
Abstract
Objectives:
Tenosynovial chondromatosis is an uncommon type of chondro-dysplasia of synovial and connective tissue. We report a case of a patient with a primary right wrist extra-articular chondromatosis extending to the flexor and the extensor compartments.
Methods:
Until now, there has been no study describing double surgical access for such a case.
Results:
Due to the extension, two surgical accesses are required to completely remove the neoformation.
Conclusions:
At 2 years of follow-up, the good functional-clinical results and absence of recurrence confirm the validity of our surgical strategy.
Introduction
Tenosynovial chondromatosis is a very rare benign disease that begins with chondro-dysplasia of synovial and connective tissues. 1 It is possible to define a primary form, of unknown etiology, and a secondary form linked to joint diseases such as osteoarthritis, osteochondral fractures and neuropathic arthropathy. As regards joint localization, we are able to identify an intra-articular form, which is the most common (incidence of 1:100,000)2,3 and an extra-articular form.2,4–6
The intra-articular form develops inside the joint, in particular from under the synovial tissue. It has a strong tendency to occur in the knee (50% of cases) and less frequently in the hip, shoulder and elbow.2,3,7 The extra-articular form develops from tendon sheaths or articular membranes and it affects mainly the hand and wrist structures.5,8,9
We report a case of patient, a 68-year-old man, who developed a primary right wrist extra-articular chondromatosis extending to the flexor and extensor compartments without functional joint deficit. The wide extension of the neoformation required two surgical accesses, one dorsal and the other volar, in order to remove it completely.
Case
A 68-year-old man was admitted to our hospital in March 2012 complaining of a big mass which he reported had begun to grow 2 years previously. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
This neoformation was developing progressively on both the dorsal and the volar sides of the right wrist. The subject did not report spontaneous pain, and there was no history of trauma. At physical examination, we highlighted the alteration of the anatomical profile of the right wrist which was swollen and showed no signs of cutaneous suffering. On palpation, the tumor revealed a tense-elastic consistency and the patient complained of pain during this examination. The active and passive range of motions of the wrist were possible up to the maximum degrees without any pain. We did not detect any neurovascular deficit.
The blood test excluded rheumatoid and infectious diseases. On the basis of these clinical elements, we performed ultrasound and magnetic resonance imaging (MRI) examinations. Both examinations showed an important synovial reaction with a pseudo cyst of about 43 mm in diameter involving the radiocarpal and intercarpal joints as well as the sheath of the flexor, the extensor tendons and abductor of the thumb (Figure 1).

The MRI examination shows the extension of tenosynovial chondromatosis.
The clinical results led us to hypothesize a case of extra-articular chondromatosis requiring surgical excision in order to complete the histopathologic evaluation.
After the excision of the dorsal wrist plane, we observed various gelatin-like foreign bodies originating from the tendon sheaths. The latter showed hyperplasia of the synovial tissue. Because of the difficulty in carrying out a complete excision of the numerous nodules, we performed a second surgical step using the volar access to complete the excision and radical synovectomy (Figure 2).

The dorsal access shows gelatin-like foreign bodies originating from tendon sheaths.
The histopathologic examination confirmed the diagnosis of extra-articular chondromatosis highlighting macroscopically various gray-white neoformations composed of hyaline cartilage of 5–0.6 cm in diameter. As far as the microscopic picture was concerned, we found hypertrophic-hyperplastic process and regressive phenomena on synovial membranes as well as the presence of chondrocytes of various dimensions with round, increased volume to double size nuclei. Furthermore, the histologic evaluation showed nodules surrounded by the tenosynovial membrane. These lesions composed of cellular and lobular growth characterized by tissue islands of hyaline cartilage metaplasia in synovium. Microscopically, we observed both mature and immature cartilaginous tissue apposition in foci surrounded by fibrous tissue and linked to synovial tissue (Figure 3).

Histopathologic section shows nodules of cartilaginous tissue.
Two years of follow-up did not reveal any post-surgery complications, reoccurrence of pathology without pain or main functional limitation of wrist (Figure 4). The patient was given the Disability of the Arm, Shoulder and Hand questionnaire (DASH) test. The score was 36. 10
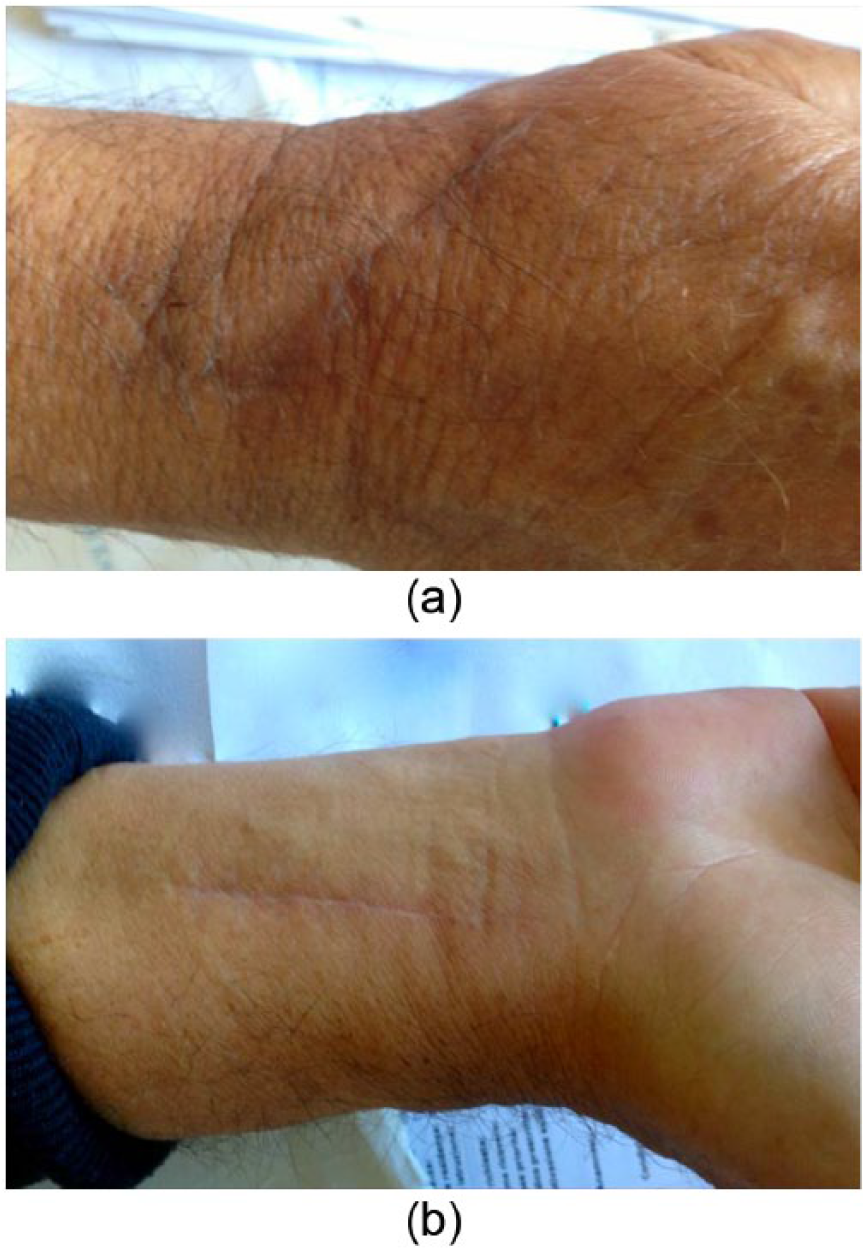
The images show the double surgical access at 2 years of follow-up. (a) excision of the dorsal wrist plane; (b) excision of the volar wrist plane.
Discussion
The chondromatosis is a rare benign disease characterized by multiple cartilage neoformations in the subsynovial articular tissue. Generally, it is mono-articular and affects, in order of frequency, the knee, the hip, the shoulder and the ankle joints while it is uncommon in small diarthrodial joints.3,11
The first step of the pathological process on the affected joints is neoplastic proliferation of the cartilage tissue with hyperplasia in synovial and cartilage nodules defined as chondroma. 2 This process could affect primarily joint bursa or tendon sheaths. The latter is the particular point of our case. The extra-articular form prefers the wrist/hand or the foot/ankle structures and less often big joints such as the knee or hip.4,5,8,9
According to the data in the literature,1,5,6 we may note how this disease affects flexor tendons more frequently than extensors. In our patient, we observed the spread to both flexor and extensor tendon sheaths of the radiocarpal and intercarpal joints, probably linked to the lesion dimension. This involvement of both compartments has never been written about in the literature.
Clinical diagnosis is not simple because tests often do not give any clear evidence. The most common symptoms are swelling with pain, deformities of the phalanges and reduced joint function caused by compression of nearby structures.8,12 Sometimes the clinical picture is silent since there may be no pain or functional limitation but only a lot of swelling without any history of trauma as was the case for our patient. After the clinical diagnosis, we proceeded to instrumental evaluation.
X-ray examination showed hyperdiaphonia near the joint with multiple calcific ossified nodules. 4 Occasionally, we may see a lot of nodules that, together, form one big multilobate nodule with osteolysis of the bone structures near the joint. This may also happen with periosteal chondroma and so complicates the diagnosis. The lack of ossification/calcification of the nodules at the beginning of the disease also complicates the traditional X-ray diagnosis;7,9 however, our X-ray examination did not reveal any alteration. Our MRI examination, however, showed disease of the soft tissue. MRI is, therefore, very useful not only for the diagnosis but also to clarify the extension of lesion prior to surgery.4,6,9
Histological tests are, however, necessary to confirm without any doubt the type and nature of the lesion. In our case, the macroscopic test revealed gray-white nodules of various dimensions, from a few millimeters to some centimeters, composed of hyaline cartilage. Microscopically, we observed several chondrocytes with different grades of cellular atypia, bundling nuclear and hyperchromasia without malign aspects. As regards etiology aspect, there emerges a debate in the literature. Whether synovial chondromatosis is a neoplastic process or a reactive metaplasia degeneration is unknown. This debate is due to histologic common features (enlarged chondrocytes, hypercellularity and metaplastic cartilaginous foci). 2 According to cytogenetic work, the neoplastic hypothesis is supported. In fact, this process is characterized by subsynovial cartilage neoplasia, hyperplasia of synovia and cartilaginous nodules formation. 2
The treatment of extra-articular chondromatosis is essentially surgical and consists of the complete excision of the neoformation and synovia. Complete excision prevents the disease from reoccurring.6,12–14 Due to the particular extension of the neoformation in our case, it was necessary to perform double access surgery on both the dorsal and volar plane of the wrist to ensure complete removal of the lesion. Double access for such a condition has never been described before in the literature and this is what makes this case unique.
This pathology in the wrist is very rare and has never been dealt with in the literature before now. Notwithstanding the swelling and the spread of the disease in two compartments, the clinical picture was without pain. In the end, we had to perform double surgical access and the successful outcome means we can recommend this surgical choice.
The limitation of the case report is the lack of preoperative DASH score with a specific test to evaluate two tendon compartments independently.
Footnotes
Acknowledgements
The authors thank Mrs Catriona mMacleod, BA, and Mr Brian John Molloy, BA, for language revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.