
Abstract
Introduction:
The majority of the end-stage renal disease patients begin hemodialysis with the central tunneled catheter as a permanent or bridge vascular access. The procedure of central tunneled catheter insertion can be complicated by exit site bleeding, prolonged tunnel healing, and infection. The study aimed at evaluating whether the catheter exit site wound closing with a single-suture method is equally effective as the double suture method, which is most frequently applied. The assumption was that the single-suture method, which is less traumatizing for the skin, could offer an advantage for the patients with “paper” skin, that is, elderly, after long-term immunosuppressive treatment.
Methods:
Insertion of central tunneled catheter with antegrade tunnel formation was performed in 140 patients divided randomly into two groups of 70 patients using either single-suture method or double suture method.
Results:
Follow-up observations revealed a comparable number of early complications, that is, bleeding or exit site infection, in about 26% of the patients from both groups. No difference appeared in the catheter displacement, either. The percentage of patients with a prolonged central tunneled catheter exit site wound healing was not significantly lower in the single-suture method group: 5.8% versus 11.3%, p = 0.367. There was no impact of single-suture method versus double suture method on the central tunneled catheter long-term function and survival.
Conclusion:
The single-suture method of the central tunneled catheter exit closure is equal in efficacy to the double suture method. Its potential benefit for the patients with an increased risk of poor wound healing should be tested in further study.
Introduction
Many initiatives resulted from the publishing of the guidelines that strongly recommend, as a desired goal, the creating of arteriovenous fistula (AVF) in patients with end-stage renal disease (ESRD) before the hemodialysis starts.1–3 But the reality is that 84% of the US patients, 81% of Canadian ones, and 68% in Europe begin the therapy with a central venous catheter.4–6 European Renal Best Practice guidelines emphasize that central tunneled catheters (CTCs) should be preferred above the non-tunneled ones due to a lesser risk of infection. 1 Unfortunately, CTCs are also associated with significant morbidity and mortality. The rates of hospitalization because of vascular access-related complications, as well as general morbidity and mortality in patient population dialyzed using CTCs, significantly exceed those observed among individuals treated with AVFs.7,8 There are many published sources of detailed CTC implantation instructions.9–11 However, there is very scarce data regarding exit site creation. The majority of catheters are implanted with the antegrade method. 12 The CTC skin entering point preparation is an important part of the procedure. Proper incision, dissection, and finally suturing provide hemostasis, optimal conditions for wound healing, and reduce the risk of the CTC exit site and tunnel infection. This study aimed at comparing the potentially less skin-traumatizing single-suture method (SSM) of the CTC stabilizing with the dominating double suture method (DSM) with respect to the occurrence of early complications, particularly catheter displacement and prolonged would healing.
Material and methods
The retrospective, single-center study, based on patient record analysis was performed to compare two methods of the CTC exit site suturing as an important factor that influences the healing of postoperative wound, preventing from the early- as well as late-occurring complications which potentially affect the CTC line survival. From 2016 to 2019, there were 449 CTCs inserted in 373 adult patients in the Dialysis Unit at the Renal Department of Opole University Hospital. The study was not formally randomized according to prespecified criteria, but the patients were randomly qualified to a nephrologist performing a particular method of CTC exit site suturing depending on the on-call list.
The procedures were performed by two equally experienced nephrologists, and the patients were referred to each of them, randomly, according to the on-call list. Both of them had placed tunneled catheters for more than 15 years, around 100 catheters per year. The suture materials and the number of throws were the same during the study period. One hundred forty procedures performed in 140 patients using the SSM and the DSM were divided into two groups, each consisting of 70 patients included in the analysis (Figure 1). The patients were included in the study on condition they had a new CTC inserted as the only possible vascular access for hemodialysis, and they were waiting for AVF or arteriovenous graft (AVG) due to incomplete maturation or dysfunction, transferred from peritoneal dialysis for any cause or with kidney transplant failure. The exclusion criteria were when the CTC was not newly inserted but exchanged over guidewire or when tunneled lines or any subcutaneous devices were implanted previously on the side. Preoperatively, every patient was evaluated for the presence of a systemic infection and coagulopathy, and had the internal jugular veins scanned with ultrasonography to choose the optimal side for line insertion. The patients with the symptoms suggesting an active systemic infection—according to clinical symptoms, blood test results (i.e. C-reactive protein (CRP), procalcitonin (PCT), and white blood cell (WBC) levels), as well as microbiological tests—had an acute line for dialysis inserted and were diagnosed and treated until the infection was fought off. As it was mentioned above, hemostasis work out before implantation was performed The patients with the high risk of bleeding were identified when the level of treated platelets (PLTs) was ⩽50 × 109/L, activated partial thromboplastin time (APTT) was prolonged of >45 s, and international normalized ratio (INR) was over >2.0. Those patients were given PLT concentrate or the fresh frozen plasma (FFP) transfusion before the procedure, in accordance with the obligatory recommendations.13,14 All patients had jugular and subclavian veins scanned to find an optimal location for CTC implantation. The decision was also based on the prospective AVF or AVG location or the presence of other intravascular devices (i.e. Hickman’s catheters or implantable cardioverter defibrillator). All CTCs were inserted under local anesthesia with 1.0% or 2.0% lignocaine, with the US real-time guidance, using the antegrade method, in a designated procedure room, and the CTC exit site was secured with one of the methods under study. The SSM was performed in the manner described below. After the insertion of the CTC into the central vein, the line’s function was checked with a 20-mL syringe filled with normal saline solution. When the obtained blood flows were ineffective, the CTC position was corrected, until satisfactory CTC function was reached. The aim was to position the CTC cuff at the distance of 4 cm from the vein entering point, and 2 cm from the exit site. Thereafter, the CTC was fixed to the skin with two 2-0 or 3-0 nylon sutures. Then, a single suture of the same type was placed on the side of the line. At the moment of the suturing, the CTC body was pushed with the forceps to the other side of the needling point, in the caudal direction of the needling to prevent the catheter body puncturing (Figure 2). When hemostasis was achieved, the exit site was cleaned and prepared for the application of sterile dressing. The DSM was performed in the same way as SMM; however, the sutures were placed on both sides of the CTC exit site wound (Figure 3). Hemostasis inspection and wound preparation was also the same as for SSM. The patients with CTC inserted into jugular and subclavian veins had the chest X-ray performed a few hours after the implantation and the CTC dressing was inspected regularly over the next 24 h for the presence of bleeding. All complications were recorded and defined in the way described below. A major bleeding was defined when the patient presented systemic instability (i.e. tachycardia, hypotension), hemoglobin level decrease of more than 1 g/dL, and had a blood products transfusion. Other cases were treated as minor bleeding episodes. Following the CTC insertion, on every dialysis session, the dressing was exchanged and the CTC area was examined. The exit site and tunnel were inspected to estimate the healing process and the presence of any infection symptoms, that is, redness, swelling, or discharge. The exit site skin sutures were removed typically 14 days after the CTC insertion and the anchor sutures—after 21 days, with the check of the CTC cuff ingrowth. Prolonged healing of the exit site was defined as the lack of appropriate wound closure after 14 days. In that case, the sutures were left until the 21st day after insertion. Catheter dysfunction was defined as the inability to aspirate the locking solution from both lines or the achieved blood flow below 200 mL/min at the beginning of the hemodialysis session. Early CTC dysfunction was recognized when it occurred within the first week post-CTC insertion; the dysfunction was labeled as “late,” when it occurred after that period. The complete observation time included 30 days.
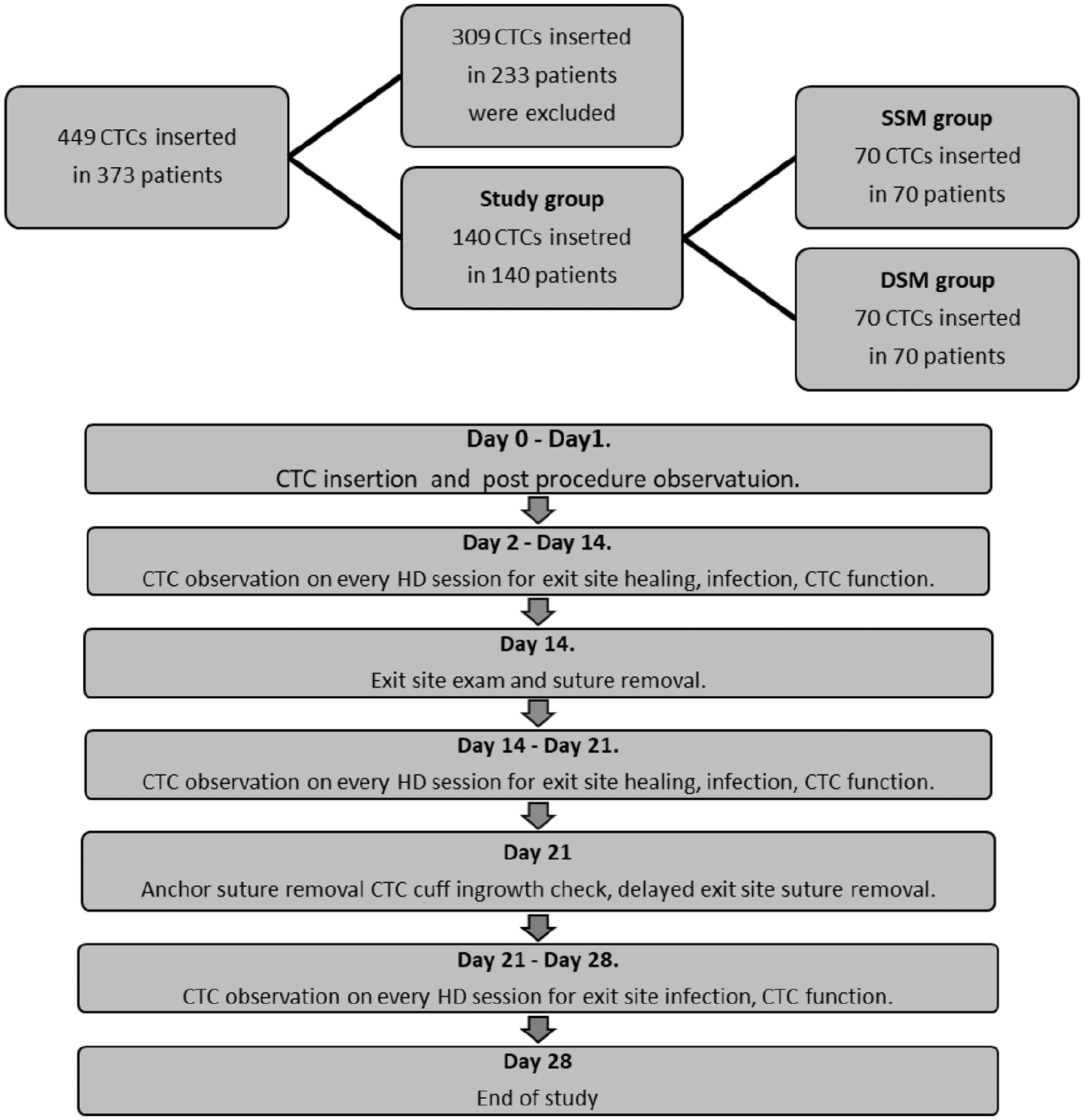
Study design.

Single-suture method (SSM)—exit site wound sutured on one side of the CTC line. Catheter stabilized with two anchor sutures to skin.

Double suture method (DSM)—exit site wound sutured on both sides of the CTC line. Catheter stabilized with two anchor sutures to skin.
The data were collected from the patients’ records, and only the complete ones were taken for evaluation. In the groups under study, the following types of CTC with comparable frequency were used: Arrow® Edge®, Arrow Cannon II Plus™, Arrow NextStep™, Bard® Hemosplit™, Bard Equistream™, Baxter® GamCath® HighFlow Dolphin Protect™, and Gambro® GamCath EverFlow™.
CTC insertions, a vascular access for hemodialysis, were routinely performed as a part life support therapy. Informed consent was obtained from all the individual patients before the procedure. Study based on patient record analysis was conducted in accordance with the ethical standards of the Declaration of Helsinki from 1964 and its later amendments and was approved by head of Bioethical Committee, Institute of Medical Sciences, Opole University (1.2021). The patients presented in the images illustrating the DSM and SSM have given their written consent for publishing the materials.
Statistical methods
Nominal variables are presented as n (% of total), continuous variables as mean (SD). Normality of distribution was verified with the use of the Shapiro–Wilk test, kurtosis and skewness values as well as on the basis of the visual assessment of histograms. The comparison of groups was conducted with the Fisher exact test, χ2 test, or independent samples Student’s t test, as appropriate. In addition, relative risk (RR) between groups with 95% confidence interval (CI) was calculated for complications frequency. Additional analysis included logistic regression, which was used to identify parameters predicting presence of complications after surgery. Separate models were prepared for each of complications: minor bleeding, major bleeding, prolonged healing, and infection, as well as for each of the groups separately. Only variables which were significantly different between patients with and without complications were included into the regression model as predictors. Since logistic regression was used, model coefficients were presented in log odds form (meaning that when the predictor increases by one unit, the outcome increases by log odds). To make interpretation easier, log odds were exponentiated into odds ratios (ORs), so that when the predictor increases per one unit, the expected change in the outcome is described in terms of % odds. The models were assessed with χ2 test, R2 Nagelkerke coefficient, and the Hosmer and Lemeshow goodness of fit (GOF) test. For the significant continuous predictors of complications, optimal cut-off points and receiver operating characteristic (ROC) curves were prepared with the Youden criterion. All the tests were two-tailed, and the differences were considered significant at the level of p < 0.05. The analyses were conducted in statistical software R, version 3.5.2 (http://cran.r-project.org).
Results
One hundred forty patients were included in the study, 70 patients in the DSM group and 70 patients in the SSM group. Demographic and clinical characteristics of the groups under study are presented in Table 1. The SSM group patients were significantly younger than those from the DSM group (60.89 ± 13.76 versus 65.67 ± 14.24 years; p = 0.031). CTC was implanted as bridge vascular access for hemodialysis in the patients waiting for AVF or AVG more often in the SSM group (62.8% versus 42.8%; p = 0.011), while CTC, AVF, or AVG dysfunction was an indication for the procedure more often in the DSM group (35.9% versus 55.8%; p = 0.011). There were no differences in the cause of ESRD, coagulation parameters, as well as anticoagulants, antiplatelet, and steroid use, between the groups under study.
Demographic and clinical characteristics of groups under study.

SSM: single-suture method; DSM: double suture method; CTC: central tunneled catheter; AVF: arteriovenous fistula; BMI: body mass index; ESKD: end-stage kidney disease; AVG: arteriovenous graft; PLT: platelet; INR: international normalized ratio; APTT: activated partial thromboplastin time.
Data presented as n (% of group) unless otherwise indicated. Groups compared with χ2 test or Fisher exact test for nominal variables and t test for continuous variables.
The groups under scrutiny did not differ with regard to the number of complications observed after the procedure: 18 (25.7%) versus 19 (27.1%) episodes; p = 0.887, in the SSM versus the DSM group, respectively. A detailed list and comparison are presented in Table 2. The most frequent was an exit site minor bleeding that occurred in equal number in both patient groups: nine episodes (12.8%). A comparable number of patients experienced the exit site major bleeding and required blood products transfusion in groups under study: 2 (2.8%) versus 3 (4.2%) episodes; p = 0.678, the SS versus the DS group, respectively. One patient (1.4%), from the SSM group, had the CTC removed due to excessive bleeding, not responding to medical and surgical interventions (i.e. blood product transfusions, desmopressin, extra sutures). A prolonged healing of the CTC exit site wound was more frequent, but not significantly, in the DSM group: 8 (11.4%) versus 4 (5.7%) episodes; p = 0.367, the DSM versus the SSM group, respectively. The exit site infection occurred in both groups with comparable frequency: 3 (4.2%) versus 4 (5.7%); p = 0.763, in the SSM versus the DSM group, respectively. One patient (1.4%), from the SSM group, had the CTC removed due to a CTC-related bloodstream infection diagnosed on 24th day of observation. There was no case of the CTC cuff non-maturation noted on 21st day when anchor sutures were removed and until the end of the study. No catheter displacement occurred in both groups. No differences were observed in the number of early CTC dysfunction cases (seven versus nine episodes; p > 0.9, the SSM versus the DSM group, respectively), as well as occurrence of late episodes (six and five episodes; p > 0.9, the SSM versus the DSM group, respectively) between both cohorts. Vascular access patency in all cases was successfully restored without necessity of CTC exchange. The first month of CTC survival was of 68/70 (97.1%) in the SSM and 70/70 (100%) in the DSM group. No significant relationship was confirmed between the occurrence of any insertion complication and the CTC exit site suturing methods under study (DSM and SSM).
Frequency of CTC removal complications between groups.

CTC: central tunneled catheter; SSM: single-suture method; DSM: double suture method; CI: confidence interval; RR: relative risk of complications presence in DS group versus SS group with 95% CI.
Data presented as n (% of group). Groups compared with χ2 test or Fisher exact test.
Further analysis of complication-predisposing factors was conducted (Table S3). Only among the SSM group patients, those who experienced a minor bleeding episode had significantly higher preprocedural APTT level than the same group individuals without the complication (36.56 ± 4.13 versus 31.78 ± 6.43 s; p = 0.035, the SSM patients with bleeding and without bleeding, respectively, MD = 4.78, 95% CI (0.35, 9.20) p = 0.035). No other factors influenced minor bleeding occurrence in both groups (Table S3).
In logistic regression, the APTT value as a variable predicted significantly occurrence of minor bleeding in SSM, increasing the risk by 11% when growing by one, exp β = 1.113, 95% CI (1.003, 1.256). Furthermore, a model was validated with χ2 test, which confirmed its significance (p = 0.043); however, an R2 Nagelkerke coefficient was at a small level (11%). In addition, it was assessed with the Hosmer and Lemeshow GOF test (p = 0.782), which confirmed a valuable fitness of the model to the analysis data. Finally, due to the small group size of outcome variable in the model, the results should be interpreted with caution. To ascertain the APTT predicting cut-off point value of minor bleeding, ROC curves were prepared for its value in the SSM group (Figure 4). The analysis showed the area under the curve (AUC) of 0.770, 95% CI (0.620, 0.921), meaning sufficient differentiation of patients with minor bleeding from those without the complication based on the APTT value. Optimal cut-off point for APTT was 33.0 s, with minor bleeding prediction for APTT ⩾33.0 s. Sensitivity of the analysis was 89% and specificity was 58%. It means that 89% patients with minor bleeding and 58% of patients without minor bleeding were correctly identified using the cut-off point received from APTT.

ROC curve for APTT value predicting minor bleeding in SSM group.
The occurrence of major bleeding was predicted by the PLT level in the DSM patients (MD = −188.76, 95% CI (−328.96, −48.56), p = 0.009), as well as in the SSM group (MD = −128.23, 95% CI (−241.69, −14.76), p = 0.027). In the SSM group, it was also related to the APTT level, however not significantly (p = 0.06). No other factors had an impact on major bleeding occurrence in both groups under study (Table S4). The factors significantly different between patients with and without major bleeding were included into logistic regression model as predictors variable, and the ones with major bleeding, as outcome. For the SSM and the DSM groups, none of the parameters was significantly predicting the presence of major bleeding on the basis of the logistic regression model.
As mentioned previously, the CTC exit site wound prolonged healing was observed more frequently, but not significantly, in the DSM group: 8 (11.4%) versus 4 (5.7%) episodes; p = 0.367, the DSM versus the SSM group, respectively; however, the analysis had not identified any predisposing factors in both groups (Table S5). Further analysis of patients with or without the CTC exit site infection revealed that the infectious complications occurred more frequently among older patients in the DSM group, MD = 11.35, 95% CI (2.41, 20.30), p = 0.021. Apart from that observation, no variable had a predicting value in occurrence of the side effect (Table S6.). None of the factors was a significant predictor of infection in the logistic regression model, either.
Discussion
This study is—to our best knowledge—the first comparison of different methods of the CTC exit site creation. The idea was based on our own observation that in older, malnourished patients, DSM caused prolonged healing and predisposed to exit site infection. In the cohort of 140 hemodialysis patients, two groups each of 70 patients were randomly formed to compare effectiveness of the SSM of the CTC exit site wound closing with the DSM, widely used in clinical practice. We did not observe any differences in terms of the complication rate between the groups, as they occurred in about 25.7% in the SSM group versus 27.1% in the DSM (Table 2). In detail, minor bleedings were observed equally in 12.8% patients of both groups; however, in the SSM group, the episode occurrence was strongly related to the APTT cut-off value which was within the normal range (33.0 s). Major bleeding appeared in 4.2% SSM cohort and in 2.8% DSM patients and was predisposed by PLT count in SSM and DSM (91.50 ± 3.54 and 130.00 ± 52.0 × 109/L, respectively), and additionally by the APTT level among the SSM individuals (39.00 ± 11.53 s). Our results correspond to previously reported ones, in which, despite differences in definition, minor and major bleeding complication occurrence was up to 30% and 2%, respectively. 13
Coagulation parameters in our study cohort, even in those patients who developed hemorrhagic complications, met criteria for a safe CTC insertion procedure. Notwithstanding, the significant correlation between minor bleeding occurrence and the APTT values, albeit in the normal range, in the SSM group may be taken as the signal for a particular hemostasis scrutiny when the tunnel closure is formed in the patients with APTT in the upper half of the norm.
Kerr et al. 14 reported that the use of purse-string suture around the CTC exit site reduces incidence of postprocedural bleeding from 25% to 6%. Interestingly, the suture was removed 2 days after the procedure. However, no data were provided on exit site healing and possible infectious complications.
Exit site infection occured with a similar rate, 4.3% in SSM and 5.6% in DSM patients. The reported incidence of the complication ranges from 6.0% to even 24% and may lead to tunnel infection, CTC loss, and septicemia with metastatic infectious complications, especially when caused by Staphylococcus aureus.
Of note is the lower percentage of prolonged tunnel healing above 14 days in the SSM group, 5.8% versus 11.3% in the DSM. This advantage, not significant in the small sample size study, could be tested in the further trial focusing on the patients carrying high-risk tunnel complication, that is, malnourished, heavily obese, elderly, diabetics.
The limitations of the study are retrospective, of flawed methodology, single-center character as well as small sample size. Therefore, further trials studying different methods of CTC implantation, to limit complications and extend vascular access longevity, are required.
In summary, the presented observations demonstrate that the SSM is equally efficient as the DSM tunneled catheter cuff stabilization. It traumatizes skin less and potentially offers an advantage of a better tunnel healing in the patients with deficient or excessive subcutaneous fat tissue. That assumption should be verified in further study, focused on such vulnerable patient categories. To our best knowledge, it is the first study of the influence of the methods of the CTC exit site suturing on the healing process, CTC maturation, as well as occurrence of complications.
Conclusion
The SSM of the exit site wound closing for central tunneled hemodialysis catheter implantation exhibits a similar efficiency as the DSM. It could potentially offer benefit to individuals with “paper” skin, that is, the elderly and those receiving long-term immunosuppressive treatment. This has to be proved in further study.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211019889 – Supplemental material for The efficacy of single suture for exit site wound closure and stabilization of hemodialysis central tunneled catheter
Supplemental material, sj-pdf-1-smo-10.1177_20503121211019889 for The efficacy of single suture for exit site wound closure and stabilization of hemodialysis central tunneled catheter by Tomasz Porazko, Andrzej Piersiak and Marian Klinger in SAGE Open Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the head of Bioethical Committee, Institute of Medical Sciences, Opole University (1/2021).
Informed consent
Informed and written informed consent was obtained before the procedure from all subjects included in the study. The patients presented in the images illustrating studied procedure methods have given their written consent for publishing the materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.