
Abstract
Fibular hemimelia is a rare congenital malformation that is commonly associated with other lower limb abnormalities. This is a unique case of a bicruciate ligament, anterior cru ciate ligament/posterior cruciate ligament (ACL/PCL) deficiency in a 6-year-old female with fibular hemimelia in which we describe an ACL reconstruction using autograft–allograft hybrid technique. This case focuses on the technical aspects of an ACL reconstruction using a physeal-sparing technique with a hybrid ACL graft in a pediatric patient with fibular hemimelia. When evaluating patients with fibular hemimelia, it is important to consider implications of treatment in a stepwise manner as this condition commonly presents with other abnormalities that will most likely require multiple procedures, including limb lengthening.
Introduction
Fibular hemimelia (FH) is the most common long bone abnormality. 1 The severity of this condition can be classified as Type I or II, characterizing it as a partial shortening or complete aplasia, respectively. 2 FH often presents with other abnormalities such as inferior patellar displacement, 3 deletion of forefoot lateral rays, 4 isolated absence of the posterior cruciate ligament 5 or anterior cruciate ligament,6–9 and complete absence of both cruciate ligaments. 10 Cruciate ligament aplasia alone has a very rare occurrence of just 0.017 per 1000 live births, most of whom will eventually require a knee replacement. 9 This case report describes the surgical management of a pediatric patient with complete unilateral FH as well as bicruciate ligament aplasia.
Case report
A 6-year-old female with a history of left FH and limb-length discrepancy presented for orthopedic evaluation of knee instability. Anterior tibial instability appeared to be the most pressing clinical issue with frequent subluxation episodes. The patient’s medical history revealed a left Achilles tendon lengthening at 11 months of age. Bilateral imaging of the legs revealed an absent left fibula (Figure 1). The patient’s left leg was 3.5 to 4 in. shorter than the right with the left foot also smaller in size than the unaffected right side. On the affected left side, she was also ACL and PCL deficient. Physical exam revealed a normal straight leg raise with full range of motion, a grossly positive Lachman at 30° of knee flexion and a positive tibial sag at 90° of knee flexion. Varus–valgus stress tests in full extension and in 30° of flexion were normal.

Bilateral radiographs demonstrating absence of the left fibula. Red lines approximate graft placement. (a) Anterior–posterior (AP) view and (b) lateral view.
Previous consultations with a pediatric orthopedic surgeon addressed procedures to potentially equalize the length of the legs through limb lengthening. Specifically, a tibial osteotomy of the left leg with the application of ring external fixator was recommended. It was also recommended that prior to the lengthening surgery, the knee ligaments should be stabilized. The patient was primarily symptomatic with instability from the anterior; this was visibly evident with anterior tibial subluxation episodes during walking. She was thought to be a candidate for ACL reconstruction using the Micheli procedure, 11 a physeal-sparing technique utilizing the patient’s iliotibial band (ITB) autograft. However, due to the degree of anterior laxity and the expected small width and thickness of the ITB, graft augmentation procedures were considered.
In the operating room, the exam under general anesthesia again revealed a grossly positive Lachman with an excess of 2 cm of anterior tibial translation and a positive pivot shift. Her medial collateral ligament and laterlal collateral ligament were intact and stable and the PCL absent. A photo of the legs demonstrates the marked difference in limb length (Figure 2).

Photograph demonstrating marked limb-length discrepancy.
After incision and exposure of the lateral thigh, a portion of the ITB was harvested producing a graft, 120 mm in length and 10 mm wide (Figure 3(a)). As the graft was considerably small in cross-section, and the anterior tibial laxity was quite significant, the decision to use a semitendinosus allograft to augment the reconstruction was made (Figure 3(b)). The allograft was baseball stitched to the ITB under tension.

(a) ITB autograft measuring 120 mm in length and 10 mm in width. (b) Semitendinosus allograft was used to augment the ITB autograft.
Arthroscopic examination of the knee was consistent with the clinical examination finding of complete absence of both the cruciate ligaments (Figure 4(b)). In addition, she had a relatively small notch. The geometry of the notch was not altered at the time of surgery because of the relatively horizontal position of the ACL graft, nor was the posterior cruciate ligament deficiency addressed. The femoral portion of the graft was sutured to the intermuscular septum, while the tibial side was sutured to the periosteum of the proximal anterior tibia at 0° of extension after being passed intra-articularly. This patient was very young and therefore had a small transverse meniscal ligament. After intra-articular routing of the graft, it was decided to not place the graft under the intermeniscal ligament as is normally done in the Micheli procedure 11 as a precaution to avoid damage to intermeniscal ligament. After the graft was secured to the tibia with sutures in the periosteum (Figure 4(a)), the Lachman exam was repeated and the anterior laxity of the tibia on the femur had been minimized. Anterior tibial translation was reduced to an appropriate 3 mm at 30° of flexion. The patient tolerated the procedure well and left the operating with the leg in full extension in a posterior splint. The patient returned to the clinic 13 months postoperatively. She subjectively reported that she has been very active playing on the playground with friends and feels that the knee is quite stable and strong. Her physical exam revealed full range of motion from 0° to 140° with no terminal flexion pain, a stable Lachman’s exam, good quadriceps contraction from a straight leg raise, and no tenderness to palpation along the ITB. Radiographic imaging of the knee and tibia revealed no growth alterations or damage to the physes on the proximal tibia or distal femur.
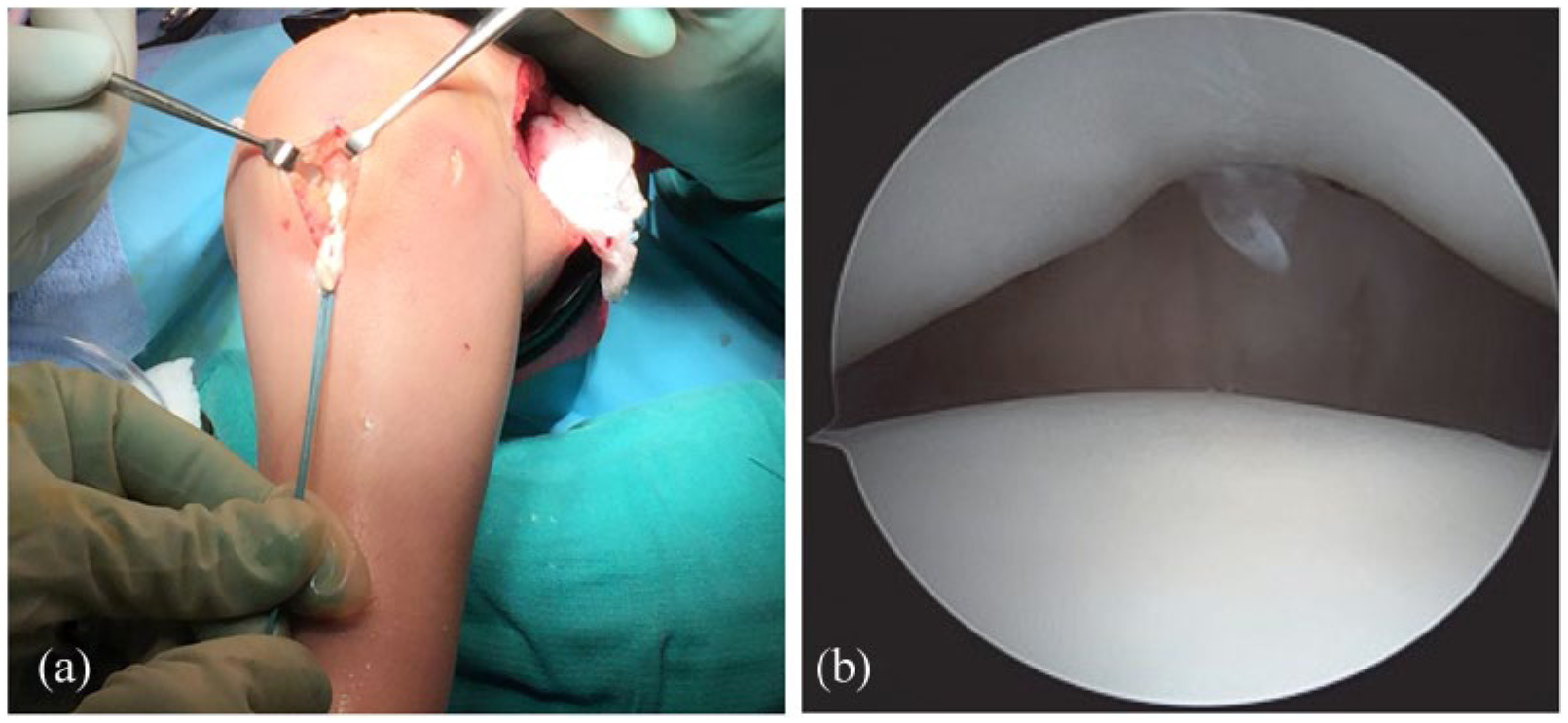
(a) Augmented graft prior to suturing into periosteum. (b) Arthroscopic examination of the knee joint revealing cruciate ligament aplasia.
Discussion
FH is a rare congenital deformity that is often accompanied by other structural abnormalities. The treatment of congenital absence of the cruciate ligaments is controversial. In older patients with incomplete notch formation, the addition of a new ligament may require significant removal of bone during notchplasty. 10 In many younger patients, with incomplete bone formation, conservative treatment has been successful. Hejgaard and Kjaerulff 12 reported a 7-year-old patient with congenital absence of the ACL who was effectively treated with a brace, but noted that surgical treatment may be needed at the end of the growth period.
The absence of the cruciate ligaments increases the risk for meniscal injuries and retropatellar pain, 13 making the long-term condition of the knee joint a great concern. Patients with degenerative menisci will most likely result in articular cartilage damage, 14 drastically increasing the risk of osteoarthritis. 15
This patient will have a limb-lengthening procedure next. It is usually advisable to stabilize the knee first,16,17 given that the limb-lengthening operation on a lower extremity with an unstable knee joint can lead to a contracture or subluxation of the tibia on the femur. 17
A very important feature of this case was the use of a semitendinosus allograft to augment the iliotibial autograft for the ACL. This “hybrid” graft is most often used in transphyseal ACL reconstruction with hamstring autograft in cases of insufficient tissue. 18 The decision to use this graft was subjective and focused both on the available amount of ITB tissue and the degree of anterior tibial laxity. The cross-sectional area (CSA) of the ACL does affect the degree of strain experienced by the ACL. 19 The addition of the allograft more than doubled the CSA of the reconstructed ACL.
With congenital absence of both cruciate ligaments, this patient’s knee joint was very unstable. This stability prevented her from being active without experiencing giving-way episodes that caused her to fall during activities such as running. Due to the young age of the patient and, hence, open physes, a physeal-sparing method of reconstruction was her best option. Kocher et al. reported a series of 44 skeletally immature patients in need of ACL reconstruction, all of whom underwent a combined intra-articular and extra-articular physeal-sparing technique using an ITB autograft. They reported excellent functional outcome, a low revision rate, and minimal risk of iatrogenic growth disturbance. Three of the patients in that study presented with congenital absence of the ACL. An ACL deficient child with clinical instability that cannot be stabilized with a brace is an indication for surgical reconstruction in this patient population. 20
Knowing the risk of an unstable, ACL deficient knee and the seemingly inevitable long-term degenerative changes that accompany this condition, reconstructive surgery was thought to be the best option for this patient. Long-term follow-up will determine the success of isolated hybrid ACL reconstruction of a bicruciate deficient knee in a 6-year-old female with FH.
Conclusion
This case focuses on the technical aspects of an ACL reconstruction using a physeal-sparing technique with a hybrid ACL graft in a pediatric patient with FH. When evaluating patients with FH, it is important to consider implications of treatment in a stepwise manner as this condition commonly presents with other abnormalities that will most likely require multiple procedures, including limb lengthening.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from the patient to publish the findings of this clinical case while complying with HIPAA Law.