
Abstract
Dysplasia epiphysealis hemimelica, also known as Trevor Fairbank disease, is characterized by asymmetrical osteochondral overgrowth of the epiphyseal cartilage. The clinical presentation of dysplasia epiphysealis hemimelica is wide and variable, depending on the site of the lesion. Herein, we describe the physical examination of a 9-year-old boy with intra-articular dysplasia epiphysealis hemimelica, in whom the symptoms were elicited on “reverse Wilson’s sign”: bending the knee from 70° to 120° against resistance while externally rotating the tibia. Arthroscopic treatment of the intra-articular dysplasia epiphysealis hemimelica of the knee showed good outcome; hence, this modality should be considered for the management of intra-articular dysplasia epiphysealis hemimelica.
Introduction
Dysplasia epiphysealis hemimelica (DEH), also known as Trevor Fairbank disease, is characterized by asymmetrical osteochondral overgrowth of the epiphyseal cartilage.1,2 The clinical presentation of DEH is wide and variable, depending on the location of the lesion, and varies from asymptomatic to mechanical symptoms such as restricted joint movement and skeletal deformity. 3
Herein, we report a case of symptomatic knee joint caused by intra-articular DEH lesions, located at the posteromedial side of the medial femoral condyle (MFC). Symptoms were elicited on “reverse Wilson’s sign”: bending the knee while externally rotating the tibia. 4 The aim of this report was to describe the clinical symptoms and the physical examination of a boy with DEH and to show that arthroscopic treatment was successful for an intra-articular DEH lesion of the knee.
Case presentation
A 9-year-old boy presented to our institution with pain and catching phenomenon over the medial aspect of the right knee of 12 months duration without any past history of injury.
Physical examination revealed no effusion in the affected knee joint. Ligamentous instability tests were negative. Moderate tenderness and swelling were found over the posterior medial joint space. The range of motion was not restricted with neutral or internal rotation of the tibia; however, bending the knee while externally rotating the tibia caused pain, catching, and locking.
A plain radiograph revealed irregular exophytic ossification at the posteromedial side of the MFC (Figure 1). Computed tomography (CT) also revealed lobulated irregular osseous hypertrophy of the medial side of the femoral epiphyses (Figure 2). Magnetic resonance imaging (MRI) showed asymmetrical osteocartilaginous lesion, continuous with the distal femoral epiphysis (Figure 3). The cartilaginous region of the lesion showed intermediate signal intensity on proton-density weighted imaging (WI) (Figure 3(b)) and high signal intensity on T2*-WI (Figure 3(a) and (c)). The articular surface was swollen, and a cartilaginous bulge was found. These radiological findings were consistent with DEH. Knee pain, catching, and locking were continuous, and surgical treatment was finally selected.

Plain radiograph showing irregular exophytic ossification at the posteromedial side of the medial femoral condyle of the right knee.

Computed tomography (CT) images revealed lobulated irregular osseous hypertrophy of the medial side of the medial femoral epiphyses: coronal (a), sagittal (b), axial (c), and volume rendering imaging (d).

Magnetic resonance imaging showing asymmetrical osteocartilaginous lesions, continuous with the distal femoral epiphyses: coronal view of T2*-weighted image (WI) (a), sagittal view of fat suppression proton-density WI (b), and T2*-WI (c), and axial view of T2 turbo spin echo WI (d).
Examination under anesthesia revealed that locking and catching were reproducible by bending the knee from 70° to 120° against resistance while externally rotating the tibia.
Arthroscopy showed intact anterior cruciate ligament, posterior cruciate ligament, and meniscus. The chondral surface was intact and smooth, including the lateral compartment and patellofemoral joint. No free bodies were detected. The cartilaginous surface of the MFC was smooth without chondral injury or instability, but at the posterior part of the MFC, protuberance of the cartilaginous surface was seen without obvious injury, including fissures and defects (Figure 4(a)). The anterior part of the extensive chondral protuberance of the MFC impinged on the posterior medial tibia and menisci at about 70° of knee flexion while externally rotating the tibia (Figure 4(b)). The lesion rode over the posterior horn of the medial menisci on bending the knee (Figure 4(c)). Probing showed no softening or continuity differences between the lesion and the normal cartilage.
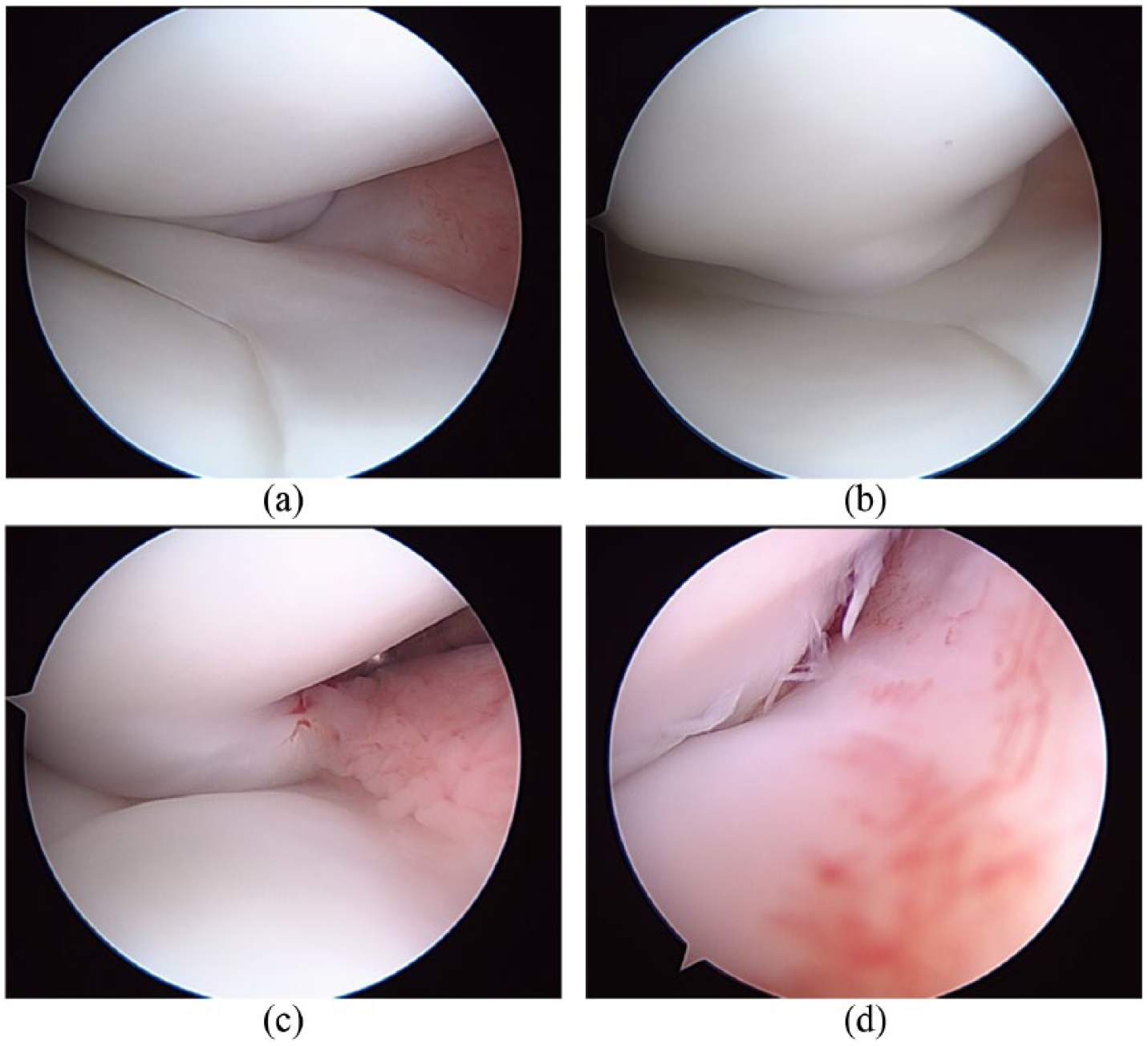
Arthroscopic findings: (a) protuberance of the cartilage surface was seen at the posterior medial femoral condyle (MFC) without cartilage injury. (b) The extensive chondral protuberance of the MFC was over-riding the posterior horn of the medial menisci during deep knee flexion. (c) The protruding region was impinging on the posterior medial tibia during internal rotation of the knee, and the locking phenomenon was elicited. (d) After arthroscopic removal and contouring of the posteromedial protuberance, impinging was eliminated during full range of motion.
Arthroscopic removal and contouring of the protuberance were performed until the phenomena were completely eliminated during the full range of motion (Figure 4(d)). After completing the procedure, the full range of motion while externally rotating the tibia was confirmed to be free of any locking or catching phenomena.
Postoperatively, active movement was encouraged, and progressive weight bearing was allowed. Three months postoperatively, he recovered completely and returned to school, with no recurrence of symptoms. He returned to his previous level of activity without any restriction 1 year postoperatively.
Discussion
DEH is a rare developmental disorder characterized by asymmetrical epiphyseal osteochondral overgrowth. 3 The etiology remains unclear, but it may be caused by a congenital defect affecting the early stages of limb development during the fetal life or by abnormal proliferation of chondrocytes. 5 DEH is also considered to be a non-hereditary disorder, and malignant transformation has not been reported. DEH most typically affects the tarsal or knee joint, although involvement of other bones such as the pelvis, carpus, and phalanges has also been reported. 6 The hemimelic and unilateral compartments are usually involved.
The clinical presentation of DEH is wide and variable, depending on the location of the lesion, and ranges from asymptomatic to mechanical symptoms, restricted joint movement, and skeletal deformity. 3
Intra-articular lesion of the knee, such as osteochondritis dissecans (OCD), also manifests with mechanical symptoms. The “classical site” of OCD lesions is the lateral aspect of the MFC.4,7 Physical examination of the classical site of medial femoral OCD showed “Wilson’s sign”, during which the examiner extends the knee from 90° to 30° against resistance while internally rotating the tibia.4,7 This sign is diagnostic of medial femoral OCD, causing pain due to lesion impingement on the tibial eminence.
Herein, we reported a case of symptomatic knee joint caused by intra-articular DEH lesions, located at the posteromedial side of the MFC. Symptoms could be elicited by bending the knee while externally rotating the tibia. Arthroscopy revealed extensive chondral protuberance at the posteromedial side of the MFC impinging on the posterior medial tibia and menisci at about 70° of knee flexion while externally rotating the tibia.
The natural course of DEH is progressive until skeletal maturity with associated physeal closure. 8 The management of DEH is controversial due to its rarity, and treatment options range from simple observation to radical excision of the lesions. 9 Asymptomatic lesions might be observed, with good outcomes. 10 Intra-articular lesions, however, tend to be complicated, with recurrence and deformities. 11
In this case, arthroscopic resection of the protuberance was performed, resulting in relief of symptoms. The role of arthroscopic treatment seems to be growing in the literature. In the ankle joint, a DEH lesion mimics anterior ankle spur, resulting in anterior ankle impingement syndrome. 12 Arthroscopic excision of the anterior tibial protuberance leads to an early good result with resolution of pain and limitation of motion. In addition, the results of the arthroscopic resection of intra-articular DEH in patients aged 9 and 10 years show good results up to 5 years of follow-up. 13 In this case, the good result of the patient may be also due to the lesion clear borders between normal and pathologic tissue, and small size. The arthroscopic approach should be considered as a treatment for patient with intra-articular DEH.
In conclusion, we reported the case of a patient with symptomatic knee joint caused by intra-articular DEH lesions, located at the posteromedial side of the MFC. Symptoms were elicited by bending the knee while externally rotating the tibia. Arthroscopic treatment successfully relieved the symptoms, and hence, should be considered as a treatment modality in patients with intra-articular DEH.
Footnotes
Acknowledgements
T.M. drafted the manuscript and A.H. reviewed the manuscript. The authors thank Nobuyuki Takahashi, MD, PhD, senior radiologist, for his contribution to image diagnosis and his valuable comments.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representatives for anonymized patient information to be published in this article.