
Abstract
The presentation of cerebral venous sinus thrombosis may be acute or chronic with a progressive clinical course. The diagnosis can be challenging, and there are several clinical syndromes associated with the disease. It is also an uncommon but recognised complication of homocystinuria. We describe a case where early anticoagulation, together with dietary intervention, was associated with a favourable clinical outcome.
Vascular occlusion, both arterial and venous, is the leading cause of morbidity and mortality in untreated patients with homocystinuria (HCU) due to cystathionine β-synthase (CBS) deficiency. 1 The probability of suffering from a vascular event is 30% before the age of 20 years and rises to 50% before the age of 30 years in untreated patients. 1 Untreated patients have severe hyperhomocysteinaemia, hypermethioninaemia and hypocysteinaemia.
Cerebral venous sinus thrombosis (CVST) is an uncommon but recognised complication of untreated HCU. CVST may present with non-specific clinical manifestations including headache, focal neurological deficits and seizures, and may follow a progressive course. 2 We describe a patient with HCU, who developed seizures and an evolving left hemispheral syndrome secondary to CVST and discuss the role of homocysteine-lowering therapy and early anticoagulation in achieving a good clinical outcome.
Case report
A 24-year-old man presented with sudden onset of transient right upper limb paraesthesia and weakness associated with transient numbness on the right side of the tongue. There was a history of severe left parieto-occipital headache 3 days earlier. He had been previously diagnosed with pyridoxine non-responsive HCU through newborn screening and had been commenced on a methionine-restricted, cystine-supplemented diet within 6 weeks of birth. 3 He was a known compound heterozygote for c.919G>A, p.(Gly307Ser) and c.785C>T, p.(Thr262Met) of the CBS gene and had no other recognised complications of HCU. 4 Dietary compliance to treatment had initially been good but gradually deteriorated in the 6 years prior to presentation as reflected by infrequent blood sampling and rising free homocystine levels (Figure 1).

(a) Sagittal T1-weighted image shows increased signal from subacute thrombus in the superior sinus, (b) sagittal 2D PC MRV shows absence of signal from the anterior two-thirds of the superior sagittal sinus due to occlusion and (c) sagittal 2D PC MRV shows recanalisation of the superior sagittal sinus at 6 months follow-up.
Initial clinical evaluation
Physical examination on admission to hospital revealed a right upper motor neuron seventh nerve palsy, mild right upper limb weakness and a right extensor plantar response. Over the next 24 h, he developed a generalised tonic clonic seizure followed by deterioration in his level of consciousness, aphasia and an evolving right hemiparesis, more marked in the upper rather than lower limb.
Clinical investigations
Free homocystine (fHcy) and total homocysteine (tHcy) levels on admission were markedly elevated at 86 and 290 μmol/L (normal: 0 and <15; Figure 2), respectively. The corresponding methionine was elevated at 102 μmol/L and cystine was low at 22 μmol/L. Initial serum B12 and folate levels were normal. His coagulation profile was within normal limits. Previous thrombophilia screen by mutational analysis including factor V Leiden, thermolabile methylenetetrahydrofolate reductase and prothrombin 20210 A was negative.
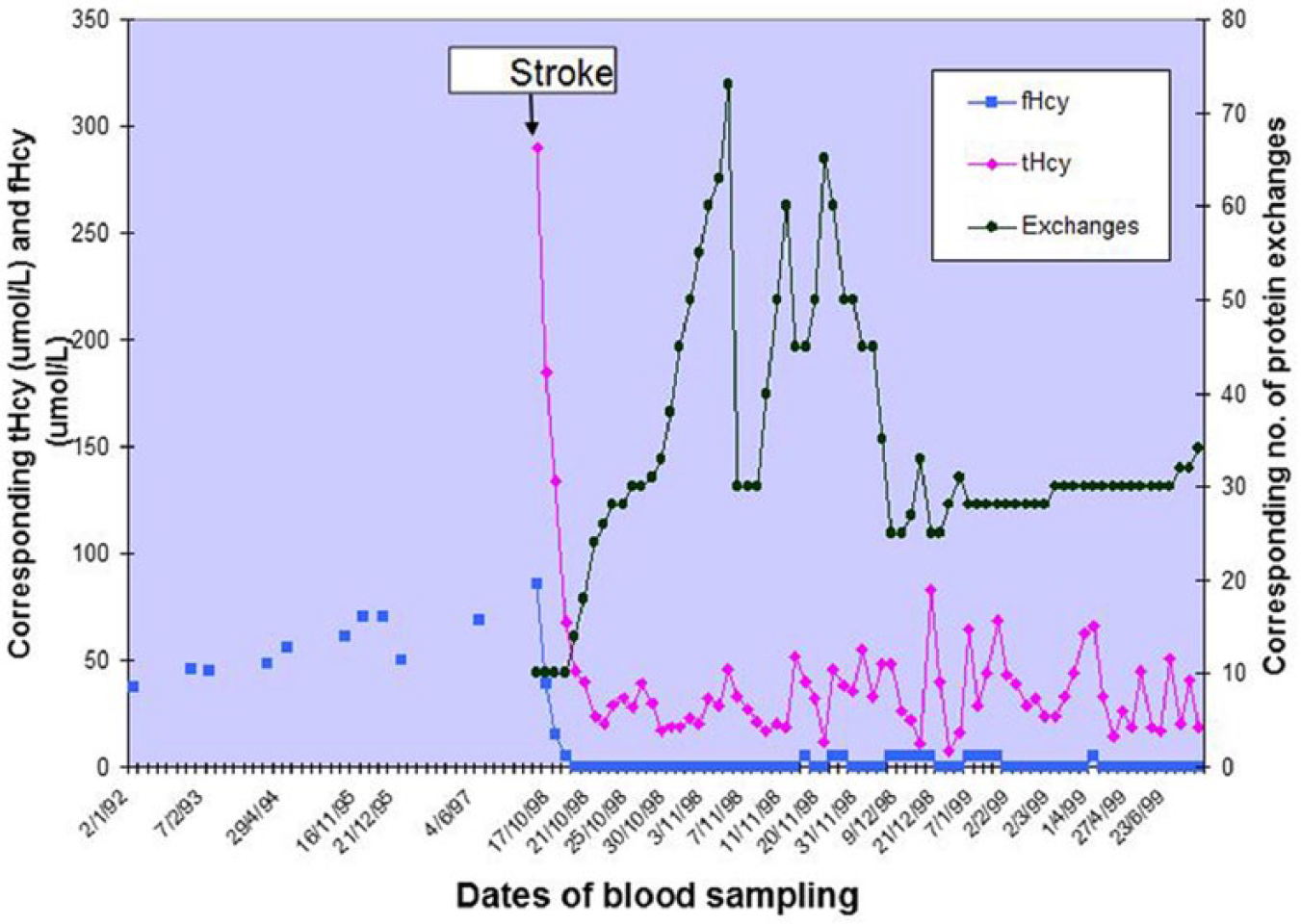
Dietary natural protein intake with corresponding total and free homocysteine levels.
Computed tomography (CT) of brain showed scattered areas of high attenuation over both parietal para-sagittal convexities with oedema of the left hemisphere. A sagittal T1-weighted MRI of brain showed increased signal in the superior sagittal sinus anteriorly (Figure 1(a)), corresponding to an absence of signal from the anterior two-thirds of the sinus on two-dimensional phase-contrast magnetic resonance venography (2D PC MRV; Figure 1(b)). There was no evidence of venous infarction on MRI despite the focal neurological findings.
Management
He was commenced on anticonvulsant therapy and anticoagulated with intravenous heparin followed by warfarin to maintain an International Normalised Ratio (INR) of 2–2.5 times normal. His normal dietary (natural) protein was stopped to reduce serum homocysteine levels. It was gradually reintroduced and titrated to maintain serum-free homocystine < 5 μmol/L and total homocysteine < 50 μmol/L (Figure 2). He stabilised at a tolerance of 30 g of dietary (natural) per day. A synthetic methionine-free, cystine-supplemented amino acid mix was given at 1 g/kg body weight. Supplementation of cofactors involved in the metabolism of methionine included pyridoxine (B6) 200 mg three times daily, folic acid 2.5–5 mg daily and vitamin B12 4 μg three times daily. A remethylating agent, betaine anhydrous 2 g three times daily, was given to remethylate homocysteine to methionine. A caloric intake of 3000 kcal/day was prescribed to prevent catabolism and minimise hyperhomocysteinaemia.
Clinical course and outcome
There was resolution of his aphasia and facial weakness with almost full recovery of right upper limb strength within 24–36 h of commencement of anticoagulation and dietary therapy. His clinical course was punctuated by transient episodes of dysarthria and right upper limb numbness. Although the response of these events to phenobarbitone was suggestive of focal seizure activity, an electroencephalogram (EEG) showed no focal discharges. A repeat MRI brain showed no extension of the thrombus.
Serum-free homocystine and total homocysteine were reduced to <5 and <50 μmol/L, respectively, from day 3 of admission and have been maintained at this level (Figure 2). He was discharged well with an INR of 2–2.5 times normal and remain anticoagulated for 1 year after the event. He has regained full neurological function and remains asymptomatic and with good HCU biochemical control, for a follow-up period of more than 10 years. A repeat MRI/MRV brain at 6-month follow-up revealed complete recanalisation of the superior sagittal sinus (Figure 1(c)).
Discussion
Venous thrombosis is by far the most common cause of vascular events in HCU. 1 It may be the presenting feature 2 or may occur in established disease, as illustrated by our patient. CVST in a young person without obvious thrombophilic tendencies should raise the diagnosis of HCU. Similarly, a diagnosis of CVST should be particularly considered in those with established HCU.
The diagnosis of CVST may be missed as the spectrum of presentation is extremely variable and can be misleading. Its course is unpredictable with the possibility for sudden deteriorations. Thus, the first step in successful management is to suspect and recognise the condition. Untreated or poorly controlled HCU patients have a predeliction for venous thrombosis, and a high index of suspicion for CVST is required.
The rationale for anticoagulation in CVST is to prevent propagation of thrombus and involvement of cortical veins. Caution has been exercised in the past because of the attendant risk of haemorrhagic infarction. The use of anticoagulation in CVST, however, is currently supported by many studies. 5 The early institution of anticoagulation in our patient and the subsequent clinical response support this view.
An important aspect of the management of this case was the early institution of appropriate homocysteine-lowering dietary therapy. Other dietary modifications included the provision of metabolic cofactors, a remethylating agent and adequate calories to prevent catabolism and hyperhomocysteinaemia. It is essential to maintain free homocystine <5 μmol/L and total homocysteine <50 μmol/L consistently throughout life so that the risk of a recurrent vascular event is minimised. The precise pathophysiology of thrombus formation in HCU patients is not known but is presumed to be due to prolonged elevation of these parameters. While the rationale for anticoagulation is to prevent thrombus propagation, the role of dietary therapy is to prevent (de novo) thrombus formation.
HCU patients represent an important subgroup of CVST cases, albeit a rare risk factor. The successful management of this patient suggests that it is the combination of effective dietary intervention and early anticoagulation which was pivotal for a favourable outcome.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of Dr Eileen Naughten, who is retired; the dieticians: Margery Kellett, Dearbhla Hunt (National Center for Inherited Metabolic Disorders) and Marie Gorman (Beaumont Hospital), the MRI radiographers (Beaumont Hospital), laboratory staff, nursing, physiotherapy and psychology colleagues of both hospitals for their contribution to the care of the patient reported here. S.Y. was responsible for the metabolic management of the patient, collated the data and drafted the manuscript; D.A.-W. provided radiological advice; O.H. was responsible for the neurological management of the patient.
Authors’ Note
Sufin Yap was previously affiliated to National Centre for Inherited Metabolic Disorders, Children’s University Hospital, Dublin, UK, where the patient was treated and followed up.
Declaration of conflicting of interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.Y. has received honoraria from Orphan Europe.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.