
Abstract
Schwannoma is a slow-growing, benign tumor of the nerve sheath. It rarely presents in the nasal cavity or the paranasal sinuses. Although schwannomas in the nasal septum have been reported previously, cases of this tumor in the nasal columella are rare in the literature. Here, we report on a 67-year-old woman with a schwannoma in the nasal columella that was successfully removed using a sublabial approach, along with a review of relevant literature.
Introduction
Schwannoma is a benign, slow-growing tumor arising from Schwann cells of the cranial, peripheral, and autonomic nerves. Schwannoma is common in the head and neck region (~25%–45%) but uncommon in the nasal cavity and paranasal sinuses, accounting for 4% of head and neck schwannomas.1–3 The area most commonly associated with schwannoma of the nasal cavity and paranasal sinuses is the nasal septum,1,3,4 approximately 31 cases have been reported to date. 4 To the best of our knowledge, schwannoma in the nasal columella is extremely rare as only four cases have been reported in the English-language literature.2,5,6 We report this rare case of schwannoma in the nasal columella, with a review of the relevant literature.
Case report
A 67-year-old woman with a 10-month history of widening of the nasal columella and a 5-month history of nasal pain was referred to our clinic. She had no rhinologic symptoms save for a bilateral nasal obstruction. On physical examination, she showed partial obstruction of both nostrils due to widening of the nasal columella as well as hypervascularity of the columellar skin (Figure 1). A smooth, soft, well-circumscribed mass around the superior labial frenulum was palpable. Nasal endoscopy revealed a normal septum and nasal cavity. The contrast-enhanced computed tomography (CT) scan revealed heterogeneous soft-tissue density without enhancement in the front of anterior nasal spine and no invasion of the structures surrounding the mass (Figure 2).
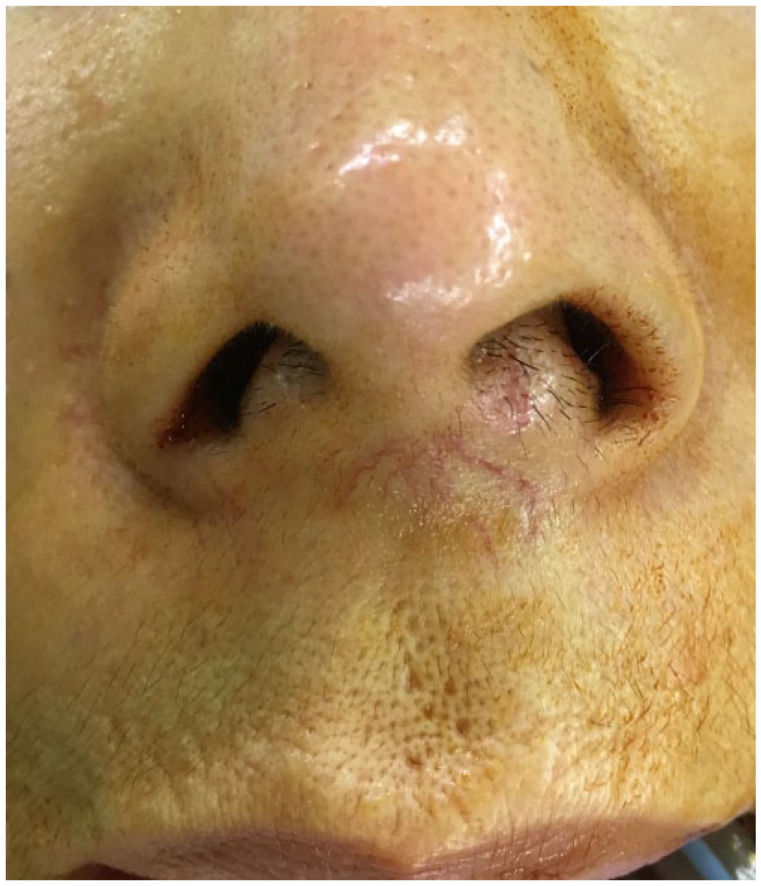
Preoperative view showing columellar widening and hypervascularity of the columellar skin.

Contrast-enhanced computed tomography scan showing a heterogeneous soft-tissue mass without contrast enhancement (white arrow) around the anterior nasal spine. ((a): axial and (b): coronal).
The patient underwent complete mass excision via a gingivobuccal incision under general anesthesia. A soft, well-encapsulated mass was observed under mucosa, which showed no adhesions to the surrounding structures (Figure 3). The mass was yellowish, soft, and round in shape, measuring about 2.1 cm × 2 cm in size. Intraoperative frozen biopsy was performed and revealed a spindle cell tumor. Considering the possibility of schwannoma, the nerve of origin for the tumor was explored for during the dissection, but could not be identified.

Intraoperative view of the tumor after gingivolabial incision was performed, showing a well-encapsulated mass.
The histopathologic examination showed areas of hypercellularity (Antoni A) and hypocellularity (Antoni B). The Antoni A region was composed of spindle-shape cells with hyperchromatic nuclei (Figure 4(a)). Immunohistochemical staining showed that the tumor was positive for S-100 (Figure 4(b)) but negative for smooth muscle actin. Therefore, the pathologic diagnosis was confirmed as schwannoma.

(a) Histopathologic photomicrograph demonstrating a high density of cellular spindle-shape cells with hyperchromatic nuclei (hematoxylin and eosin, ×200) and (b) immunohistochemical stain showing positivity for S-100 protein.
Postoperative neural deficit and cosmetic problems were not observed, and the patient had no sign of recurrence during the 2-year follow-up period.
Discussion
The most commonly occurring benign neurogenic tumors are schwannoma and neurofibroma. Although neurofibroma is a tumor with multiple lesions with a high risk of malignant transformation, schwannoma is a solitary, slow growing, encapsulated tumor with low risk of malignant change. 3 It has been reported that schwannoma in the head and neck region accounts for 25%–45% of all cases.1–3 Schwannomas of the head and neck are divided into intracranial acoustic schwannomas and non-vestibular extracranial head and neck schwannomas, depending on their location. 7 Non-vestibular extracranial head and neck schwannoma is more common than intracranial acoustic schwannoma. The most common site for non-vestibular extracranial head and neck schwannoma is the parapharyngeal space. Although the nasal cavity and paranasal sinuses are supplied with abundant nerves, 5 schwannoma in these areas is uncommon, accounting for 4% of head and neck schwannomas.1–3 Schwannoma in the nasal columella is extremely rare. Schwannoma in the nasal columella is postulated to originate from the infraorbital nerve, the external branch of the anterior ethmoidal nerve, or an autonomic nerve. It has been reported that it is difficult to identify the nerve of origin intraoperatively;1,3,4 the nerve of origin was not identified in our case as well. We surmised that this schwannoma might have arisen from a peripheral branch of the infraorbital nerve because of the tumor location in the lower half of the nasal columella.
The clinical symptoms of both inflammatory sinonasal disorder and a schwannoma in the nasal cavity or paranasal sinuses are similar. The most common symptoms of this tumor are nasal obstruction, epistaxis, nasal pain, mucopurulent discharge, and anosmia. Hypoesthesia or paresthesia can be a presenting complaint in consequence of the compression of the involved nerve. 3 This tumor may have a delayed diagnosis because it has no specific, unique symptoms. Patients with a tumor in the nasal columella could present with esthetic complaints such as columellar widening rather than rhinologic symptoms.2,5 The differential diagnosis of the lesion includes abscess, hemangioma, fibroma, lipoma, granuloma, and mucocele. 6 Although schwannoma shows no typical findings on imaging studies, these are important when planning the surgical approach. The common findings of schwannoma on a contrast-enhanced CT scan are a mottled appearance with peripheral intensification and bony erosion with destruction.1,4 A CT can be helpful for delineating the relationship of the lesion to the surrounding bony structures, but it might be difficult for differentiating schwannomas from inflammation and other tumors on imaging alone.1,2 Magnetic resonance imaging (MRI) is useful in this regard. Schwannomas exhibit various signals ranging from hyperintense to hypointense on T1-weighted MRI and hyperintense on T2-weighted MRI.2,8 Imaging studies of schwannoma might be more helpful in identifying accurately the area of tumor extension and selecting the surgical technique rather than for diagnosis.
Macroscopically, schwannomas appear as well-circumscribed, encapsulated masses with a gelatinous or cystic appearance. Microscopically, schwannomas exhibit two distinct histologic patterns of Antoni A and Antoni B areas. Antoni A areas are composed of a dense cellular arrangement and may have nuclear palisading, referred to as Verocay bodies. On the other hand, Antoni B areas consist of a low density of intercellular arrangement.1,8 Because the S-100 protein occurs in central and peripheral nerve cells, immunohistochemistry stains for S-100 may be helpful for the diagnosis of schwannomas that do not demonstrate the characteristic histologic findings such as Antoni A or B. 3
The treatment of choice for nasal schwannomas is complete excision. Various surgical approaches such as lateral rhinotomy, Caldwell-Luc approach, midface de-gloving, or endoscopic approach are employed to completely remove the tumor; the approach should be chosen according to the size, localization, and extension of the tumor mass. The open rhinoplasty approach is primarily used for excision of schwannoma in the nasal columella.2,5,6 This approach is useful for removing the tumor involving the nasal tip. 6 In our case, the patient underwent complete excision through a sublabial approach, not open rhinoplasty. We think that complete excision by sublabial approach would be sufficient for schwannoma confined to the columella and not involving the nasal tip; this approach also causes less scarring.
Conclusion
The schwannoma, uncommonly presenting in the nasal cavity and paranasal sinuses, is rarely reported in the nasal columella. However, we consider that the differential diagnosis for tumors in nasal columella should include schwannoma. Although an open-rhinoplasty approach is most commonly used to remove schwannoma in the nasal columella, we propose that a sublabial approach is sufficient to remove this tumor, if it has not extended to the nasal tip.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.