
Abstract
Salmonella enterica serotype Panama accounts for <1% of all reported cases of Salmonellosis. Previous reports suggest that it may be unusually virulent in children. We report the case of a family, five of six of whom developed a diarrheal illness due to this organism following exposure during a trip to Costa Rica. Included among these patients were three children, all of whom developed clinical shock requiring aggressive fluid resuscitation, and all of whom ultimately recovered. DNA fingerprinting, using pulsed-field gel electrophoresis, demonstrated that all three children were infected with an identical strain of Salmonella. Moreover, this strain was unique among strains recovered in Nebraska. Clinicians should be aware of the propensity of Salmonella enterica serotype Panama to cause especially severe disease in children; laboratory personnel should be aware of the unique need for thiourea buffering when attempting to perform pulsed-field gel electrophoresis analysis on such strains.
Keywords
Salmonellae are frequent and well-known causes of foodborne and gastrointestinal illness. According to the Centers for Disease Control and Prevention (CDC), 1 during the period 1998 through 2015, there were more than 2400 separate Salmonella outbreaks in the United States, where salmonellae are thought to be responsible for up to 1,000,000 illnesses annually, leading to 19,000 hospitalizations and 380 deaths. 2
Salmonella enterica serotype Panama is among the more than 2500 serotypes of Salmonella enterica 3 identified to date. Although this serotype is among the 30 most common Salmonella serotypes known to cause human disease, with 1903 cases reported over the 11 -year period from 2003 to 2013 (an average of 173 cases/year), 4 it nonetheless represents 1% of the serotypes detected, with a higher percentage isolated from blood. 5 We report a cluster of Salmonella serotype Panama infection occurring among members of a single family who vacationed in Costa Rica. Five of six family members became clinically ill, including three of the four children, all of whom developed sepsis requiring hospitalization and fluid resuscitation.
Report of cases
Three siblings who developed severe diarrhea and fever after returning from a vacation to Costa Rica in January 2017 are described in this report. Their mother experienced systemic flu-like symptoms with fever, chills, and abdominal pain (but no diarrhea) while in Costa Rica, with spontaneous resolution of her symptoms after returning home. Their father experienced diarrheal illness without fevers or chills, which also resolved without medical intervention. The family had one other child (an 18-year-old male) who accompanied them to Costa Rica but never became ill. No family members received typhoid immunization.
Patient A, a 14-year-old male, developed the onset of fever, chills, headache, and abdominal pain 4 days after return (4 days post-return (PR)) to the United States. He developed diarrhea consisting of 5–6 loose green stools per day on day 5 PR, with diffuse abdominal pain, and nausea. He was seen in the emergency department (ED) after 1 day of diarrhea (day 6 PR). He was discharged from the ED but was admitted the following day (day 7 PR) when a blood culture was noted to contain Gram-negative rods. On presentation, he had a blood pressure of 102/49, temperature of 38.2 C (his temperature during hospitalization reached a maximum of 40.1 C), serum bicarbonate level of 24 mg/dL, and leukocyte count of 6620/mm3. The patient was treated with intravenous IV ceftriaxone and aggressive fluid resuscitation during his hospitalization. Tests for malaria, dengue fever, and chikungunya were negative. A nucleic acid amplification test (NAAT), (FilmArray Gastrointestinal (GI) panel, BioFire Diagnostics, Salt Lake City, UT) performed on a stool specimen was positive for Salmonella species but attempts to culture Salmonella from the stool were negative. Blood cultures, however, were positive for a Salmonella serogroup D organism subsequently identified by the state public health laboratory as Salmonella enterica serotype Panama. Antimicrobial susceptibility testing determined the isolate to be susceptible to ampicillin, cefotaxime, and trimethoprim/sulfamethoxazole. The patient was discharged and completed a 14-day course of daily IV ceftriaxone; he remains well.
Patient B, an 11-year-old female, experienced the onset of symptoms on day 4 PR (the same day as patient A), with fever to 38.9 C, chills, and near-syncope. On day 6 PR, she began experiencing diarrhea, and on day 8 PR developed genital ulcerations and dysuria. She was admitted to the hospital, where her bicarbonate level was 24 mg/dL, and her leukocyte count was 4790/mm3. She was treated with IV ceftriaxone and aggressive fluid resuscitation. Likewise, her stool was positive by NAAT for Salmonella as well as enteropathogenic E. coli (but negative by culture). Blood cultures ultimately were positive for Salmonella enterica serotype Panama, with an antimicrobial susceptibility pattern identical to that of her brother’s isolate. Surface cultures of her genital lesions revealed only normal perineal flora. She was discharged to complete a 14-day course of daily IV ceftriaxone, and remains well.
Patient C, a 13-year-old male, developed fever and myalgia on day 8 PR from Costa Rica. These symptoms resolved spontaneously within 3 days and he returned to school and normal activity. Several days later, he developed fatigue, myalgia, vomiting, frequent non-bloody watery diarrhea, diffuse headache, dizziness, and chills prompting a visit to the ED. On presentation, he had a blood pressure of 84/44, temperature of 39.7 C, serum bicarbonate level of 20 mg/dL, and leukocyte count of 15,320/mm3. Like his siblings, he was admitted to the hospital and treated with IV ceftriaxone and aggressive fluid resuscitation. Although cultures of the blood were negative, he, too, had a stool NAAT which revealed the presence of Salmonella species. Culture from this stool ultimately identified Salmonella enterica serotype Panama. Following 5 days of treatment with IV ceftriaxone, he was switched to oral amoxicillin (based on the antimicrobial susceptibility pattern of his siblings’ isolates) and discharged in stable condition to complete a 14-day course of therapy as an outpatient.
Materials and methods
Salmonella isolates. Salmonella was detected and identified from the blood (patients A and B) and stool (patient C) of the three patients using standard laboratory procedures. Specifically, stool specimens were inoculated onto blood, MacConkey, MacConkey with sorbitol, xylose lysine deoxycholate, and cefoperazone vancomycin, and amphotericin agars, as well as Gram-negative broth. Cultured isolates were subsequently submitted to the Nebraska Public Health Laboratory for susceptibility testing, serotyping, and DNA fingerprinting by pulsed field gel electrophoresis (PFGE).
Molecular serotyping. DNA was extracted from Salmonella isolates using InstaGene Matrix (BioRad; Hercules, California) and the SimpliAmp Thermal Cycler (Applied Biosystems; Carlsbad, California). Multiplex PCR amplification was performed using 2 µL of biotinylated DNA with the xMAP Salmonella Serotyping Assay Kit, (Luminex; Austin, Texas) and HotStarTaq Master Mix PCR Kit (Qiagen; Valencia, California). Amplicons were hybridized with the appropriate bead mixture, labeled with streptavidin phycoerythrin (SAPE) reporter, and read by the xMAP instrument.
Genomic DNA isolation. Genomic DNA of the Salmonella strains was extracted using the SimpliAmp Thermal Cycler (Applied Biosystems; Carlsbad, California).
PFGE. PFGE was performed as described by Ribot et al. 6 Briefly, fingerprints were generated by XbaI digestion and addition of a solution of thiourea (10 mg/mL), and were then separated in 1% pulse field-certified agarose using an electrophoresis cell (BioRad; Hercules, California). The PFGE patterns were analyzed using Applied Math software version 6.6 (BioNumerics; Sint-Martens-Laten, Belgium). Isolates of epidemiologically unrelated Salmonella serotype Panama strains that had been detected in Nebraska (seven isolates) were included in the analysis.
Results
PFGE demonstrated that all three Salmonella serotype Panama isolates were indistinguishable (Figure 1). The nine isolates that were not epidemiologically linked were clearly distinguishable from the three epidemiologically linked isolates. The DNA fingerprints from the three strains from this study were new to the national PulseNet database. 7
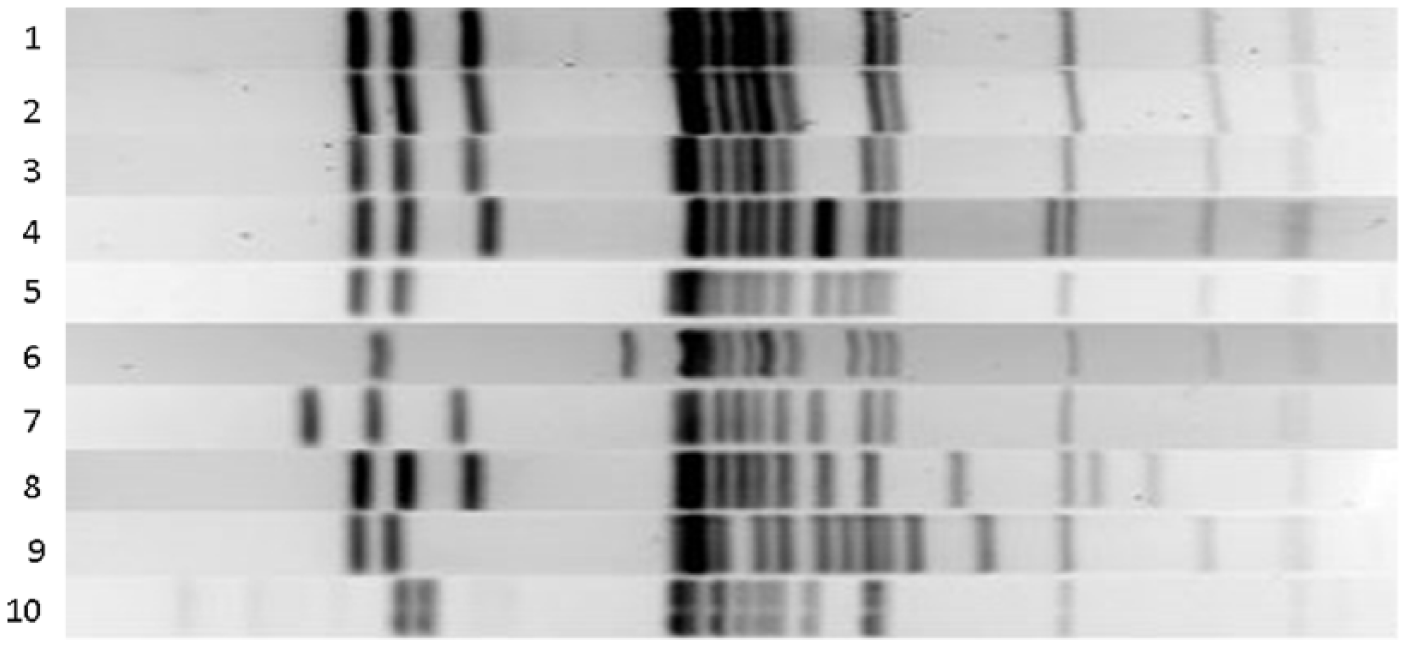
Salmonella enterica serotype Panama DNA fingerprints generated by pulsed field gel electrophoresis. Our patients’ isolates (National Public Health Laboratory (NPHL) 170069, 170070, 170084) are shown in lanes 3–5, with the remaining lanes (1–2, 6–10) from previous isolates detected in Nebraska. The first two digits in each isolate’s identification number refers to the year in which it was obtained.
All isolates were susceptible to ampicillin, cefoxitin, chloramphenicol, ciprofloxacin, ceftriaxone, gentamicin, kanamycin, naladixic acid, sulfisoxazole, streptomycin, trimethoprim-sulfamethoxazole, and tetracycline. All isolates were also thiourea-dependent (see discussion below).
Discussion
Salmonella serotype Panama was first isolated in 1934, when it was determined to be the cause of an outbreak of foodborne illness among American soldiers stationed in Panama. 8 Shortly thereafter, it was linked to severe diarrheal disease 9 and to invasive disease, particularly meningitis,10,11 among infants. In at least one instance, meningitis in an infant was linked to exposure to Salmonella serotype Panama excreted in the breast milk of her asymptomatic mother. 12 Moreover, in a study conducted in Taiwan, although only 11 of 257 episodes of pediatric gastroenteritis were due to serotype Panama, 8 of these 11 patients developed bacteremia. 13 These same authors noted that Salmonella serotype Panama was responsible for four of the six cases of meningitis seen in their study and observed that this organism was more invasive in Hep-2 cells than was Salmonella serotype Typhimurium. Our experience lends support to the notion that Salmonella serotype Panama may be more virulent than other Salmonella serotypes, particularly in children. The previous finding of a serotype-specific plasmid encoding for factors that promote extra-intestinal growth in a murine model 14 may provide a plausible mechanism for such a conclusion. We are unable to relate our female patient’s genital lesions to her Salmonella infection, although Salmonella serotype Panama has been associated with Bartholin’s abscess complicating food poisoning. 15
A food vehicle has been implicated in several previous outbreaks of Salmonella serotype Panama infection, with 109 cases resulting from beans prepared at a camp in Texas, 16 11 cases originating from lamb prepared in a residence in New York, and 17 cases from fruit salad prepared in a residence in New York. Our experience, coupled with the original isolation of the organism in Panama, and a separate report of 20 cases arising from Guatemalan cantaloupe 17 during a multistate outbreak in 2011, lead us to posit a Central American reservoir for Salmonella serotype Panama. While we cannot know, with certainty, the vehicle of disease transmission in our cases, our patients were exposed to a number of potential risk factors while vacationing in Costa Rica. Their meals were prepared by a live-in housekeeper and her daughter and they consumed high-risk foods such as chicken, eggs, salads, and fresh fruits prepared by this housekeeper.
The National Antimicrobial Resistance Monitoring System (NARMS) at the CDC tracks resistance patterns among enteric pathogens, including Salmonella. Although extra-intestinal Salmonella infection caused by strains other than Salmonella serotype Typhi are rare, data collected from 2003 to 2013 (where total isolates tested were > 100), showed that Salmonella serotype Panama was the third most likely non-typhoidal serotype to be isolated from extra-intestinal sources (15.1%), exceeded only by serotypes Schwarzengrund (15.3%) and Poona (15.1%). 18 The NARMS report showed that Salmonella enterica serotype Panama had the strongest association between resistance to ⩾ 1 agent and isolation from the blood with an operating room (OR) of 6.85 (95% confidence interval (CI): 1.25–37.58).
National surveillance for Salmonella infections using data from a 42-year period of 1968–2011 did show that serotype Panama, while representing less than 1% of reported isolates, was nonetheless one of the top 30 serotypes detected in the United States. Of note, 7.1% of reported isolates were obtained from blood, cerebrospinal fluid, or joint specimens. 5 More recent data from the National Salmonella Surveillance Annual Report for 2013 showed that of the 38,273 Salmonella isolates that were serotyped, only 163 represented serotype Panama (0.43%) and only 1 of these was detected in Nebraska. 19
The percentage of non-human isolates of serotype Panama by source reported by the National Veterinary Services laboratories showed porcine sources to be the most common (45.87%), followed by bovine (11.86%) and turkey (8.89%). 14 In our case, state and local health departments conducted epidemiologic and traceback investigations but were unable to identify the source of the outbreak, not surprising given the likelihood of its origin in Costa Rica.
Our experience was both clinically concerning and microbiologically unusual. Liesegang and Tschape, 20 in 2002, described thiourea-dependence in certain Salmonella and E. coli strains, among them Salmonella serotype Panama. These strains are sensitive to rapid DNA degradation during the course of PFGE pattern analysis thereby requiring the application of 10 mg/mL thiourea into the running buffer. The Salmonella strain isolated from our patients exhibited such a requirement. While DNA degradation during sample preparation for PFGE is not uncommon with certain Gram-negative rods,21,22 this dependence is strain, rather than species or serotype, dependent. Thus, temporal detection of a dependence on thiourea in an identified serotype might suggest outbreak relatedness of the isolates.
In conclusion, this case study describes three children from a single family who developed sepsis due to Salmonella serotype Panama, and required aggressive fluid resuscitation. Clinicians caring for children with gastroenteritis and sepsis syndromes, as well as public health officials, should be aware of the potential for some Salmonella serotypes, including Panama, to cause especially severe disease. They should also be aware of a potential epidemiologic link to Central American travel or exposure to Central American foods. Microbiology laboratory personnel should be aware of the unique requirements for thiourea buffering when performing PFGE analysis, especially when a rare serotype has been detected.
Footnotes
Acknowledgements
The views expressed herein are those of the authors and do not necessarily reflect the position of the University of Nebraska, the Nebraska Public Health Laboratory, or their component entities.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.