
Abstract
Component malpositioning during Birmingham hip resurfacing increases the risk for component wear, metallosis, component loosening, and the likelihood of dislocation and revision surgery. Computer-assisted navigation can increase the accuracy to which components are placed, and the utilization of this technology in Birmingham hip resurfacing is increasing. The present report summarizes the accuracy of acetabular component positioning in a Birmingham hip resurfacing case utilizing navigation. Intraoperative C-arm fluoroscopy following the use of the navigation tool confirmed excellent seating, positioning, and stability of the acetabular component. In addition, post-operative antero-posterior radiographs confirmed device accuracy and revealed a stable joint with no evidence of acetabular loosening or femoral fracture. Computer-assisted navigation may therefore be an effective tool to improve the accuracy of component positioning during Birmingham hip resurfacing.
Keywords
Introduction
Hip resurfacing is a bone-sparing alternative to total hip replacement (THA) that accounts for approximately 1% of hip arthroplasties in the United States. 1 The Birmingham hip resurfacing (BHR) system (Smith & Nephew, Andover, MA, USA) is a US Food and Drug Administration (FDA)-approved metal-on-metal (MoM) implant, effective in providing joint stability and longevity to patients seeking less invasive surgical treatment for debilitating hip disease.2,3 As with THA, however, component malpositioning can lead to detrimental post-operative outcomes and is a leading cause of dislocation and revision surgery. 1 Computer-assisted navigation may help to reduce the risk of component malpositioning in such cases by improving the accuracy with which components are placed intraoperatively. Indeed, a growing body of literature shows promising results for the use of computer-assisted navigation in both THA 4 and hip resurfacing procedures.5–12 While resurfacing studies have largely evaluated the accuracy of computer-assisted navigation for femoral component placement,6–8,11,13 the accuracy of computer-assisted navigation associated with acetabular component positioning is less characterized.10,12 The present report summarizes the use of an emerging, imageless navigation tool in a case of BHR, where navigation accurately measured the acetabular component position intraoperatively.
Case report
Patient presentation
A 48-year-old male presented with a chief complaint of bilateral hip pain, more prominent on the right side. The pain was described as intermittent, but significantly progressing in the most recent year, with daily occurrence. The pain was constant and worsened when walking, during prolonged periods of sitting, with sitting to standing, and with physical exercises including running. The patient noted a severe limitation in mobility, experienced with simple activities such as putting on socks and shoes. Past medical, family, and social histories were unremarkable. Conservative management including anti-inflammatory medication, activity modification, icing, home exercising, stretching, and resting had not provided significant relief.
Orthopaedic examination and diagnosis
Initial orthopaedic examination of the right hip revealed a range of motion of 0° to 90° of flexion with pain at end range, internal rotation (IR) in flexion 5°, external rotation (ER) in flexion 40°, abduction 40°, and adduction 10°. Anterior impingement test on the right side and Patrick’s test to the groin were both positive. On examination of the left hip, range of motion was 0° to 95°, IR in flexion 10°, ER in flexion 50°, abduction 50°, and adduction 10°. Anterior impingement testing on the left was positive. Abductor strength was 5/5 bilaterally. No deformities were identified, and neurological status was intact.
Plain film radiographs revealed bilateral hip osteoarthritis with the presence of osteophytes, joint space narrowing, sclerosis, and cam-type femoroacetabular impingement (Figure 1). Based on patient history, age, and examination findings, final diagnosis was bilateral hip osteoarthritis, right hip greater than the left. Treatment options for the right hip included cortisone injection, THA, or BHR. After discussing the risks and benefits of each procedure, the patient opted for right BHR due to his active lifestyle.

Pre-operative radiograph: pre-operative AP plain film radiograph depicting bilateral hip osteoarthritis with the presence of osteophytes, joint space narrowing, sclerosis, and cam-type femoroacetabular impingement.
Treatment
Surgery was performed with the assistance of C-arm fluoroscopy and Intellijoint HIP® (Intellijoint Surgical Inc., Waterloo, ON, Canada; off-label use), a 3D mini-navigation tool currently approved for use in posterior, lateral, and direct anterior approaches for THA. While this device has received clearance from the FDA for use in primary and revision THA, it has not been evaluated for use in BHR. The posterior application of the navigation device was followed, which has been described in detail previously 14 (Figure 2).
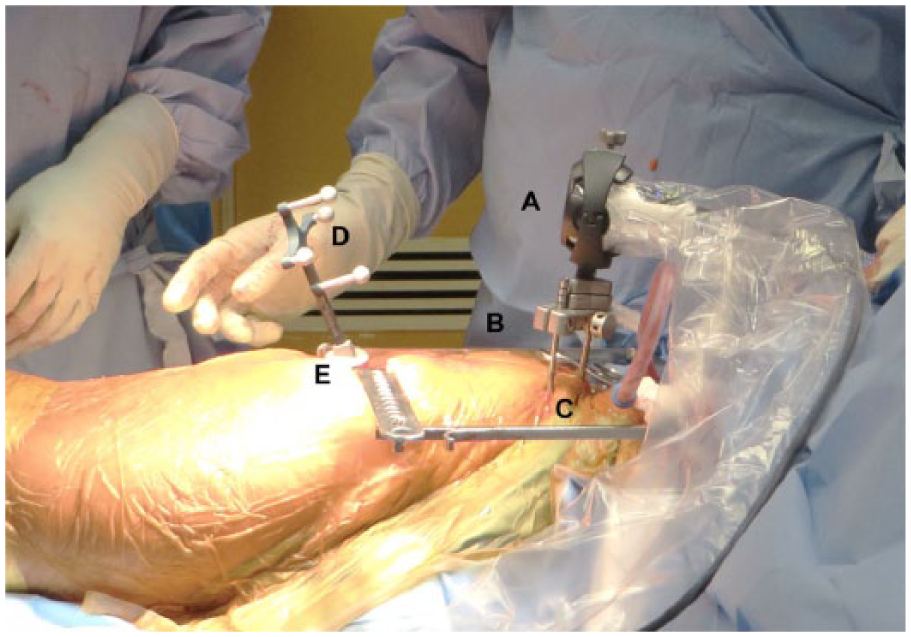
The Intellijoint HIP® navigation camera (A) is enclosed in a sterile drape and magnetically attaches to the pelvic platform (B). The pelvic platform is installed on the ipsilateral iliac crest using two pelvic screws (C). The tracker (D) is magnetically attached to the femoral platform (E). The camera captures movements of the tracker and relays the information to a workstation for review by the surgeon.
Surgical technique
The patient was placed right side up in the lateral decubitus position and stabilized using a pegboard. The right hip and lower extremity were prepped and draped in usual sterile fashion, followed by a confirmed surgical time out. Two 5-mm stab incisions were made at the iliac crest to accommodate the pelvic screws, pelvic platform, and camera of the navigation system, at which point the horizontal and frontal planes of the patient were registered. A 12-cm posterolateral incision was made and the tensor fascia latae and gluteus maximus fascia were incised. The sciatic nerve was palpated and protected. The gluteus medius and minimus were also protected. Short external rotators and quadratus femoris tissue were incised, leaving a cuff to prevent medial femoral circumflex bleeding. Hemostasis was adequate throughout the entire procedure and the sciatic nerve was palpated and protected throughout the entire procedure. A femoral disc was placed on the lesser trochanter to accommodate the tracker of the navigation tool. Hip biomechanics were registered including baseline leg length. Subsequently, the posterior capsule was incised in a U-shaped capsulotomy. The hip was dislocated atraumatically. Circumferential release of the capsule was performed. With the assistance of C-arm fluoroscopy, a guide pin was placed at the centre of the femoral neck at an angle of approximately 138°. C-arm fluoroscopy and biplanar imaging demonstrated excellent positioning of the guide. The femoral head was prepared per usual fashion using barrel reamer, chamfer reamer, and spherical reamer to create a spherical femoral head. At this point, a femoral cup trial was placed. Excellent fixation was noted without any notching or impingement. Next, the femur was transitioned anteriorly using assistance and blunt retractors. The acetabulum was visualized circumferentially with difficulty due to the stiffness of the hip. The labrum and pulvinar were excised and medial wall was visualized. Sequential reaming was performed. Medialization was excellent without a breach, with great cortical cancellous bleeding bed, and with sequential reamers in 1- and 2-mm increments. Next, a 58-mm acetabular component was impacted in place using the navigation system to confirm excellent angulation at 44° inclination and 20° anteversion, noting excellent seating, alignment, and stability. C-arm fluoroscopy demonstrated excellent positioning of the acetabular component with grade medialization and adequate seating. Next, Simplex cement was mixed per usual fashion and placed in the femoral head which was then impacted into place. Excellent fixation was noted. Cement was allowed to harden, with excess cement removed. Hip was relocated atraumatically. Hip range of motion and stability tested excellent. The navigation system was utilized to confirm baseline leg length restoration, followed by the removal of all navigation-related materials. Copious lavage was performed followed by closure. Skin glue was applied. Aquacel dressing was placed. Patient was awakened, extubated, and brought back to the recovery room in stable condition with no complications noted.
Follow-up
Post-operatively, the patient was doing extremely well with no pain and full return of mobility. At his 12-week follow-up visit, the patient stated he was back to most of his physical activities and was happy with his progress. An antero-posterior (AP) pelvis x-ray of the right hip showed BHR that was well aligned with no evidence of loosening and no femoral neck fracture (Figure 3).

Post-operative radiograph: a 12-week, AP pelvis radiograph is depicted, showing BHR that is well aligned with no evidence of loosening and no femoral neck fracture. TraumaCad overlay (Brainlab, Chicago, IL, USA) depicts post-operative cup position measured at 46° inclination and 17° anteversion.
Discussion
BHR is considered safe and stable, as many cases describe strong mid- to long-term results, including 88%–99% joint survivorship reported at ⩾5 years.15,16 Commonly performed in younger, active, adult males, BHR conserves the femoral head and can produce excellent functional scores post-operatively.3,17 However, incorrect positioning of components during BHR can lead to early complications and early BHR failure.18,19 While inaccuracies in positioning related to the femoral component increase the risk of loosening and fracture,20,21 acetabular component malposition is associated with accelerated wear, impingement, and early dislocation. 22 The utilization of computer-assisted navigation during resurfacing procedures has largely focused on the positioning of the femoral component.6–8,11,13 In the present report, the accuracy of a navigation tool for acetabular measurements (anteversion and inclination) and leg length during BHR was evaluated.
Following patient registration and hip exposure, device measurements of intraoperative cup position were relayed in real time and allowed for a final intraoperative position of 44° inclination and 20° anteversion, selected by the operating surgeon (R.S.). Following navigation, excellent seating, alignment, and stability of the acetabular component were confirmed using C-arm fluoroscopy. Post-operatively, radiographic analysis (TraumaCad; Brainlab) measured a final cup position of 46° inclination and 17° anteversion, indicating device accuracy to within 2° and 3° of radiographic values (Figure 3). The device was also utilized intraoperatively to monitor leg length and ensured restoration following hip relocation. This was confirmed radiographically, as a 1-mm difference in leg length was observed between pre- and post-operative radiographic measurements.
These results are consistent with previous reports confirming the accuracy of computer-assisted navigation in resurfacing.10,12 A recent study by Vigdorchik et al. 12 utilizing the same navigation tool reported device accuracy to within 0.7° and 3° of post-operative radiographic values and restored a pre-operative 3-mm leg length discrepancy to 0 mm following the procedure. In turn, Romanowski and Swank 10 assessed inclination accuracy following the use of intraoperative navigation and reported no significant difference between pre- and post-operative inclination measurements. The ability of computer-assisted navigation to accurately match target values of cup position is critical for reducing the risk of adverse patient outcomes, such as accelerated component wear resulting from steep inclination angles.23,24 The present report showcased the ability of computer-assisted navigation to accurately measure cup position intraoperatively. Adverse outcomes may be preventable with technologies that promote accuracy and reduce the risk of component wear resulting from component malposition.
Limitations of this study first include the inability of the navigation tool to assist with guidance of the femoral pin and cap. This restricted navigation assistance to the acetabular component only. However, this was accommodated for with the use of C-arm fluoroscopy to visualize femoral component position. In turn, the device was able to track leg length changes throughout surgery and accurately restored leg length to within 1° of the radiographic pre-operative position. This is of value as leg length discrepancies are now a leading cause for litigation against orthopaedic surgeons following THA. 25 The second major limitation of these findings is the singular case examined. The use of the navigation tool in the present report shows promising results for acetabular component navigation during BHR, but further clinical evidence is required. While the device was able to accurately measure anteversion and inclination intraoperatively, these findings should be tested in a larger sample size.
Conclusion
The present case reported a BHR procedure, wherein the utilization of an imageless navigation tool allowed for accurate component positioning and leg length restoration. These findings are congruent with previous reports on the utilization of computer-assisted navigation during hip resurfacing procedures and provide further insight for the benefits of navigation in BHR specifically.
Footnotes
Acknowledgements
The authors would like to thank Nancy Cipparrone, for her assistance in gathering medical information for the present report.
Declaration of conflicting interests
R.S. has received consultancy fees from Intellijoint Surgical, Inc. J.R.B. and J.M.M. are both employees of and hold equity with Intellijoint Surgical, Inc.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.