
Abstract
Sarcoidosis is an inflammatory multisystemic disease of unknown etiology with multiple presentations of cutaneous lesions. It characteristically infiltrates scars due to several kind of trauma such as surgery, tattoo and even herpes zoster. We present a case of a 65-year-old woman with progressive distal paresthesia and motor weakness. She was referred to our dermatology clinic for a new violaceous nodular plaque within an old melanoma scar on the posterior neck. On positron emission tomography–computed tomography, there were multiple enlarged thoracic lymphadenopathy and a fluorodeoxyglucose-avid cutaneous lesion on the posterior neck, right in the melanoma scar. Cutaneous and nerve biopsies showed non-necrotising granulomas, supporting the diagnosis of systemic sarcoidosis and excluding melanoma recurrence with metastasis. It is the first case of cutaneous sarcoidosis arising within a melanoma scar. Interestingly, patients with melanoma have a higher risk of sarcoidosis.
Keywords
Introduction
Sarcoidosis is an inflammatory multisystem disease of unknown etiology characterised by the development of non-caseating granulomas in different organs. 1 It affects the skin in 25% to 35% of cases. 1 Cutaneous sarcoidosis is often referred to as the great imitator because of a myriad of possible skin lesions that can simulate other diseases. 2 Occasionally, it has the characteristic of infiltrating scars of surgery, trauma and tattoos. 1 Few cases of subcutaneous sarcoidosis in a melanoma scar have been reported to date. 3
Observation
A 65-year-old woman presented to her regional hospital with bilateral hand and foot paresthesia and distal motor weakness that started 3 months ago and progressively increased. She was transferred to a university hospital for extensive investigations. Her past medical history revealed a cutaneous melanoma of the left posterior neck in 2015 (Breslow 1.41 mm, 2 mitoses/mm2, no ulceration). Sentinel lymph node biopsy was negative (stage T2aN0M0). Re-excision occurred in July 2015 with 1.0-cm margins. She did not receive any systemic antineoplastic therapy and had been lost to follow-up. Her medical diagnoses included seronegative polyarthritis, high blood pressure, type II diabetes, dyslipidemia and anxiety. Her medications included etanercept, hydroxychloroquine, leflunomide, amlodipine, olmesartan, metformin, rosuvastatin, dexlansoprazole and citalopram.
She was evaluated by the dermatology team for a new lesion within the site of her melanoma scar. The lesion was asymptomatic and had not been noticed by the patient. The physical examination showed a violaceous nodular plaque of 1.5 cm per 0.5 cm located in the medial portion of her linear melanoma scar on the left posterior cervical region (Figure 1). There were no other cutaneous lesions, nor any palpable lymphadenopathy or hepatosplenomegaly.

Cutaneous violaceous nodular plaque in a melanoma scar on the left posterior neck.
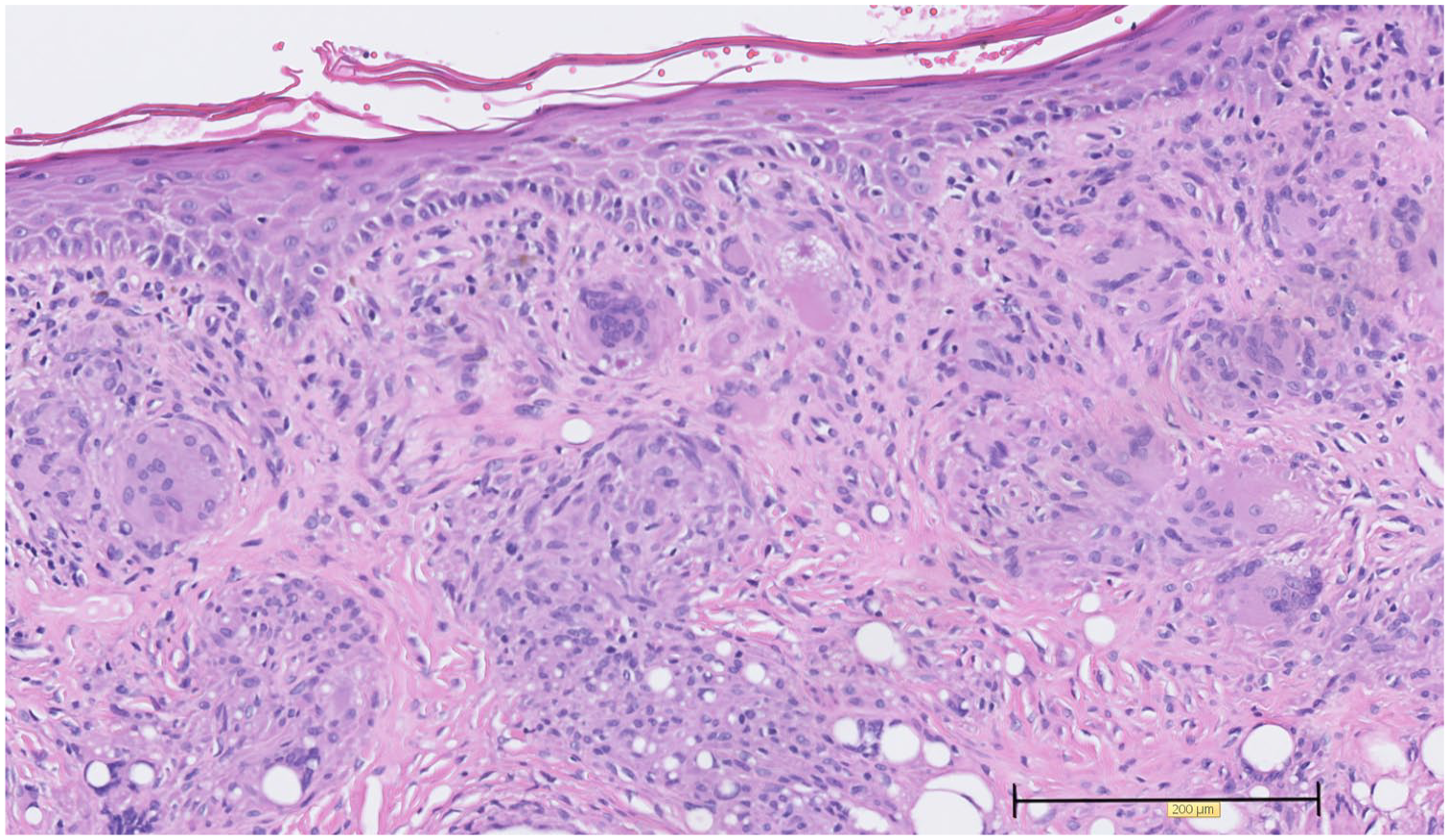
Concurrently, she was evaluated in the neurology department with sensitive and motor nerve conduction studies that showed mononeuritis multiplex. Thoracic, abdominal and pelvic computed tomography with contrast showed multiple enlarged thoracic lymphadenopathy without any sign of other neoplasia. Positron emission tomography–computed tomography (PET/CT) illustrated hilar and mediastinal lymphadenopathy and a focal cutaneous captation of 1 cm per 0.7 cm in the posterior left cervical area. Fine-needle aspiration of a right paratracheal adenopathy guided by endobronchial ultrasound was done and only provided cells with normal morphology. Adenopathy were too small to try a mediastinoscopy to provide other tissue for analysis. Bronchoscopy analysis (cytology and cultures) was normal. She then underwent a sural nerve biopsy that showed non-necrotising granulomatous inflammation around the nerve compatible with sarcoidosis. A muscle biopsy was completely normal. In the dermatology department, we proceeded to an incisional 4-mm punch biopsy of the nodular plaque of the neck. Histologic examination showed multiple non-necrotising granulomas in the cicatricial superficial and mid dermis (Figures 2 and 3). A few asteroid bodies were present in the granulomas (Figure 4). Polarised microscopy showed rare irregular-shaped birefringent particles. Special stains for microorganisms were negative in the biopsy sample. It confirmed the diagnosis of cutaneous sarcoidosis in the patient with a new diagnosis of systemic sarcoidosis with polyadenopathy and mononeuritis multiplex.

Skin biopsy shows non-necrotising granulomas in a cicatricial superficial and mid dermis on hematoxylin and eosin stain.
High-power view of non-necrotising granulomas on hematoxylin and eosin stain.
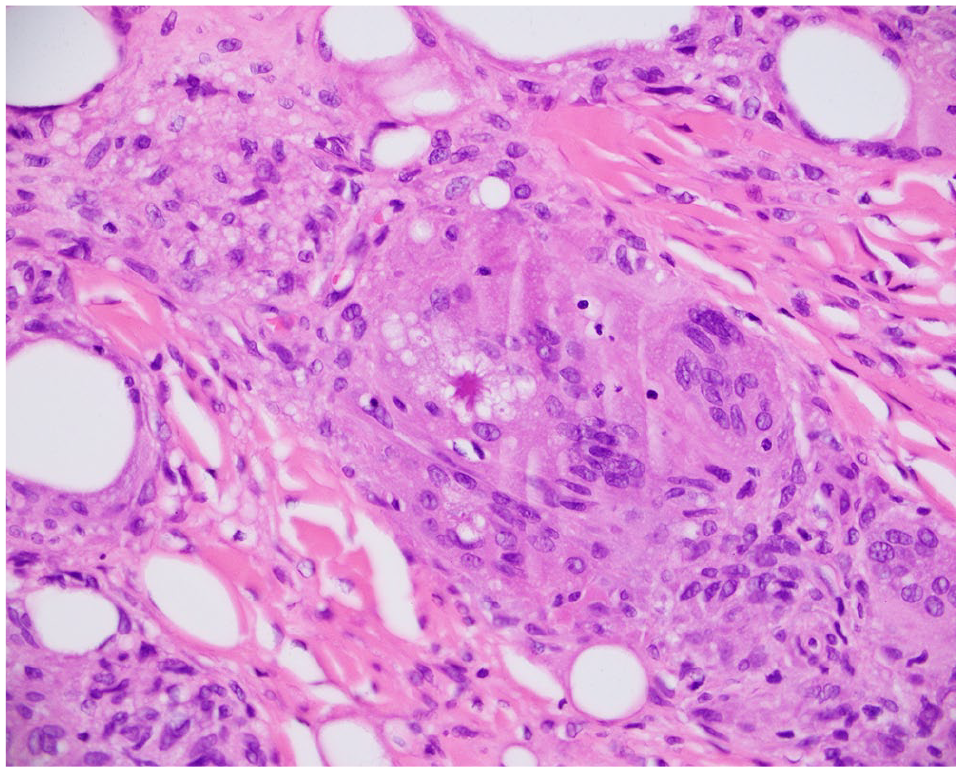
High-power view of an asteroid body on hematoxylin and eosin stain.
Cerebral magnetic resonance imaging did not show any signs of central nervous system involvement by sarcoidosis. A serum angiotensin-converting enzyme level of 56 U/L was normal (normal: 10–74 U/L).
She was treated initially with a 2-day course of intravenous immunoglobulins without any success. She then received a 5-day course of high-dose Solu-Medrol followed by prednisone in tapering doses from 60 mg per day to 15 mg per day at 5 months of follow-up. Leflunomide was stopped by her rheumatologist because of a possibility of inducing neurologic symptoms. Etanercept was continued until follow-up when it was replaced by infliximab in an attempt to treat polyarthritis and sarcoidosis at the same time. On follow-up at 4 months, she showed significant improvement with normalisation of walking and decreased distal paresthesia. Motor and sensitive nerve conduction studies significantly improved. The nodular plaque on the posterior neck had also decreased in size.
Discussion
Sarcoidosis is an inflammatory multisystemic disease that affects both sexes, but predominates in women, and can present at all ages and in any ethnic groups. 1 It is characterised by the development of non-caseating granulomas in different organs such as lungs, lymph nodes and nervous system. 1 Fatigue, fever and night sweats are frequent systemic symptoms. 1 In 25% to 35% of cases, it affects the skin in different manners. 1 Macules, papules, plaques and subcutaneous nodules are a few of all possible lesions which show granulomas in histopathology. 1 Rarely, sarcoidosis infiltrates cutaneous scars of surgery, trauma, tattoos, intramuscular or intradermal infiltrations and herpes zoster,1,4 but this rare sign is highly specific of a cutaneous manifestation of sarcoidosis. 5
Malignancies appear to be associated with sarcoidosis.6,7 Neoplasia can appear before, concomitantly or after the diagnosis of sarcoidosis. Patients with sarcoidosis seem to have an increased risk of melanoma. 7 More importantly, among melanoma patients, an increased risk of sarcoidosis has been described. 6 In a review of 1199 inpatients with melanoma, 7 developed sarcoidosis, which shows a prevalence of sarcoidosis of 0.58% among melanoma inpatients. 8 In a recent review of the literature, sarcoidosis has been reported in 80 patients with melanoma, with the majority of sarcoidosis diagnosed after the neoplasia. 6 Adjuvant therapy for melanoma with interferon or immunotherapy is a significant risk factor for the development of sarcoidosis, but approximately half of the reported cases were not associated with antineoplastic treatment.6,8 Knowing the possible relation between melanoma and sarcoidosis, fluorodeoxyglucose (FDG)-avid cutaneous scar and nodal involvement on PET/CT can be a diagnostic pitfall because it can correspond not only to melanoma recurrence with metastasis, but also to sarcoidosis. 9 Cutaneous and lymph node biopsies are then important to distinguish melanoma recurrence with metastasis from sarcoidosis as melanoma metastasis can also coexist with lymph node sarcoidosis. 10
Sarcoidosis treatment is necessary if an organ function is threatened and includes systemic corticosteroids such as prednisone. 1 Treatment with anti-tumour necrosis factor (anti-TNF), mostly with infliximab, has proven effective for multisystemic sarcoidosis. 11
Footnotes
Acknowledgements
The authors thank Dr. Steve Mathieu for providing language help.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent for patient information and images to be published was provided by the patient.