
Abstract
Sarcoidosis is an idiopathic disease, characterized by non-caseating granulomas in multiple organs/tissues. Cutaneous involvement occurs in approximately one-quarter of patients with a wide variety of presenting morphologies. This case report describes a case of photodistributed sarcoidosis, a rare cutaneous variant, with systemic involvement. A 42-year-old man presented with a history of a pruritic, rash with photoexacerbated annular plaques along with arthralgias and bone pain. Compared to previous reports of photodistributed sarcoidosis, our case presented with annular plaques rather than papules, and there was no prior exposure to ionizing radiation. He was treated successfully with prednisone and hydroxychloroquine. It is important to include sarcoidosis in the differential of photodistributed dermatoses.
Introduction
Sarcoidosis is an idiopathic disease characterized by the presence of non-caseating granulomas in a variety of organs and tissues. The clinical presentation is heterogeneous as cutaneous lesions may present with a variety of morphologies, including papules, nodules, plaques, and infiltrated scars. 1 This includes many uncommon and rare morphologies (Table 1). Since it is a rare presentation, there are few reports of photosensitive cutaneous sarcoidosis in the literature.1–3
Uncommon and rare cutaneous variants of sarcoidosis.

Case report
A 42-year-old man, presented to the Dermatology clinic with a history of a pruritic rash that started on his upper chest and spread to his head in a photodistributed pattern. He also had severe bone pain, unexplained recurrent fevers, right upper quadrant pain, muscle aches, ankle joint pain, mild subjective exertional dyspnea and drenching night sweats that began 9–10 months after the onset of the rash. He reported that the eruption was exacerbated by sun exposure. Previous treatment included two, 2-week courses of 50 mg of prednisone. Partial improvement of the rash, occurred each time. Multiple courses of topical permethrin to treat suspected scabies did not help. Past medical history was remarkable only for alcohol-induced cirrhosis and psoriasis. His medications were venlafaxine, naproxen, and pantoprazole. He did not have any industrial chemical or radiation exposures, and his family history did not include any autoimmune diseases.
On presentation, he had photodistributed well-defined red-brown, annular and ovoid non-scaly plaques mainly involving the head, neck, shoulders, and upper chest (Figure 1(a)). There were also subtle well-defined, non-scaly red-brown macules on the abdomen and thighs. The tibia and ulna were tender to palpation bilaterally. There was no overt joint inflammation and no adventitial breath sounds. The differential diagnosis included granuloma annulare, subacute cutaneous lupus, infectious granulomas including leprosy, actinic granuloma, and mycosis fungoides.
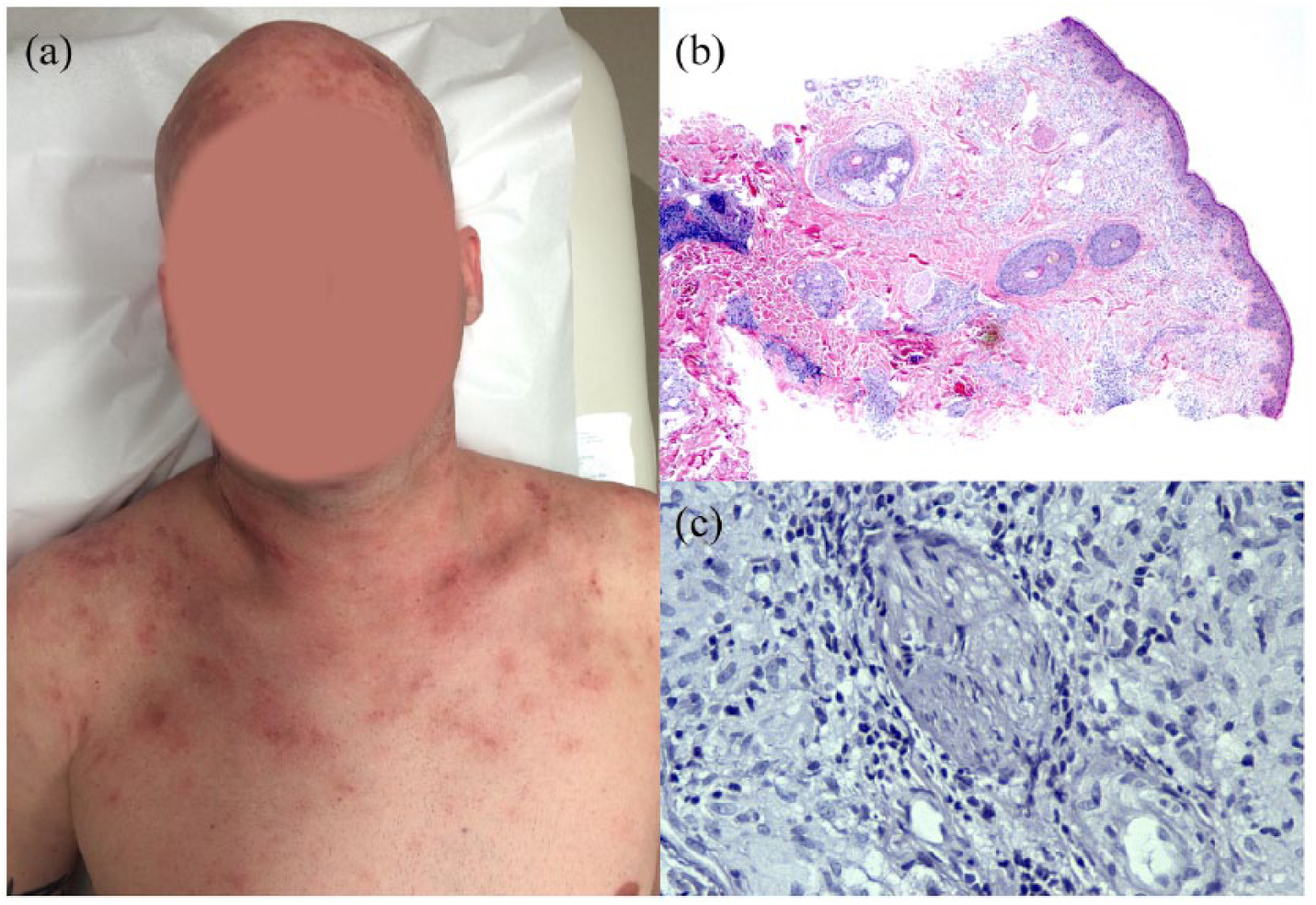
(a) Photodistributed red-brown non-scaly plaques in a photodistributed pattern on the head and neck. (b) A punch biopsy with H&E stain demonstrating sarcoidal granulomata within the superficial and deep dermis, and (c) showing no evidence of leprosy, tuberculosis or another mycobacterium within the granulomas on Fite stain. The photomicrographs are at taken at 40× and 200× magnification, respectively.
Notable laboratory findings included a negative antinuclear antibody test, diffuse reactive hypergammaglobulinemia with no monoclonal bands and mild transaminitis with elevated gamma-glutamyl transferase. It was felt his abnormal liver enzyme tests were most likely secondary to his alcohol use. Skin biopsy of the lesions revealed superficial and deep non-necrotizing granulomatous dermatitis with scattering accompanying lymphocytes. There were no atypical lymphocytes, diffuse neutrophilic/lymphocytic infiltrates, dermal edema, mucin, or epidermal change (Figure 1(b)). The skin biopsy (Figure 1(c)) and a blood smear were negative for leprosy. A tuberculosis skin test was non-reactive. On imaging, a computed tomography (CT) of his chest and abdomen showed non-calcified pulmonary granulomas, while a bone scan demonstrated cortical uptake in the tibia suggestive of osseous sarcoidosis. Further testing of pulmonary function excluded restrictive lung disease. An echocardiogram and ophthalmological exam were unremarkable.
In light of his investigations, he was diagnosed with systemic sarcoidosis with photodistributed cutaneous involvement. Prednisone 40 mg daily with a slow taper and hydroxychloroquine 200 mg twice daily were started. Resolution of his cutaneous involvement, arthralgias, and bone pain occurred over 3 months. He is followed by a general internist to monitor for progression of his pulmonary disease and his other systemic manifestations. He has not had any adverse side effects and has had a sustained remission on antimalarial monotherapy.
Discussion
Sarcoidosis is a systemic granulomatous disease with cutaneous manifestations occurring in approximately one-quarter of patients. There are various skin morphologies possible including the more common brown-purple infiltrated plaques or papulonodular lesions. 1 Although radiation exposure 4 has been theorized to cause photodistributed sarcoidosis, this has not been associated with any reported cases, including ours. Here, we have reported a case of photosensitive and photodistributed cutaneous sarcoidosis. In contrast to previous reports,1–3 our patient’s cutaneous eruption presented with annular plaques, not papules. Limitations of this case report include non-generalizability to a larger population as this case report included one patient.
Previous reported cases were treated successfully with either oral or topical steroids, with and without antimalarial medications.2,3 One patient was treated with photoprotection only due to intolerance to hydroxychloroquine. 1 Our patient’s sarcoidosis was successfully treated with hydroxychloroquine and oral prednisone; however, hydroxychloroquine caused a mild flare in his psoriasis despite concurrent oral prednisone. Therapeutic options are limited by his liver cirrhosis and social circumstances. He preferred to manage his psoriatic lesions with topical therapy only. Systemic corticosteroids and antimalarial agents have been the most effective therapies for photodistributed sarcoidosis 5 and can also treat systemic manifestations, including bone pain. For optimal treatment, patients require screening for pulmonary and extrapulmonary disease at diagnosis to ensure appropriate care. This case report highlights a rare case of photodistributed sarcoidosis and supports the use of prednisone and hydroxychloroquine in its management.
Footnotes
Acknowledgements
All authors had full access to all of the information in the report and take responsibility for its integrity and accuracy. B.W. and J.M. gave critical revision of the manuscript for important intellectual content. C.O., B.W., and I.T. drafted the manuscript.
Informed consent
The patient gave verbal consent but was unable to give written consent. Facial features have been obscured to maintain confidentiality.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.