
Abstract
Sinonasal schwannoma (SNS) is a rare entity with 4% occurring at this location and only 36 cases described in the literature. A 22-year-old woman presented recurrent unilateral epistaxis, hyposmia, unilateral nasal obstruction, and hemicranial headache for a year. The endoscopic examination showed a tissue mass filling the left nasal cavity and nasopharynx. Imaging showed a mass that occupied the left posterior ethmoid cells in the hyposignal T1, hyposignal T2, and gadolinium enhancing. A preoperative biopsy was made and the diagnosis was a schwannoma. The tumor mass was completely removed under general anesthesia. The final histopathological study reconfirmed the diagnosis of schwannoma. Six months after surgery, control endoscopic and imaging showed the absence of tumor recurrence. SNS is a rare entity and its diagnosis is generally based on a histological examination. Therefore, the possibility of schwannoma must be considered in front of a mass of the nasal fossa.
Background
Schwannomas are benign tumors arising from Schwann cells. 1 Schwannomas can be ubiquitous; their location in the head and neck represents 25%–45% with a preferred vestibular nerve location. 2
Schwannoma rarely involves the nasal cavity and paranasal sinuses, the incidence rate reported is 4% with over 100 cases in the literature. 3
We describe the presentation, radiologic findings, and treatment of a patient with an ethmoidal schwannoma.
Case report
A 22-year-old woman attended the ENT department with a history of nasal obstruction, hyposmia, left-sided headache, and two episodes of mild left epistaxis. Nasal endoscopy showed a smooth mass totally occluding the left nasal side extended to the choana (Figure 1). A computed tomography (CT) scan demonstrated the total opacity of posterior ethmoid cells, extended to the middle homolateral meatus, and reached the inferior part of the middle turbinate (Figure 2). Magnetic resonance imaging showed the mass arising from the sphenoethmoidal recess in the hyposignal T1 and the hyposignal T2 with significant enhancement of gadolinium (Figure 3). An endoscopic biopsy was performed and the result of histopathological examination was schwannoma. Endoscopic sinus surgery was performed under general anesthesia and the tumor located at the level of the left sphenoethmoidal recess was completely removed after a partial resection of the middle turbinate. The final histopathological study of the mass confirmed the diagnosis of schwannoma and showed hypocellular myxoid Antoni B areas with Verocay bodies. Immunoperoxidase stains for S100 were positive (Figure 4). Six months after surgery, the control magnetic resonance showed an absence of tumor recurrence. The patient was symptom-free and had no recurrence after 20 months.

Endoscopic view of the left nasal cavity.

Axial CT SCAN shows left mass in the nasal cavity.

Axial T2-weighted MR image shows left posterior ethmoidal mass.
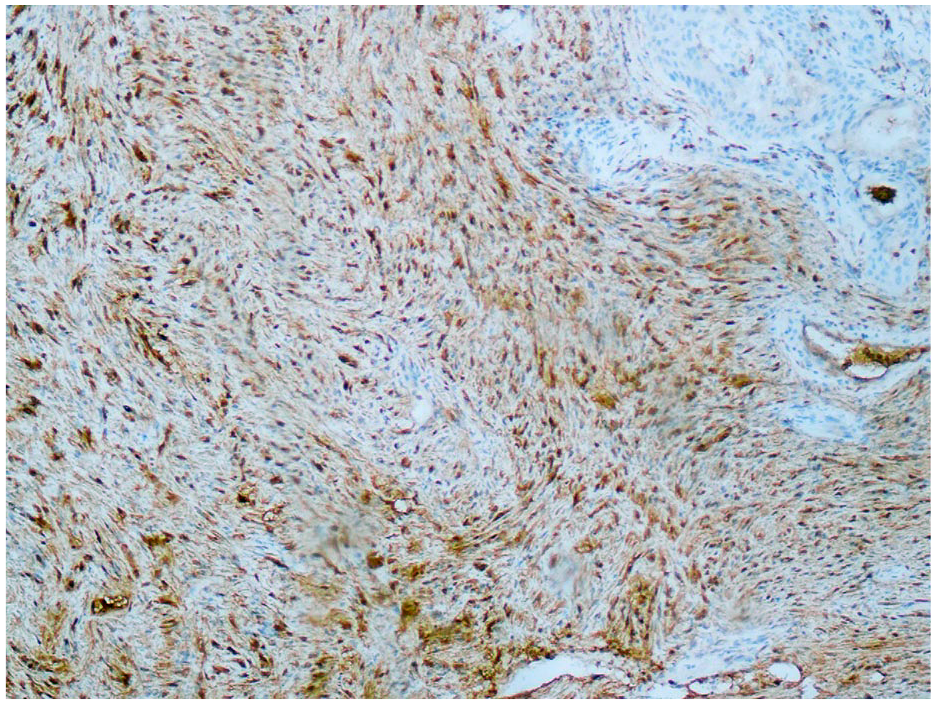
The tumor is PS100 positive.
Discussion
Sinonasal schwannoma (SNS) is commonly misdiagnosed with other sinonasal tumors because it lacks specific clinical symptoms. 4 Patients can present with a variety of nonspecific clinical symptoms that depend on the location and extension of the tumor. SNS are rare lesions with no age or gender predilection. It is suggested that SNS emanate from the branches of the trigeminal nerve or parasympathetic nerves to the septal vessels and mucosa. 5
Due to its complex innervation, the most common sites of SNS are the nasal septum, maxillary sinus and ethmoid sinus.
Macroscopically, SNS is a non-encapsulated mass in contrast to head and neck schwannomas which are well-defined capsuled tumors. 6 This particularity was explained by the origin from sinonasal mucosal autonomic nerves which lack a perineural layer.
Our patient was found to have a non-encapsulated tumor like most cases in literature.
Microscopically, schwannomas have biphasic components such as dense hypercellular areas (Antoni A) and myxoid hypocellular areas (Antoni B). 7 Diffuse strong expression of S100 confirms neural-derived tumors. The malignant transformation of schwannomas is exceptional. 7 Although extremely rare, the possibility of neurofibromatosis (NF) should not be forgotten and a careful examination should be performed to confirm a sporadic form of schwannoma.
Imaging can help characterize the mass and its extension. A CT scan usually shows the size and extent of the tumor and the presence of any bony erosions. The preoperative imaging of choice for schwannoma is MRI, which enables more specific findings than a CT scan. The majority of SNS have a highly dense cellular resulting in low T2 signal intensity on MRI. A preoperative biopsy may be recommended to eliminate other sinonasal tumors, especially malignant ones.
The mainstay treatment for schwannoma is surgical excision. The choice of the approach is conditioned on different factors such as the size, location, and extent tumor. 8 Endoscopic resection can be performed securely for small schwannomas with limited extension, otherwise, an external approach is required for giant tumors that extend to the anterior skull base. 9 Although recurrence is rare after removal, a few cases of malignant transformation have been reported. Therefore, regular long-term follow-up is required.
Conclusions
Although SNS is a rare tumor, this case report emphasizes the need to keep in mind schwannoma in any differential diagnosis of any unilateral mass of the sinonasal cavity. A preoperative biopsy may be useful to confirm the histopathological diagnosis of schannoma before choosing the surgical approach. Due to the fact of the benignity of this tumor, a mini-invasive endoscopic surgery is the optimal treatment when tumor extension is limited.
Footnotes
Author contributions
H.C. was a doctor in charge of a patient, initiated the study, and wrote the manuscript. A.H. was a doctor in charge of a patient and wrote and edited the manuscript. S.T. wrote and edited the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
Written informed consent for publication of patient’s clinical details and clinical images was obtained from the patient.