
Abstract
Vast literature exists detailing the identification and management of central auditory processing disorder in children: however, less information is available regarding central auditory processing disorder in the adult population. This study aimed to document the diagnostic and management procedure for adults presenting at a multidisciplinary clinic due to concerns regarding their listening and central auditory processing skills. This retrospective study was a case file audit of two adults (a male, aged 37 years and a female, aged 44 years) who presented at a multidisciplinary (audiology and speech pathology) clinic for a hearing and central auditory processing evaluation. Both participants completed a case history questionnaire and were then interviewed with results being documented in their file. Participants were evaluated by a dually qualified audiologist-speech pathologist on a battery of peripheral hearing tests (including pure-tone threshold audiometry, immittance measures and speech tests), central auditory processing assessments (including monaural low redundancy, dichotic listening and temporal processing tests) and evaluation of short-term auditory memory skills. Participants were self-referred, never having been assessed previously for central auditory processing disorder, yet had perceived heightened difficulty with processing information; having conversations (particularly in noisy work or social environments) and remembering information, resulting in a range of psychosocial responses. Following diagnosis of central auditory processing disorder, participants undertook an individualized short-term aural rehabilitation program as dictated by their needs and preferences. Post-program participants perceived better ability to listen and process information even in adverse listening conditions. They reported that their newly learned skills improved their work abilities and social participation leading to positive outcomes. Medical and other allied health professionals should consider the possibility of presentation of central auditory processing disorder in adulthood and make appropriate referrals for central auditory processing testing to facilitate diagnosis and appropriate intervention. Aural rehabilitation should be considered for adults newly diagnosed with central auditory processing disorder.
Introduction
Central auditory processes (CAP) are the auditory mechanisms responsible for sound localization and lateralization, auditory discrimination, auditory pattern recognition, temporal aspects of audition (including temporal resolution, temporal masking, temporal integration and temporal ordering) and auditory performance with competing or degraded acoustic signals. 1 Accordingly, deficits in any of these functions lead to inadequate processing of auditory information. Central auditory processing disorder (CAPD) is a deficit in the processing of auditory-presented information despite usually normal pure-tone hearing thresholds.
CAPD is a topical area frequently discussed in reference to children and less frequently discussed in relation to adults, particularly in regard to assessment, diagnosis, treatment and management. CAPD in children is characterized by listening and/or processing difficulties, usually with no other medical conditions such as stroke, traumatic brain injury or temporal lobe tumors. Among children, behavioral characteristics associated with CAPD include difficulty comprehending speech in competing or reverberant environments, frequent requests for repetition of information, misunderstanding messages, inconsistent or inappropriate responses, delays in response to oral communication, difficulty following complex auditory directions, difficulty with sound localization, inattentiveness and distractibility and literacy difficulties. 1 Furthermore, children suspected of suffering from CAPD are often reported as being intolerant to loud noise, are frequently distracted by background noise and have difficulty following instructions. 2 These symptoms are not exclusive to CAPD and diagnostic audiological testing is undertaken to confirm the diagnosis of CAPD.
According to the American Academy of Audiology (AAA) 3 and the European Perspective on Auditory Processing Disorder, 4 the behavioral manifestations and symptoms reported and/or observed during interviewing or observation of patients (both children and adults) suspected of having CAPD may include difficulty with understanding speech in competing background noise or reverberant environments, localizing to sound sources, hearing on the phone, following rapid speech, following directions, detecting subtle changes in prosody, learning a foreign language or novel speech materials, maintaining attention, musical ability, literacy and learning. Further behavioral manifestations include seeking visual or facial cues to aid understanding, frequently requesting repetition or rephrasing, responding inconsistently or inadequately, having hyperacusis and being easily distracted.
Research on test performance in young and middle-aged adults is surprisingly less common than the literature on children, especially since many original tests of central auditory processing were developed based on adult samples, for example, the pitch and duration pattern tests developed by Musiek.5,6 Since the pure-tone audiogram provides no information about CAP, specific CAP tests should be used to provide diagnostic and rehabilitative information. 7 Neijenhuis 8 evaluated and developed a test battery for use with adult populations and concluded that, although more research is needed to refine test batteries for use on specific populations, the developed battery is of clinical value.
In general, adult-based research has identified CAPD as a “hidden hearing loss” characterized by difficulty with listening or recognizing speech in the presence of noise despite normal pure-tone thresholds. 9 The association between CAP (particularly temporal processing) and literacy deficits in adults has also been explored. Hari and Kiesila 10 evaluated 10 dyslexic adults and 20 control subjects using a series of binaural clicks, with an auditory processing deficit defined as difficulty processing rapid sound sequences. Results suggested that dyslexic adults displayed difficulty processing rapid sound sequences, which was manifested as a significant delay in their conscious auditory perceptions and continued throughout their lifetime. Ahissar et al. 11 also investigated the association between CAP abilities and reading skills. In this study, 102 adults were assessed on a battery of psychoacoustic measures and standard measures of reading and spelling. Results suggested that an association exists between CAP skills and reading. In particular, poor readers had difficulty with tasks that required spectral distinctions, such as frequency discrimination.
CAPD may occur subsequent to or comorbid with other primary conditions, for example, after stroke, 12 following traumatic brain injury 13 or comorbid with cognitive deficits such as Alzheimer’s disease. 14 To distinguish between multiple conditions with similar symptoms, a comprehensive, multidisciplinary assessment is required. 15
In aging adults, difficulty associated with listening in compromised environments, such as situations in which there is background noise, is commonly associated with peripheral hearing loss but may also be reflective of CAPD in this population. 16 In particular, aging adults experience difficulty with speech perception (particularly speech-in-noise) and discrimination.17,18 In a sample of 2015 adults aged 55 years and older, Golding 19 concluded that the detection of CAP abnormality for average older adults increased with age (binaural abnormality was detected in 27.3% of participants aged 64 years and lower; 44.3% of participant aged 65–74 years and 69.0% of participants aged 75 years and above), with men more likely to have a higher number of abnormal CAP test outcomes than women. The probability of demonstrating CAP abnormality increased with accompanying cognitive decline or increased hearing impairment. According to Atcherson et al., 20 structural and functional central nervous system changes occur with advancing age and contribute to the processing of auditory information but are also influenced by hearing loss and cognitive decline. Cognitive aging research highlights that aging is associated with reduced sensory and mental processing speed and a reduction in cognitive skills (reduced working memory and attention), which affects listening. 21 Furthermore, in a study examining central aspects of perception (temporal resolution and speech recognition in noise) and the role of attention (gap detection) in a group of 18 adults diagnosed with mild cognitive impairment and age-matched controls, Iliadou et al. 22 found that the group with mild cognitive impairment performed significantly poorer than the control group on the speech recognition in noise task as well as the gap detection task (particularly in the right ear which although must be interpreted with caution, may be linked to a left hemisphere auditory processing deficit). These authors further concluded that auditory temporal processing tests might be useful in the early diagnosis of mild cognitive impairment.
In regard to management, Whitelaw 23 exposed the myth that since there is no cure for CAPD in adults, there is no value in assessing their CAP skills or in providing adults with management. Whitelaw 23 further highlights that the auditory system remains plastic for a long period of time and that offering intervention to adults with CAPD is viable. While numerous child-focused management approaches have been developed, only few have been trialed on adults, despite the notion that most people with CAPD will potentially live with these disorders throughout their lives.24,25
According to Bellis et al., 26 auditory interventions aim at improving auditory deficits identified by valid tests of auditory function in a targeted, deficit-specific manner. Bellis 27 suggested the inclusion of environmental modifications, remediation activities and compensatory strategies in remediation interventions. Both bottom-up and top-down interventions have commonly been used in the management of CAPD which may be particularly applicable if CAPD is viewed as a spectrum disorder. 28 More specifically, interventions described in the CAPD literature have included the use of assistive listening devices (e.g., frequency modulated or remote microphone listening systems as used by Koohi et al. 12 with stroke patients with CAPD), phonemic training program, 29 dichotic interaural intensity difference training, 30 metalinguistic approaches 31 or computer programs such as Earobics (by Compu.Ed.), 32 LACE, 33 ARIA, 34 BrainHQ exercises (e.g., results of the IMPACT study 35 found that using Brain HQ exercises for 40 h led to an average increase in auditory processing speed of 135%) and the ReadMyQuips Speech Comprehension Training System (developed by Levitt, 36 who found that following the use of this program, individuals with mild to moderate hearing loss were able to improve their speech comprehension by around 30%). Some of these intervention examples have primarily been used with children who have CAPD, with only few programs (e.g., LACE) specifically containing materials applicable to adults. It is thus important to investigate the assessment and management of young adults who present for the first time in adulthood with symptoms suggestive of CAPD.
The aim of this retrospective study was to document the diagnostic outcomes and management process for two adults presenting at a multidisciplinary audiology and speech pathology clinic due to concerns regarding their listening and CAP abilities.
Case section
This retrospective study was a case file audit of two adults (Cases A and B) who presented at a multidisciplinary (audiology and speech pathology) clinic for a hearing and CAP evaluation. These adults (out of a total of four adults with CAPD seen in a 6-month period) were specifically selected for this audit, since they both participated in intervention post diagnosis of CAPD. One participant was 37-year-old man, working in an administration office servicing international students. The other participant was a 44-year-old woman and was the owner of a retail shop in a busy shopping precinct that attracts local and international shoppers. Both participants lived (with their respective partners) in metropolitan Melbourne and were English speaking. They both provided written informed consent allowing their information to be used for research purposes as long as anonymity was upheld.
The following procedure was followed for the diagnostic evaluation:
Participants completed a short, generic questionnaire that enquired about their demographic information, referral information (referrer and concern leading to the referral), work history, education, medical history and family history of hearing, CAP or learning difficulty. The final part of the questionnaire covered 10 questions devoted to hearing, listening and communication. Nine questions required a rating on a 3-point Likert-type scale (1 = no difficulty; 2 = some difficulty and 3 = lots of difficulty), while one question was an open-ended question enquiring about the top three situations that participants perceived as the most difficult and which were important for them to improve.
Participants were interviewed and further details regarding their completed case history form and social-communication functioning were discussed and results were documented.
Participants were evaluated by a dually qualified audiologist-speech pathologist using the following test battery:
Peripheral hearing tests (including pure-tone threshold audiometry, immittance measures and speech audiometry using the AB word list developed by the National Acoustic Laboratory).
CAP assessment—the test battery was derived in accordance with AAA 3 and specific tests were selected for use with these participants. Tests were as follows: monaural low-redundancy speech tests to evaluate auditory figure-ground, discrimination and auditory closure ((1) Speech-in-noise test using the AB word list with monaural speech noise and (2) The Time compressed Speech Test), 37 dichotic listening tests to evaluate binaural integration ((1) the Macquarie Staggered Spondaic Word Test29,38 and (2) Dichotic Digits Test 5 ) and test of temporal patterning to evaluate auditory patterning and sequencing (Pitch Pattern Test6,39). All stimuli were presented at suprathreshold level at 60 dBHL. A diagnosis of CAPD was made on the basis of ‒2SD on any one test or ‒1SD on two or more tests. 1
Short-term auditory memory (STAM) testing using the digits forwards and backwards (working memory) subtests of the Test of Memory and Learning. 40 Working memory is the ability to follow, retain and integrate auditory-presented information and is a primary component of speech perception. 41 Hence a measure of working memory was included in the test battery.
Comparison between pure-tone hearing threshold tests, middle ear functioning and CAP test performance against normative data led to a diagnosis of CAPD.
Following diagnosis, the following intervention procedure was adopted.
Adults participated in 60-min individualized intervention sessions over consecutive weeks (Adult A participated in two sessions and Adult B participated in four sessions). Management sessions were individualized to suit each participant’s preferences and determined by factors such as restricted time off work and financial constraints rather than dictated by the clinician as to how many sessions they should attend. The intervention sessions were client-centered and tailored to individual client’s needs. 42 Post-program results were obtained via interview and documented in their file.
Results
Analysis of participant’s case histories and interviews (Table 1) revealed that both participants were self-referred, never having been assessed previously for CAP due to their essentially non-eventful school and work career. Participants both had recently perceived heightened difficulty with processing information; having conversations (particularly in noisy work or social environments) and remembering information. Participants reported that these difficulties had resulted in a range of psychosocial responses (including low confidence and depression), leading them to talk to their General Physician and seek a CAP assessment. For further details refer Table 1.
Case history and interview information.
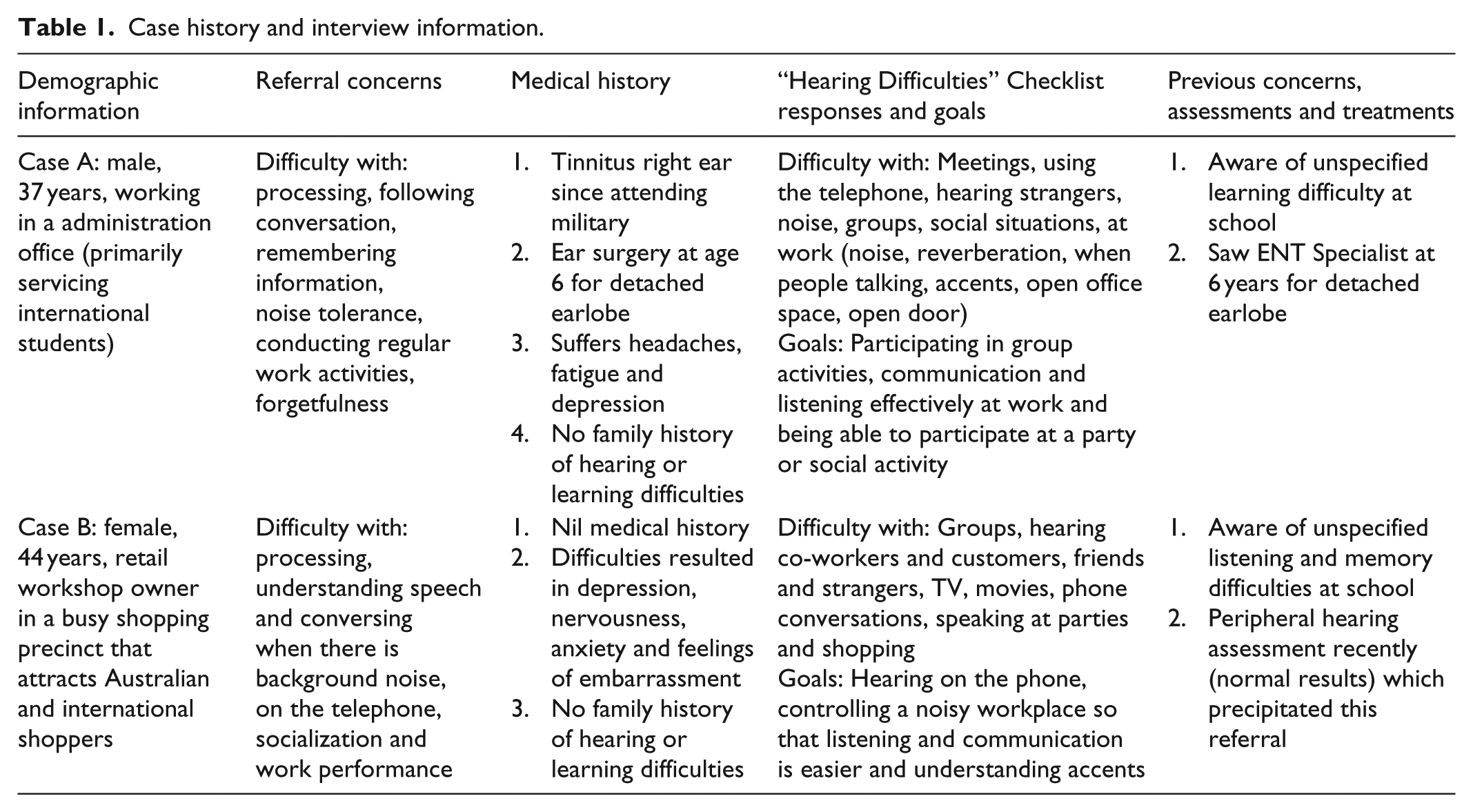
Case A reported a significant case history (when younger) of ear problems (detached earlobe), for which he sought medical attention (ear surgery) and additionally reported a positive history of noise exposure (gun fire when he was in the military at age 18 for 2 years). Case B did not report any history of ear problems. For both participants, no congenital abnormalities were reported and no further significant medical history was experienced. In regard to psychological status, both participants reported decreased psychological well-being including responses such as depression, embarrassment, anxiety and lack of confidence. Case A reported frequently feeling fatigued and experienced headaches.
These negative reactions were reinforced by participants’ self-reports. Results of the “Hearing Difficulty” sections of the case history suggested similar results for both participants, in that, neither had difficulty in quiet conditions, hearing family members, hearing the phone ringing from another room or hearing environmental sounds such as a car horn. Both participants reported some difficulty with hearing strangers speak and lots of difficulty with listening in noisy conditions and in group situations. In addition, Case A reported some difficulty with meetings while Case B reported a lot of difficulty with meetings and using the telephone. The three situations Case A identified as the most difficult and the most important for improvement included; participating in group activities, communication and listening effectively at work and being able to participate at a party or social activity. The three situations Case B identified as the most difficult and the most important for improvement included: hearing on the phone, controlling a noisy workplace so that listening and communication is easier and understanding accents.
On pure-tone audiometric testing, it was evident that Case A had normal hearing in the right ear (Pure-Tone Average of 5 dB) until 8000 Hz with a mild high-frequency dip at 8000 Hz (possibly attributed to previous noise exposure). Case A had normal hearing in the left ear (pure-tone average of 5 dB). Case B had normal hearing bilaterally (pure-tone average of 20 dB right ear and 15 dB left ear). Both participants had normal middle-ear functioning bilaterally on acoustic immittance testing and high accuracy on speech discrimination testing in quiet conditions (Case A = 94% right ear and 97% left ear; Case B = 97% accuracy bilaterally). On CAP and STAM testing, some difficulties were identified. See Table 2 for participant’s test profiles.
Diagnostic test results, intervention targets and post-training outcomes.
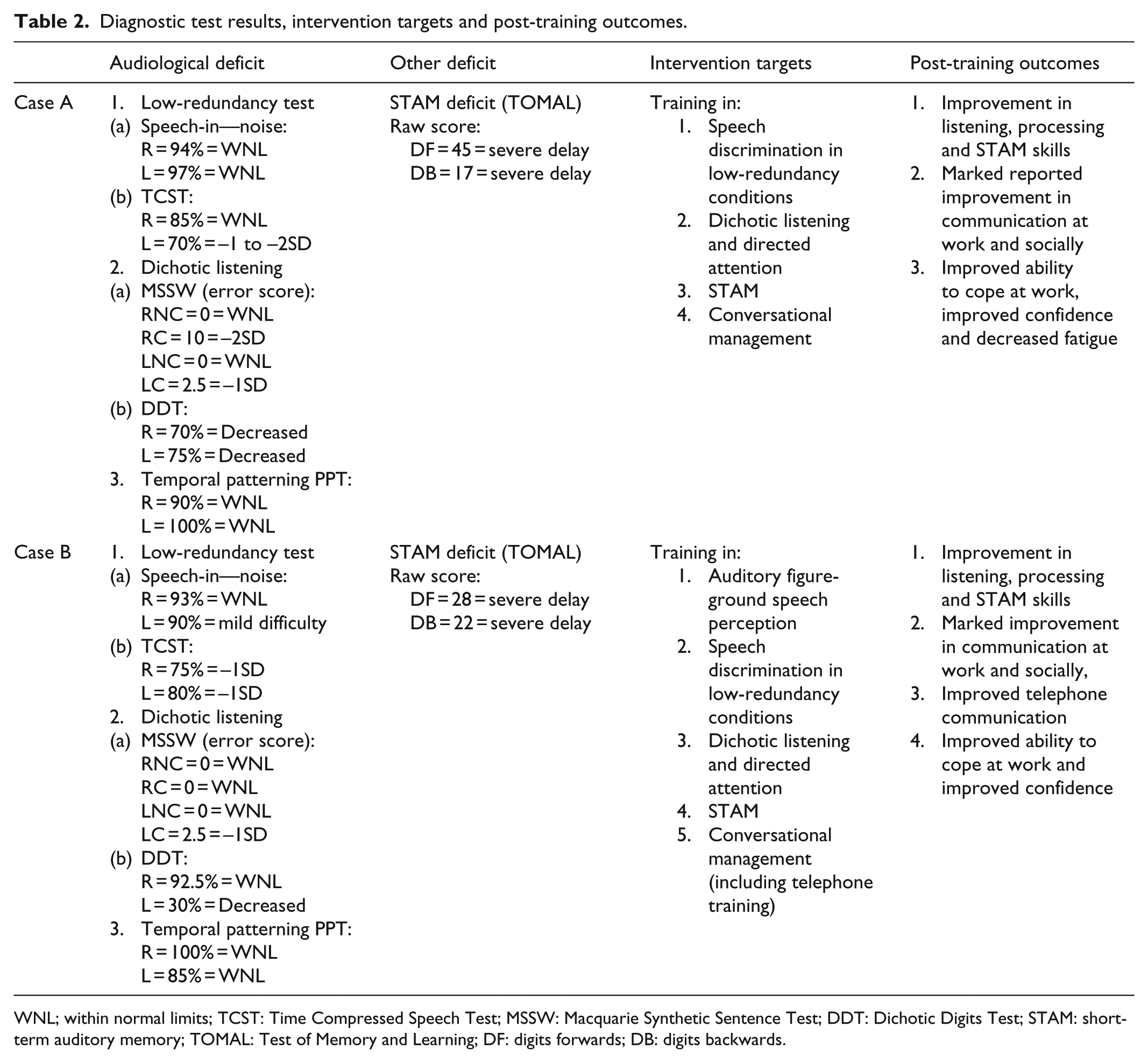
WNL; within normal limits; TCST: Time Compressed Speech Test; MSSW: Macquarie Synthetic Sentence Test; DDT: Dichotic Digits Test; STAM: short-term auditory memory; TOMAL: Test of Memory and Learning; DF: digits forwards; DB: digits backwards.
As can be seen from Table 2, both participants experienced difficulty with speech processing in conditions with low redundancy (Time Compressed Speech), dichotic listening and STAM. Case B also experienced difficulty with speech-in-noise (auditory figure-ground).
In regard to intervention, in addition to the one-on-one session with the dually qualified audiologist-speech pathologist, guidance materials were provided suggesting home and work strategies for promoting effective listening and communication, acoustic noise control, use of technology (e.g., a recording pen or voice to text teletext) and STAM. Participants were cooperative and motivated to participate in all intervention activities. In particular, intervention focused on the following: speech discrimination, auditory figure-ground (for case B only), auditory closure, dichotic listening, STAM strategy training and conversational management. More specifically, the management program consisted of exercises to improve listening, such as the landmark auditory tracking technique according to De Filippo and Scott; 43 using speech stimuli in the presence of either or both four talker babble background noise and/or reverberant modified babble noise presented binaurally, speech discrimination training (repetition of syllables and minimal pairs) as per Sloan’s technique; 44 exercises targeting auditory closure as per Heine; 45 dichotic listening (using the Dichotic Interaural Intensity Difference training procedure) as per Musiek et al. 46 as well as targeting directed attention using speech stimuli monaurally and four talker babble background noise in the opposite ear; STAM training using strategies such as repetition, chunking, association, visualization and mnemonic training as per Baddeley, 47 McNamara and Scott 48 and Bell; 49 and communication training, which is frequently used with adults with hearing loss or dual sensory loss. 50 Communication training included strategies to address environmental, speaker–listener variables and the content of the conversation. For example, developing a listener difficulty hierarchy and problem solving of how each step of the hierarchy could be managed using communication training techniques. The Listening now! program 45 covers many of the above areas and was used as a resource. For further details refer Table 2.
In post-training interviews, both participants reported significant improvements in deficit areas post-intervention. Case A made changes to his home and work environment (e.g., using topic maintenance and communication repair strategies at home, and introducing the use of headphones to control noise and acoustic modifications for noise control at work) and enrolled at University to pursue a higher degree. This participant also reported less fatigue, greatly improved communication skills (use of clarification strategies to repair conversational breakdown) and communication confidence, particularly at work. Case A also reported better directed attention to speakers and less distraction when multiple speakers were speaking. Case B reported having improved conversational and STAM skills (necessary for ordering stock in her retail shop and serving customers) and better speech discrimination and listening skills in general (including when there was high background noise). Case B made acoustical changes in her work environment (made a quiet listening corner using her retail stock as a barrier), structured more off-site meetings in quiet conditions, sought out a quieter environment for telephone conversations, introduced the use of teletext, used earplugs to control noise, proactively took rest breaks when fatigued and used communication strategies more effectively (e.g., she used assertive listening strategies, ensured topic maintenance, increased her use of clarification requests and asked for specific clarification when a conversation broke down). In addition, Case B reported increased self-esteem manifested as improved confidence at work.
Discussion
The present compilation of case studies presents important evidence for CAP difficulties experienced by young adults. Interestingly, the two adults in this study only sought help for their listening and CAP difficulties in adulthood. Possible explanations for this late referral and subsequent diagnosis may be that 20–30 years ago, CAPD was not topical and diagnostic, and rehabilitation services were not as readily available, particularly in the absence of a peripheral hearing loss. Limited knowledge of CAPD may have restricted identification and referral for assessment. It is also plausible that these adults showed mild symptoms of listening and processing difficulty as children and were not overly debilitated and thus professional assistance was only sought when their listening difficulties, work environment and emotional state exacerbated. Research has shown that educators are the primary referrers for CAP assessments, while self-referral or families refer less often. 51 Since the participants in this study were no longer in an educational setting, it is possible that their difficulties were subtle (not due to noticeable peripheral hearing loss for example) and may not have been easily identified by themselves or their family.
The positive value of questionnaires has been identified by Bamiou et al. 52 and by us, the “Hearing Difficulty” questionnaire substantiated information obtained via the case history, allowed for measurement of participant’s perceived hearing, listening and communication difficulty and allowed for identification of participant’s perceived area of deficit requiring change (goals for intervention).
Both participants in this study were diagnosed with CAPD. However, they did not have the identical auditory test profile or difficulty with all the CAP assessments in the test battery. The importance of identification of sub-skills under the CAPD category is that a client-focused approach is necessary to address each individual’s strengths and weaknesses and to plan intervention goals that are specific to each individual’s needs.
In regard to each participant’s aural rehabilitation management program, a client-centered approach was used. A client-centered approach “actively involves the client in every decision concerning treatment” including consideration of the client’s expressed social and psychological needs. 42 Based on the participant’s descriptions of their work and home environment, as well as consideration of their CAP difficulties, simulations were set up (e.g., if high background noise was a distracter, a noise recording was used). Auditory training was thus conducted in as realistic a manner as possible. Both participants showed improvements in their listening, communication, STAM and general CAP abilities following participation in their individualized aural rehabilitation program. These adults’ participation in the auditory program highlights the notion that successful rehabilitation should be based on careful diagnosis of impairment and disability, identification of individual needs, setting specific goals and supporting self-management.
Hearing loss is associated with disability and psychological distress. 53 Furthermore, hearing loss is related to maladaptive communication strategies, self-perceptions of poor social skills and reduced self-esteem and, as a result, deterioration in quality of life. One of the findings of a study of the psychological profile and social behavior of young hearing-impaired working adults showed a higher level of psychological distress among the hearing-impaired group than among the control group, which was reflected mainly in the symptom domains of anxiety, depression, phobic anxiety, interpersonal sensitivity and hostility. 54 This association may be true for people with CAPD.
The participants in this study had reduced social activities, experienced increased relational problems with family and friends and suffered emotional difficulties at work. It is conceivable that these participants may have been discouraged from exposure to socially challenging situations, resulting in isolation, depression and irritability which, in a vicious cycle, lead to poorer social-communication performance.
The participants in this case study were able to implement helpful, learned strategies into their home, work and social environments. They reported experiencing improved confidence and self-esteem following intervention, which resulted in positive feelings of well-being and overall improved quality of life. Positive well-being has implications for physical, mental and social health and is associated with better health outcomes and ultimately reduced healthcare burden. 55
Conclusion
The adults presented in this case study were diagnosed with CAPD based on their results of an audiological (including CAP) diagnostic test battery. A client-centered approach to management was adopted and included face-to-face training and home and work practice. Participants responded well to the auditory-based interventions and reported significant improvements in their symptoms and accompanying difficulties.
CAPD is traditionally and usually identified in childhood, and it is questionable whether these individuals missed diagnosis during childhood or whether the difficulties appeared only in later life. Nonetheless, the study presents evidence for the presence of CAPD in adults, although, surprisingly first diagnosed in adulthood.
CAPD may be comorbid with other disorders or difficulties. However, the adults’ positive responses to the auditory-based interventions used in their management plan confirm the influence of the disorder on a variety of work and social functions. Participants-reported improvement post intervention suggest that young and middle-aged adults are not too old to be tested for CAPD and can benefit from an aural rehabilitation program targeting their CAP, listening and associated skills. Further research investigating CAPD in adults is essential so that adults can improve their well-being and quality of life. These case studies highlight that adults with CAPD are an under-diagnosed segment of the population. Medical and other allied health professionals should be alerted to the possibility of presentation of CAPD in adulthood in order to make appropriate referrals for CAP testing to facilitate diagnosis and appropriate intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case series was obtained from La Trobe University Human Ethics Committee (approval number/id: HEC18134)*.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.