
Abstract
Granulomatous interstitial nephritis is a rare finding in renal biopsy caused by drugs, infections, and inflammatory or autoimmune diseases. Idiopathic cases account for 18% of granulomatous interstitial nephritis in native kidneys. Sarcoidosis and drugs are the most common causes of granulomatous interstitial nephritis in Western countries, while in India tuberculosis prevails. Few cases of renal sarcoidosis without extrarenal involvement, that is, isolated renal sarcoidosis, have been reported. The diagnostic criteria of isolated renal sarcoidosis remain, however, unclear. Extrarenal sarcoidosis and other etiologies of granulomatous interstitial nephritis, in particular drug-related, have to be excluded. Some of these patients may develop extrarenal manifestations during follow-up. Changes in calcium and vitamin D metabolism are frequently observed in renal sarcoidosis and support its diagnosis. While non-necrotizing granulomas are a feature of sarcoidosis and drug-induced granulomatous interstitial nephritis, they also prevail in tuberculosis-associated granulomatous interstitial nephritis. Granulomatous interstitial nephritis caused by sarcoidosis and drugs usually responds to steroid therapy. A poor response to steroids may indicate an infectious etiology such as tuberculosis and should lead to a review of the initial diagnosis. This article gives an overview of the various etiologies of granulomatous interstitial nephritis, their frequency and histopathological characteristics, as well as potential biomarkers associated with renal sarcoidosis.
Introduction
While interstitial nephritis is a common cause of renal failure, granulomatous interstitial nephritis (GIN) is a rare histological finding. It is observed in up to 0.9% of native kidney biopsies 1 and about 6% of biopsies with interstitial nephritis. 2 Renal granulomatoses can have a variety of causes. These include drugs, infections, and autoimmune or inflammatory diseases, such as sarcoidosis.1–8 Sometimes a definite etiology cannot be identified (idiopathic) or only becomes evident later during follow-up. Granulomatous inflammation may occur isolated in the kidney or may be associated with extrarenal disease manifestations—while identification of the underlying etiology is facilitated in the latter case.
In 30% to 79% of native kidney biopsies from patients with sarcoidosis, GIN is observed, consistent with renal sarcoidosis.9–12 Other renal manifestations of sarcoidosis are nephrolithiasis and nephrocalcinosis due to disturbances in calcium metabolism. Moreover, non-granulomatous interstitial nephritis and less common glomerular diseases are observed. 13 Occasionally, renal sarcoidosis without extrarenal manifestations, that is, isolated renal sarcoidosis, has been reported that may be associated with hypercalcemia and/or elevated serum angiotensin-converting enzyme (ACE).4,14 Its diagnostic criteria are, however, not well established and based upon exclusion of other causes. It has been suggested that at least a fraction of cases with idiopathic GIN represent isolated renal sarcoidosis.4,14
Response to treatment in GIN is variable and depends upon the underlying etiology and stage of the disease. Corticosteroids are the cornerstone of treatment in renal sarcoidosis, tubulointerstitial nephritis with uveitis (TINU), and drug-induced GIN. 4 In patients with GIN due to sarcoidosis who develop steroid toxicity or do not respond to steroids, other immunosuppressive drugs such as azathioprine, mycophenolate mofetil, or tumor necrosis factor alpha (TNFα) inhibitors are used. 15 Among GIN caused by infections, mycobacterial infection is the most common cause, requiring anti-tubercular treatment. 8
This review aims to give an overview of the different etiologies of GIN, their frequencies, and histopathological characteristics, focusing on idiopathic GIN and isolated renal sarcoidosis.
Methods
This review is based on PubMed and Google Scholar databases. Our search used the following keywords and/or their combinations: renal sarcoidosis, GIN, idiopathic, isolated, renal-limited sarcoidosis, renal confined sarcoidosis, and biomarker. Articles were selected according to the title and the abstract. The reference lists of the selected articles were also scanned for titles relevant to the review.
Causes and frequency of GIN
GIN is a rare histologic finding observed in 0.5% to 0.9% of native1,6 and 0.3% to 1% of transplant kidney biopsies.3,16 Causes of GIN in native kidneys are infections, drugs, and inflammatory or autoimmune diseases, in particular sarcoidosis and granulomatosis with polyangiitis (GPA), while infectious causes dominate in transplant kidneys3,17 (for an overview, see Table 1). If no cause can be identified, idiopathic GIN is diagnosed. In retrospective studies, 18% of GIN in native kidney biopsies account for idiopathic GIN1,2,4–8 (Table 2). However, the underlying causes of GIN vary according to the geographical area. In Europe and the United States, sarcoidosis and drug-induced and idiopathic GIN prevail, while tuberculosis is the most common diagnosis in India 8 (Table 2). In addition, ethnicity and socioeconomic factors may be risk factors of GIN associated with infections, in particular tuberculosis. 7
Causes of GIN and pathology.

GIN: granulomatous interstitial nephritis; NSAID: non-steroidal anti-inflammatory drug; TNFα: tumor necrosis factor alpha; EBV: Epstein–Barr virus; TINU: tubulointerstitial nephritis with uveitis; GPA: granulomatosis with polyangiitis; EGPA: eosinophilic granulomatosis with polyangiitis; BCG: Bacillus Calmette–Guerin.
Non-necrotizing granulomas prevail in tuberculosis-induced GIN.
Causes of GIN: frequencies according to the literature (%).
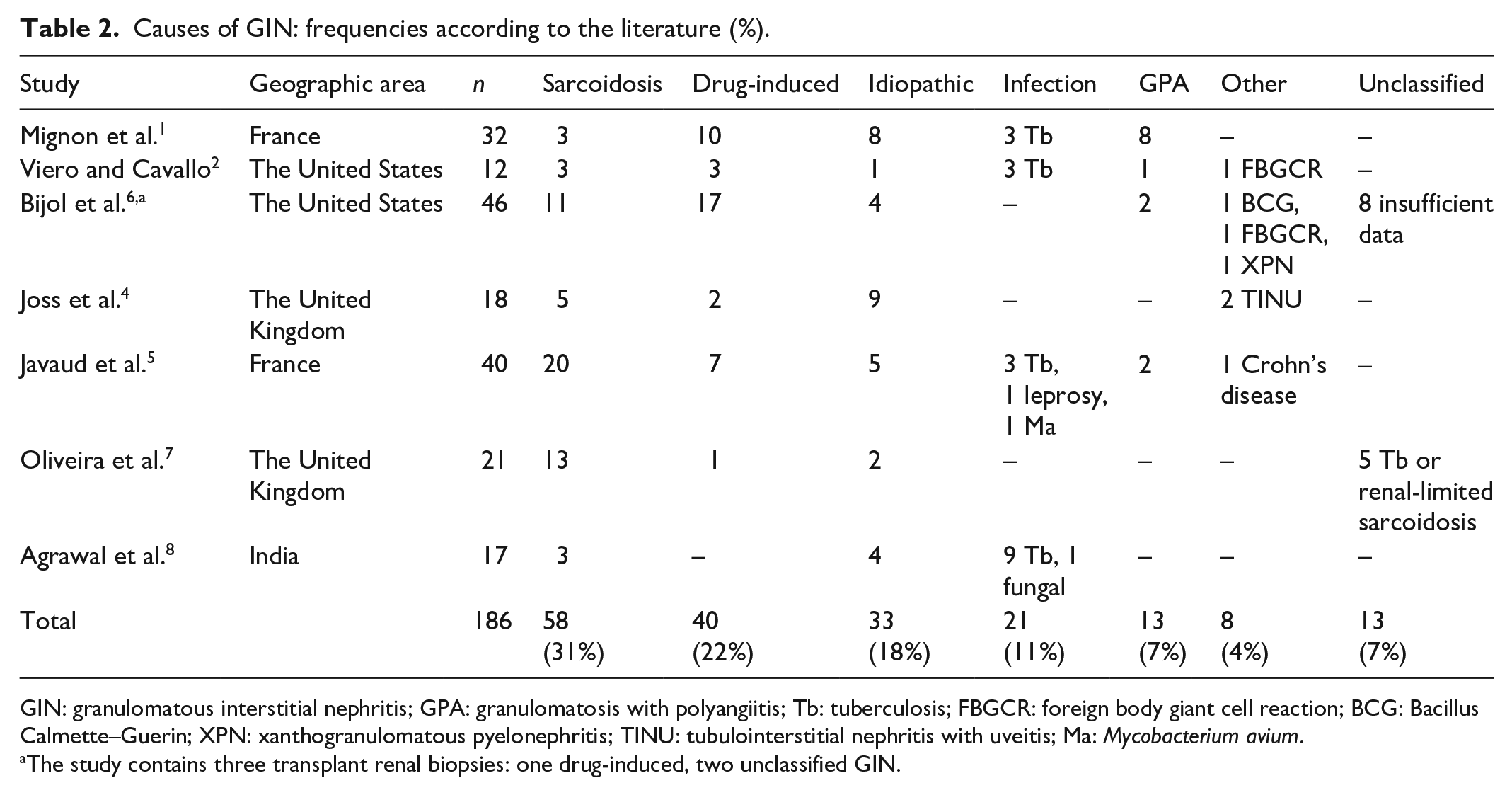
GIN: granulomatous interstitial nephritis; GPA: granulomatosis with polyangiitis; Tb: tuberculosis; FBGCR: foreign body giant cell reaction; BCG: Bacillus Calmette–Guerin; XPN: xanthogranulomatous pyelonephritis; TINU: tubulointerstitial nephritis with uveitis; Ma: Mycobacterium avium.
The study contains three transplant renal biopsies: one drug-induced, two unclassified GIN.
Histopathology: necrotizing versus non-necrotizing GIN
GIN is commonly characterized by an interstitial inflammatory infiltrate that includes distinct granulomas composed of aggregates of epithelioid histiocytes with a peripheral cuff of lymphocytes and plasma cells.3,17 Moreover, multinucleated giant cells derived from merged epithelioid cells may occur (Figure 1).

Granulomatous interstitial nephritis with non-necrotizing epithelioid cell granulomas (*), multinucleated giant cells (→), and interstitial inflammatory cell infiltration. PAS stain ×100.
Granulomas are further characterized as necrotizing if they have a necrotic center or non-necrotizing. Non-necrotizing granulomas are, in particular, observed in sarcoidosis and drug-induced GIN, while necrotizing granulomas are found in GPA and tuberculosis-induced or fungal GIN (see Table 1 and Figure 2). In drug-induced GIN, granulomas are often poorly formed, that is, ill-defined, while in sarcoidosis well-formed granulomas are frequently seen. 3 This distinction is, however, not always fully developed and therefore not reliable. 6 Interstitial infiltration of eosinophils (Figure 3) is also regarded as typical for drug-induced GIN but can also be seen in GIN cases of other etiology.5,6

Ill-defined epithelioid cell granuloma with central necrosis (*). HE stain ×200.

Ill-defined epithelioid cell granuloma with eosinophilic interstitial cell infiltration. HE stain ×200.
Recently, there has been evidence that renal tuberculosis, apart from the classical form with gross tissue destruction and caseating granulomas, can also present as chronic GIN that may not be caused by direct bacterial invasion. 18 In these cases, mycobacterium tuberculosis is frequently not detected in renal tissue by staining or polymerase chain reaction (PCR), and necrotizing granulomas are only found in a minority of patients. 19 These patients have an inferior prognosis compared to patients with GIN due to sarcoidosis, possibly due to delayed diagnosis, and show a poor response to steroid therapy. 7 While necrotizing granulomas are occasionally seen in GIN associated with tuberculosis, they are not a feature of renal sarcoidosis and idiopathic GIN. 8
Interstitial calcium deposition is observed in 16% to 29% of renal sarcoidosis patients9–11 and may therefore point to renal sarcoidosis. However, renal calcifications have also been described in drug-induced and idiopathic GIN. 4
Differential diagnosis of isolated renal sarcoidosis
In sarcoidosis, renal involvement is uncommon, occurring in 0.7% to 4.3% of patients,20–22 who usually also have extrarenal disease manifestations at presentation. 13 Renal disease in sarcoidosis, however, may be underestimated. Up to 25% to 30% of sarcoidosis patients may have clinically unapparent renal involvement. 23 Sarcoidosis accounts for 31% of GIN in native kidney biopsies, being the most frequent cause of GIN1,2,4–8 (Table 2). Some cases of idiopathic GIN may represent a renal-limited form of sarcoidosis, that is, isolated renal sarcoidosis, or precede extrarenal manifestations of sarcoidosis. 4 Furthermore, sarcoidosis may relapse isolated in the kidney after treatment of initial presentation with multiple organ involvement. 24 However, careful review of reported cases of isolated renal sarcoidosis reveals a history of drug intake associated with GIN, such as non-steroidal anti-inflammatory drug (NSAID), 25 or extrarenal disease manifestations, such as mediastinal and hilar lymphadenopathy 26 or joint involvement, 27 in some. In these cases, the diagnosis of isolated renal sarcoidosis may be doubted. In other reported cases of isolated renal sarcoidosis, concomitant diseases that may affect kidney function and calcium metabolism, for example, monoclonal gammopathy, were present. 28 Oliveira et al. reported a group of patients initially diagnosed with renal-limited sarcoidosis and treated with steroids who were then diagnosed with tuberculosis during follow-up 7 (Table 2). Therefore, to diagnose isolated renal sarcoidosis, extrarenal sarcoidosis, infections or other diseases that may have contributed to pathogenesis and an obvious drug-related etiology should be ruled out. 14
Potential biomarkers of renal sarcoidosis
Biomarkers are used to detect the presence and severity of an inflammatory disease. In sarcoidosis, a variety of potential biomarkers have been investigated in serum, bronchoalveolar lavage, and imaging. 29 An ideal biomarker for sarcoidosis has not been discovered yet. Hypercalcemia, hypercalciuria, changes in vitamin D metabolism, increased ACE, or soluble interleukin-2 receptor (sIL-2R) levels, although inconclusive, may be associated with renal sarcoidosis and support its diagnosis (Table 3).
Potential biomarkers of renal sarcoidosis.

n.i.: not investigated in renal sarcoidosis; 25OH-vitamin D3: 25-hydroxy-vitamin D3; ACE: angiotensin-converting enzyme; sIL-2R: soluble interleukin-2 receptor.
The mechanisms of abnormal calcium and vitamin D metabolism in sarcoidosis are probably multifactorial. They include an increased conversion of 25-hydroxy-vitamin D3 to 1,25-dihydroxy-vitamin D3 by 1α-hyxdroxylase produced by activated macrophages in granulomas, 30 parathormone-related protein, 31 as well as cytokine and growth factor production in sarcoid granulomas.32,33 Hypercalcemia is observed in 24% to 42% of patients with renal sarcoidosis9–11,34,35 (Table 3), while it is only observed in 4% of patients with sarcoidosis without renal involvement. 36 Hypercalcemia correlates inversely with response to therapy and resolves in remission with renal function improvement.10,13 Zammouri et al. reported hypercalciuria in 50% and Mahfoudi et al. in even 83% of their renal sarcoidosis patients at presentation.34,35 Increased urinary calcium excretion is observed early and may precede hypercalcemia in sarcoidosis with renal involvement. However, urine calcium is rarely measured in routine diagnostics and data are therefore often not available in retrospective analysis. Data on Vitamin D levels in renal sarcoidosis are scarce. Mahevas et al. observed decreased 25-hydroxy-vitamin D3 levels in seven out of nine patients and Naderi et al. in five out of five patients at presentation,10,13 while 1,25-dihydroxy-vitamin D3 levels were normal in the majority of patients. 13
Serum ACE is probably the most common laboratory test for sarcoidosis, and overall 30% to 80% of sarcoidosis patients have increased ACE levels. 37 ACE is secreted by macrophages and epithelioid cells, and correlates with granuloma burden. ACE levels have been found to be increased in several other inflammatory diseases, including tuberculosis, resulting in a low sensitivity. 38
In renal sarcoidosis, elevated serum ACE levels were seen in 18%, 55%, and 67% of patients at presentation.9,10,34,35 Oliveira et al. reported a distinct decrease in ACE levels in renal sarcoidosis patients with extrarenal involvement after 1 year of immunosuppressive treatment. 7 However, in patients on ACE inhibitors, serum ACE levels have to be interpreted carefully and cannot be used in diagnosis or as markers of disease activity. 39
sIL-2R, the circulating form of the interleukin-2 receptor (IL-2R), is a serum marker frequently used to assess activity and prognosis of pulmonary sarcoidosis.40,41 Activated T-cells upregulate the expression of the IL-2R on their surface and release the sIL-2R into circulation. 42 Consequently, elevated sIL-2R levels correlate with the activity of T-cell-mediated diseases and are not specific to sarcoidosis. They are found in various autoimmune diseases and hematological malignancies. 43
In renal sarcoidosis, clearly increased sIL-2R levels have been reported at disease presentation. 13 However, larger studies and data on the course of sIL-2R levels in renal sarcoidosis are lacking. Moreover, sIL-2R levels increase with renal function impairment due to a reduced clearance which may make data difficult to interpret. 44 Other potential biomarkers have not yet been explored in renal sarcoidosis. 29
Isolated renal sarcoidosis in retrospective studies and response to treatment
The classification of a GIN as isolated renal sarcoidosis should be made carefully in retrospective analyses, in particular because data and information may be incomplete. In some retrospective studies on renal sarcoidosis, GIN without extrarenal sarcoidosis was excluded from the analysis to avoid misclassification of GIN due to drugs, infections, and autoimmune diseases.10,13 Other studies on renal sarcoidosis have only included patients with at least one other localization of the disease,9,34 or evaluated renal sarcoidosis in patients with diagnosis of systemic sarcoidosis.11,35
In their study on GIN, Joss et al. included two patients in the sarcoidosis group with no extrarenal manifestations. 4 Both had raised serum ACE, one also hypercalcemia, and both responded to steroid treatment. Oliveira et al. reported five patients with isolated renal sarcoidosis. Four patients responded to steroids, including one patient with raised serum ACE and hypercalcemia. In contrast, five patients in that study were initially diagnosed with isolated renal sarcoidosis, but those treated with steroids showed poor response to therapy. These patients were later diagnosed with tuberculosis 7 (Table 2). In none of them, elevated serum ACE or hypercalcemia was reported. Other studies on GIN did not report cases of isolated renal sarcoidosis.1,2,5,6,8
In a study with seven patients with isolated renal sarcoidosis, two patients had raised serum ACE and hypercalcemia and one patient raised serum ACE only. Five patients, including the patients with raised serum ACE, responded to steroid therapy. 14 Another report described five patients with isolated renal sarcoidosis. Only one patient had elevated serum ACE, and four patients showed renal function improvement after steroid therapy. 45
Treatment with steroids is the standard of care in sarcoidosis, TINU, and drug-induced GIN. In idiopathic GIN, steroids have also been used, sometimes with consecutive renal function improvement.4,7,8 However, some patients initially diagnosed with idiopathic GIN or isolated renal sarcoidosis may have underlying tuberculosis. In particular those with poor response to steroid therapy or risk factors of infection.4,7 In these cases, the initial diagnosis needs to be carefully reviewed.
Limitations
The current review has several limitations. First of all, there are only retrospective studies on GIN and renal sarcoidosis available. The number of studies on GIN is small, comprising only 12 to 46 patients each. Moreover, the studies have been published over a period of 33 years (1984–2017) during which drug use, infectious diseases, and their treatment have changed. This may affect the incidence and course of GIN caused by drugs and infections in the investigated populations. Finally, studies of GIN are predominantly from Western Europe and North America. In other geographic areas, the incidences of the various etiologies of GIN differ as indicated by the increased number of tuberculosis-induced GIN in India.
Conclusion
In summary, idiopathic GIN and isolated renal sarcoidosis are diagnosed by exclusion of other etiologies. A subset of patients with (idiopathic) GIN may have isolated renal sarcoidosis, in particular those with changes in calcium and vitamin D metabolism and/or raised serum ACE. These patients can develop extrarenal manifestations during follow-up and usually respond to steroid therapy.
Footnotes
Acknowledgements
We thank Athina Vassiliadou for her assistance in language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.