
Abstract
Traumatic hemothorax is usually caused by thoracic organ damage. Cases of atypical bleeding sources may be difficult to diagnose. Here we present two surgical cases of vertebral fracture that caused hemothorax. Case 1: an 81-year-old man was admitted to our hospital after a fall. Computed tomography showed right hemothorax without rib fractures. He suddenly developed shock and intrathoracic hemorrhage. Thoracotomy revealed the bleeding source as a transverse laceration in T7. Case 2: an 83-year-old woman fell on her back and was admitted. Computed tomography indicated an L1 vertebral fracture. A few days later, she suddenly developed a right hemothorax. An intrathoracic hemorrhage was sustained after transcatheter embolization. Thoracotomy revealed a diaphragmatic rupture. Total cross-fracture of the vertebral body solely caused the hemothorax. If bleeding source is unclear in elderly patients, this etiology should be considered. We saved both patients by performing spinal fusion surgery at the appropriate time.
Introduction
Hemothorax, which commonly manifests in patients with major trauma, is primarily due to chest wall vessel damage and pulmonary injury accompanied by rib fractures 1 and presents similarly to case of delayed hemothorax after blunt chest trauma.2,3 If these typical findings at the time of admission are absent, the choice of initial treatment becomes unclear and patients may follow an unexpected clinical course. Here we report on a life-saving treatment strategy involving thoracotomy in two cases of massive hemothorax due solely to a chance-type vertebral fracture.
Case presentation
Case 1: an 81-year-old man was taken to our hospital after falling from his roof and reporting dorsolateral chest pain. He was conscious and alert and his vital signs were within the normal range. Chest radiography and ultrasonography in the emergency room showed neither a pneumothorax nor a pleural effusion. Contrast-enhanced computed tomography (CT) showed a right-sided hemothorax (Figure 1(a)). No obvious rib fractures or pulmonary injuries were noted. After admission, he suddenly developed shock and his blood pressure plummeted. A chest tube was inserted, and a total of 1330 mL of bloody pleural fluid was drained. However, the bleeding persisted and his condition did not improve. Thus, emergency surgery was indicated, and a right-sided thoracotomy was performed. The hematoma was removed and the active bleeding site was identified as a transverse fracture in the vertebral body of T7 (Figure 1(b)). Bone wax applied to the deep laceration of the vertebral body effectively stopped the bleeding. To prevent loosening of the bone wax, we affixed a sealant (TachoSil®, CSL Behring, Japan) to the lesion. A chest tube was placed to drain the pleural fluid of a contralateral hemothorax. The intrathoracic bleeding stopped and his status improved. Orthopedic surgeons diagnosed this vertebral injury as a chance-type fracture at T7 (Figure 1(c)). To ensure spinal stability, spinal fusion surgery was performed the following day. All chest tubes were withdrawn by the 5th postoperative day without any recurrence of the hemothorax. The patient recovered and was eventually discharged. Case 2: An 83-year-old woman fell on her back and was transferred to our hospital. She was taking medications for osteoporosis and had a history of a similar accident 5 years earlier. She was complaining of back pain, but there were no other abnormal findings. An imaging examination revealed a chance-type fracture at L1; no thoracic injury or abdominal ascites was noted (Figure 2(a)). She was hospitalized for elective spinal fusion surgery. Two days later, her condition suddenly deteriorated and she subsequently developed shock. Urgent imaging showed a right-sided hemothorax (Figure 2(b)) and a large hematoma around the vertebral body of L1, which was suspected to be actively bleeding due to an aortic injury. Because her vital signs improved with blood transfusion, aortography was performed, which revealed contrast extravasation from the first lumbar artery (Figure 2(c)) that was then arrested by transcatheter embolization. A right conventional tube was inserted, and 2000 mL of bloody pleural fluid was immediately drained. Although her clinical status improved, 1000 mL of bloody fluid drained the next day. The same day, spinal fusion was performed, followed by an exploratory thoracotomy. The right-sided thoracotomy revealed a moderate volume of bloody fluid and the absence of an intercostal vessel injury. A 70-mm diaphragmatic rupture running perpendicularly to the muscle fibers was identified and repaired. She recovered well after surgery without further bleeding and was transferred to a different hospital for physiotherapy on the 28th postoperative day.

(a) Computed tomography (CT) showed right-sided hemothorax with contrast extravasation (arrow). (b) Thoracotomy revealed active bleeding arising from a transverse laceration at T7. (c) Magnetic resonance imaging showed chance-type fracture at T7 (circle).
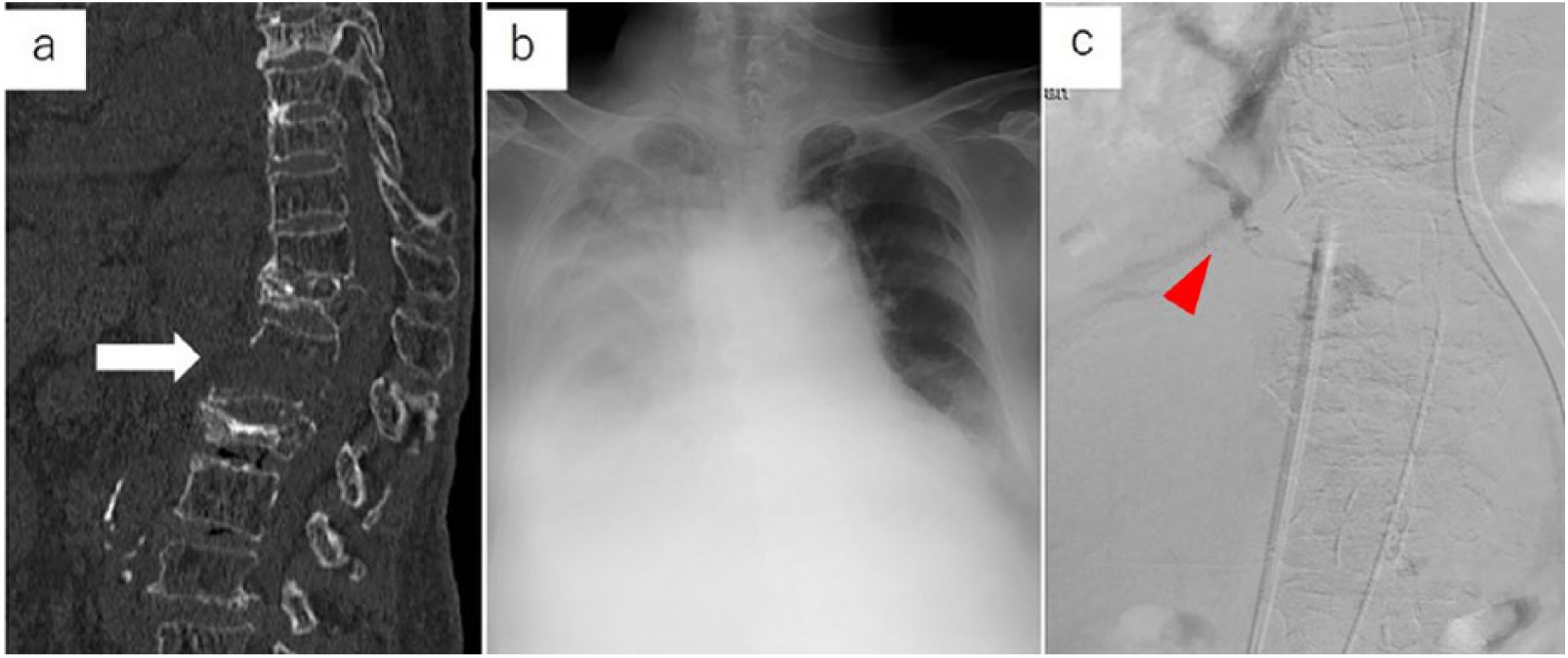
(a) CT showed chance-type fracture at L1 with dislocation (arrow). (b) Chest radiography showed massive right-sided pleural effusion. (c) Aortography revealed extravasation of the contrast from the first lumbar artery into the thoracic cavity (arrow).
Discussion
Hemothorax is often associated with blunt trauma. In most cases, the source of bleeding is the intercostal vessel and intrathoracic organs.1–3 In the cases described here, aside from the absence of multiple traumatic findings, damage to the chest wall and mediastinum was unclear, leading to initial management difficulties. In Case 1, despite the lack of rib fractures, CT showed contrast extravasation, suggesting bleeding from the intercostal artery. The presence of a severe spinal injury was not initially evident, but it became apparent after the thoracotomy. Minor vertebral fractures are unlikely to cause a fatal hemothorax because the thoracic vertebral body is covered by a thick parietal pleura. 4 However, in severe vertebral fractures accompanied by dislocation, the edge of the fracture may directly damage the parietal pleura, allowing the hemorrhage to flow into the pleural space as the thoracotomy revealed. In Case 2, the spinal injury was diagnosed early as a chance-type fracture of L1; however, the delayed occurrence of the hemothorax resulted in an unstable patient condition. Since the bleeding source was unknown, angiography was prioritized after the patient’s vital signs had stabilized. Fortunately, the lumbar artery was identified as the bleeding source and a thoracotomy could be performed after temporary hemostasis was achieved. The lumbar arteries run in front of L1 to L4 behind the diaphragmatic crura.5,6 Even if these vessels collapse, bleeding will continue in the retrocrural space. In the case of a spinal injury involving a large vertebral dislocation, as described here, the crura may also collapse, resulting in hemorrhage into the subdiaphragmatic space and eventually leading to intrathoracic hemorrhage. A chance-type fracture traverses the vertebral body components and often occurs in cases of multiple trauma, such as after a severe traffic accident. 7 There have only been a few reports in which a hemothorax was caused solely by this etiology. We summarized the five cases of life-threatening hemothorax due solely to vertebral fractures that we found in the literature, similar to those described here, in Table 1.4,8–10 Fractures of the lower thoracic vertebrae occur more commonly in the elderly and are believed to be caused by decreased spinal flexibility and bone mineral density due to aging. The tissue surrounding the spine also tends to be fragile, further increasing the risk of fracture dislocation, which may result in hemorrhage. In both of our cases, movement appeared to be related to the occurrence of delayed intrathoracic bleeding. Case 1 appeared to involve delayed bleeding because the fracture dislocation was promoted at the movement during the CT examination. In contrast, in Case 2, we believe that the bleeding occurred while the patient assumed a seated position, such as during eating. Masteller et al. 10 reported that elderly people were likely to develop a hemothorax from thoracic vertebral fractures despite a lack of major injuries. Special attention should be given to these patients. In the thoracotomy, bone wax was useful for achieving hemostasis. However, it provided only primary hemostasis, and the dislocated vertebral fracture required emergency stabilization to prevent secondary bleeding. Thus, it is necessary to provide treatment at the appropriate time upon consideration of the state of intrathoracic bleeding.
Reported cases of traumatic hemothorax due solely to a vertebral fracture.

Conclusion
Here we reported two cases of traumatic hemothorax that were difficult to diagnose. In cases of no rib fracture and an unknown bleeding source, vertebral fracture should be considered a possible cause. Unstable chance-type fractures may lead to fatal hemothorax, even in the late phase; thus, particular attention is needed in elderly patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case series was obtained from Ethics Review Committee of Rakuwakai Otowa Hospital (approval number: 18-019).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.