fashion without complications. Intraoperative transesophageal echocardiography showed mild residual incompetence of the tricuspid valve. The patient, who had remained hemodynamically stable throughout the procedure, took a prolonged postoperative course aggravated by respiratory failure, prolonged mechanical ventilation, pneumonia and acute renal failure. He was discharged to a weaning facility after an intensive care unit (ICU) stay of 7 days. Follow-up at 6, 12 and 18 months showed a favorable outcome. The patient reported complete resolution of his symptoms, which was in keeping with the absence of echocardiographic findings indicating recurrence of the tumor.
Macroscopic inspection of the tumor showed a solid, but soft structure of a slightly gelatinous texture that measured 9.5 × 6 × 3.5 cm. The cut surface showed large yellowish-grayish myxoid areas and hemorrhagic portions, which is compatible with a diagnosis of myxoma. The pathological study confirmed the diagnosis of myxoma.
Discussion and conclusion
The diagnosis of myxoma in the setting of cardiovascular collapse is straightforward and does not require specific imaging efforts beyond echocardiography. Once a huge right atrial myxoma is found in a patient, however, the time to surgery should be short, which is illustrated by cases where delays in the removal of thrombus or tumors or complications occurring during diagnostic interventions resulted in a fatal outcome.9,10
In our case, the time to surgery was prolonged because CT was ordered to rule out pulmonary embolism. In spite of slow recovery, the outcome in our patient was favorable, which is in keeping with good outcomes of and low mortality after surgical resection of myxomas reported from larger collectives.3,11 Even though the delay between diagnosis and surgery caused by the additional CT was short, it must be acknowledged that the time to surgery is an essential factor and may exert considerable influence on the outcome.
We chose complete sternotomy even though minimally invasive or endoscopic excision of atrial myxomas with or without robotic assistance has been reported.12,13 Full sternotomy not only is the most straightforward approach in a hemodynamically compromised patient with an unusually large tumor but also improves visualization of the operating field, and facilitates dealing with any complications such as bleeding or need to address the tricuspid valve. Retrospectively, our decision to perform a full sternotomy also allowed us to inspect the tricuspid valve and evaluate the situation in terms of the need for cardioplegic arrest.
Conclusion
Giant right atrial myxoma is a rare cause of cardiovascular collapse but will be identified on routine echocardiography. Treatment consists of surgical resection and should not be delayed. Minimally invasive or endoscopic treatment with or without assistance of robotic therapy is possible though straightforward full sternotomy may be preferable in cases where the tumor has reached giant dimensions and gives rise to hemodynamic compromise.
Footnotes
Consent for publication
Written informed consent was obtained from the patient for his anonymized information to be published in this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.