
Abstract
C-MAC® video-laryngoscope is often used by anesthetists in difficult intubation scenarios primarily in adults. Using this C-MAC® device in two of our pediatric cases, we successfully removed the laryngeal foreign body, while the anesthetist provided the apneic technique. A systematic review of PubMed and Google Scholar for similar cases was conducted. We found only one such case report of pediatric airway foreign body removal via video-laryngoscope in the English literature. The use of this high-quality, magnified video-laryngoscope in children in an emergency scenario is often not adequately applied. This procedure provides continuous real-time visualization to both the operating surgeon as well as the anesthetist in respect to the airway and thereby reduces the chance of any untoward complications. Here, we present two interesting case reports of C-MAC® video-laryngoscope assisted removal of laryngeal foreign body via apneic technique with spontaneous ventilation performed on two different children in our facility. Both these children had clinical symptoms of upper airway obstruction with fluctuating stridor simulating croup or asthma.
Introduction
In the era of emerging technological advances, one cannot underestimate the importance of newer video-laryngoscopic devices such as C-MAC® (Karl-Storz, Tuttlingen, Germany), Glidescope® and KingVision in the management and photo-documentation of difficult foreign body airway cases especially in the pediatric population. In children less than 4 years of age, foreign body aspiration is the leading cause of accidental death. 1 Rigid endoscopies are the preferred method for the removal of laryngeal foreign bodies and the foreign body lodged between the vocal cords at the glottic level was a challenge to both the anesthetist and the otolaryngologist. This modified our approach to the use of a video-laryngoscope to secure the airway quickly without extensive manipulation and under complete vision of the entire operating room team for a co-ordinated rescue. Ours is the second such case report of pediatric airway foreign body removal via video-laryngoscope, the first being reported by Laura Warner 2 The C-MAC® is an indirect video-laryngoscope that has a crucial role in the management of difficult airway. 3
Case report 1
A 1-year-old female child was referred to our facility NMC Specialty Hospital, Abu Dhabi, on 7 January 2018 with a history of definite foreign body aspiration of a blue colored star shaped plastic object while playing with it 2 days ago. She presented with biphasic stridor, dehydration with repeated bouts of vomiting and retching whenever any attempt to feed her was made. A plain X-ray neck anteroposterior view (Figure 1(a)) showed a 1 cm long linear radio-opaque object. A flexible laryngoscopy was also attempted in the initial local hospital but due to non-compliance, the procedure could not be completed. In view of an already 2-day-old history of foreign body ingestion, deteriorating symptoms of the child, we immediately posted the child under general anesthesia. While the child was preoxygenated via a face mask, anesthesia was induced with sevoflurane, IV fentanyl and spontaneous ventilation was achieved via apneic technique. The depth of anesthesia was monitored continuously by the anesthetist. Video-laryngoscope C-MAC® using a pediatric blade revealed a blue-colored plastic star with one of the projections lodged below glottis and one in between the vocal cords which was removed with a pediatric Magill’s forceps (Figure 1(b)). IV hydrocortisone 15 mg was then instituted for mild edema of the injured subglottic area. IV infusion of ringer lactate 500 mL was also initiated for rehydration. Child began oral feeding with no complications after 2 h and was discharged on the same day.
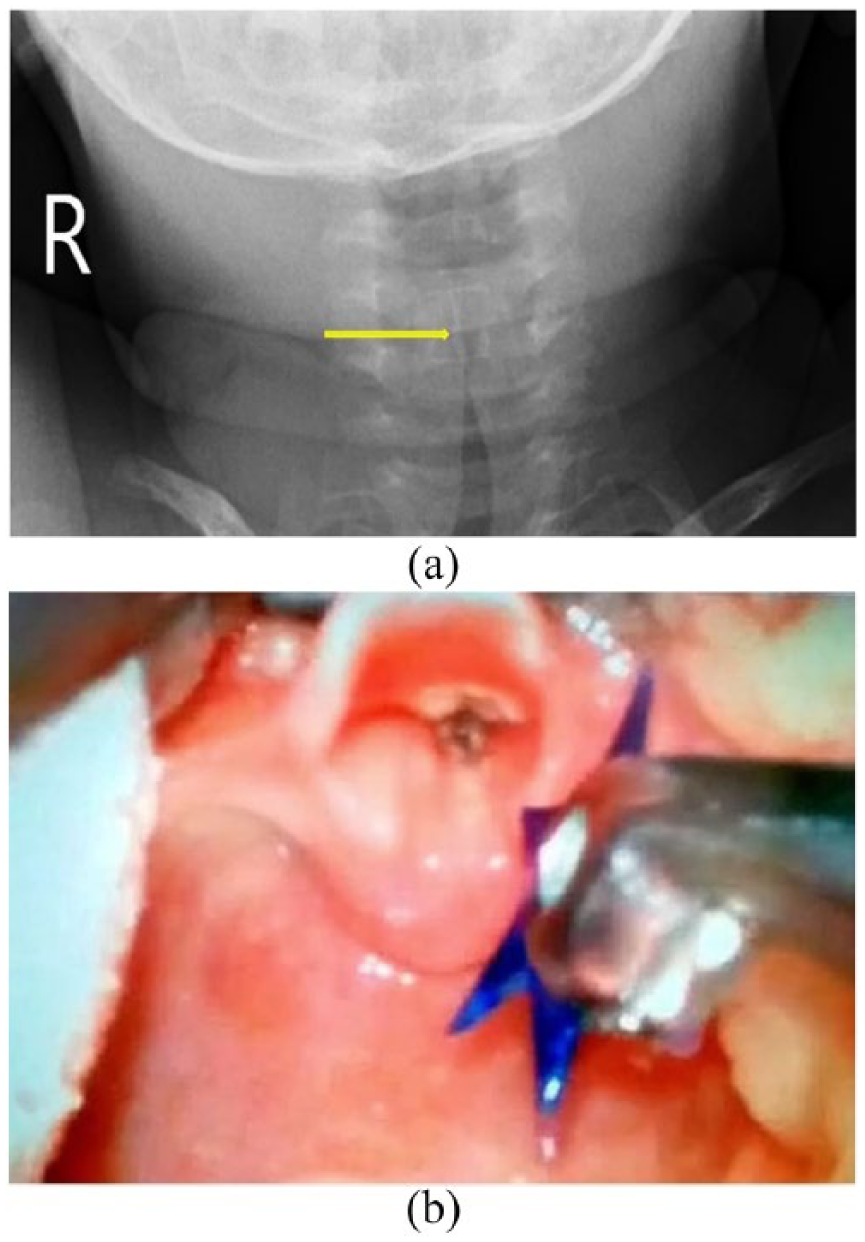
(a) Arrow showing 1 cm long and short projection of the foreign body(star) lodged in airway of child’s sub-glottis in X-ray neck anteroposterior view in case 1 and (b) a C-MAC® video-laryngoscope magnified monitor view of a removal in progress of a blue plastic star lodged in glottis in case 1.
Case report 2
A 2 year 11 month–old male child was referred to our ENT Department on 9 July 2013 with complaints of initial paroxysms of cough, difficulty breathing and mild wheezing following ingestion of fish a day ago. Although the child had a medical history of bronchial asthma, he showed no signs or symptoms of fever, vomiting or drooling of saliva. A prior history of a coin extraction by the gastroenterologist was elicited. The oropharyngeal and chest examination revealed no abnormal findings although the child produced a croup like sound on each inspiration. The oxygen saturation level was 98%. A plain X-ray neck anteroposterior and lateral view revealed a 2.2-cm long linear radio-opaque object lodged in the crico-pharyngeal region at C5–C6 level overlapping the larynx with no retropharyngeal soft tissue enlargement (Figure 2(a) and (b)). The child was promptly posted for an emergency foreign body removal under general anesthesia.

X-ray neck anteroposterior and lateral view showing sharp radio-opaque foreign body as shown by arrows in the crico-pharyngeal region at C5–C6 level overlapping the larynx in case 2.
General anesthetic agents like sevoflurane, nitrous oxide and oxygen were administered via mask airway inhalation. A pediatric Macintosh laryngoscope view showed a definite foreign body, lodged below and between the vocal cords in left subglottic area with surrounding edematous mucosa. So, it was decided to use an apneic technique with spontaneous ventilation thereby avoiding the jet ventilation due to fear of displacing the foreign body. After mask ventilation, a nasal intubation with a flexo-metallic tube was done up until the level of the upper larynx for intra-operative ventilation safety and back up. The depth of anesthesia was monitored continuously by the anesthetist. The C-MAC® video-laryngoscope visualization showed a peculiar W shaped fish bone with sharp projections lodged between and below the vocal cords which was grasped and removed with a foreign body removal forceps (Figure 2(c)). Postoperatively, paracetamol rectal suppository, IV Hydrocortisone 50 mg for the edema and maintenance IV fluids were given following which the child had an uneventful recovery.
In both of our cases, the children were preoperatively stable and no adverse events such as laryngeal or bronchial spasms, body movements or arrhythmias occurred intraoperatively. Back up endoscopy set and unit was also kept ready in case we needed to convert to a longer procedure for extraction of the foreign body.
Discussion
Vast majority of foreign body aspirations occur in children less than 3 years of age and more often in a male child due to their habit of exploring objects in the mouth such as a particular food item or non-food items like pen caps, pins and paper clips while the actual event of aspiration is frequently unwitnessed. 1 Halvorson et al. reported that subglottic foreign bodies pose a diagnostic challenge and in majority of the cases there is a delay in diagnosis. 4 Any delay in diagnosis causes increased morbidity from bronchial inflammation, obstruction and pneumonia which is resistant to treatment.
In terms of location, inhaled foreign bodies most often get lodged in the bronchi; laryngotracheal foreign bodies that occur are potentially more dangerous.4,5 The reported incidence of laryngeal lodgment of aspirated foreign bodies varies from 2% to 11%.6,7 According to a study conducted by Onotai et al., 8 supra-glottis is the commonest location of impacted foreign bodies in the larynx of Nigerian children. Impacted subglottic foreign bodies may produce upper airway obstruction and clinical signs simulating croup and asthma. 9
A meticulous history, physical examination with high degree of suspicion and early recognition of airway compromise are keystones to diagnosing such foreign body in the airway; thus, improving prognosis. Sudden and quick upper airway obstruction ensues in children due to their smaller airways; symptoms being dyspnea, tachypnea, stridor, spasmodic cough, change in voice and cyanosis. The severity of the symptoms depends on the location, mass effect, shape, character and duration of foreign body present in the upper aerodigestive tract. In challenging cases of impacted upper airway foreign body with airway compromise and severe stridor, a tracheostomy or crico-thyroidotomy may be necessary in spite of a standard endoscopic technique. An urgent team response in such cases of complete obstruction can prevent impending respiratory failure and thereby averting a cardiac arrest. In the second case report, with a subglottic impacted foreign body presenting with mild to moderate stridor, video-laryngoscope C-MAC® assisted foreign body removal became vital in the meticulous removal to avoid a laceration or perforation of the airway.
The mobile C-MAC® video-laryngoscope is a relatively new device with the unique advantage of providing both a direct laryngoscopic view and a camera view displayed on the video monitor. 10 It can create a continuous video recording or static pictures on to a removable secure digital card. 11 A significantly enhanced laryngeal view is obtained especially in difficult airway cases when compared to direct laryngoscopy with a Macintosh laryngoscope blade. 12 This provides an additional photo-documentation for record and review of case details which is excellent in academic teaching and training sessions. Different blade sizes either the re-usable or the disposable ones are available for neonatal, pediatric and adult groups. In addition, video-laryngoscope has been used in tongue base radiofrequency for the treatment of obstructive sleep apnea, upper aerodigestive tract excisional biopsies and for hypopharyngeal foreign body removal especially in difficult intubation cases. 13 Cagini et al. 14 recommended using video-laryngoscope due to the benefits offered by magnified visualization and under conscious sedation in adults in the removal of small and thin foreign bodies that are not readily detected by radiological examination or in those not readily identified by direct endoscopy.
Video-laryngoscope has often been used by the anesthetists for difficult intubation scenarios and the C-MAC® video-laryngoscope is usually not considered as a first choice by an otolaryngologist especially in pediatric cases of foreign body impaction of the airway. Both our cases demonstrates the ease and reduced procedure time with effective extraction of the foreign body as supported by a similar case report by Laura Warner. 2 Endotracheal intubation was not an option for conventional ventilating in both our cases as the foreign body was located at the glottic level between the cords. Flexible fiberoptic bronchoscopy is the gold standard in diagnosis of airway foreign bodies while inhaled foreign bodies are best removed using rigid endoscopes.
Individual situation warrants the choice of anesthesia as in inhalation or intravenous induction, spontaneous or controlled ventilation, and inhalational or intravenous maintenance. For short simple surgeries, intermittent apnea technique is performed wherein the anesthetist hyperventilates with 100% oxygen through a facemask or endotracheal tube and then the ventilation is temporarily stopped by removal of the facemask or endotracheal tube for a time frame of 2–5 min. Ventilation is reinitiated when SpO2 drops to 90%–92%. Preoxygenation extends the duration of safe apnea which is the time until the patient’s oxygen saturation reaches 88%–90%. Thus, alternating of ventilation and operation is performed until the end of surgery. The balance of the depth of anesthesia and stable spontaneous respiration is continuously monitored. 15 The limitation faced here is when the procedure maybe prolonged due to difficulties in extraction of the foreign body and then a rigid endoscope will be the next option. The most favorable anesthetic technique for managing children with foreign body aspiration has no general agreement in literature. Induction and maintenance with spontaneous ventilation in addition to supplementary nasal oxygen appears to be the most suitable technique for ENT endoscopies as demonstrated in two of our cases allowing for excellent visualization of laryngotracheal structures with the least risk of trauma. 16
The innumerable advantages that the video-laryngoscope offers in an emergency scenario over a standard direct laryngoscope are its ease, speed, safety and success. In the coming years, it is going to be another optional method for removal of non-impacted foreign body of upper respiratory tract. In addition, it provides the anesthetist with a continuous visual monitoring of the airway area which serves as a common area of interest to both the ENT surgeons and the anesthesia team alike.
Conclusion
Video-laryngoscopes such as C-MAC®, Glidescope® and King Vision are being commonly used in pre-hospital settings and in difficult intubation scenarios primarily in adults. The use of C-MAC® video-laryngoscope in pediatric airway obstruction due to foreign bodies via an apneic technique as a superior approach has been highlighted in both our cases and we would like to share this as an optional technique to be considered especially in pediatric cases. This facilitates for a safe, speedy and successful removal of the foreign body with respect to an unprotected airway wherein tracheal intubation is not a viable option. The enhanced view of the laryngeal inlet provided by the video-laryngoscope is ideal to tackle such notorious foreign bodies. An additional advantage is that it caters to a multidisciplinary team of both the anesthetist and the otolaryngologist having a continuous visualization of the airway thus executing an exemplary and co-ordinated rescue effort.
Footnotes
Acknowledgements
We, the authors acknowledge the immense help and support that we received from our NMC Healthcare group. Information on informed consent to report the individual case reports has been obtained from the patient(s) legally authorized representative.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.